
記住我




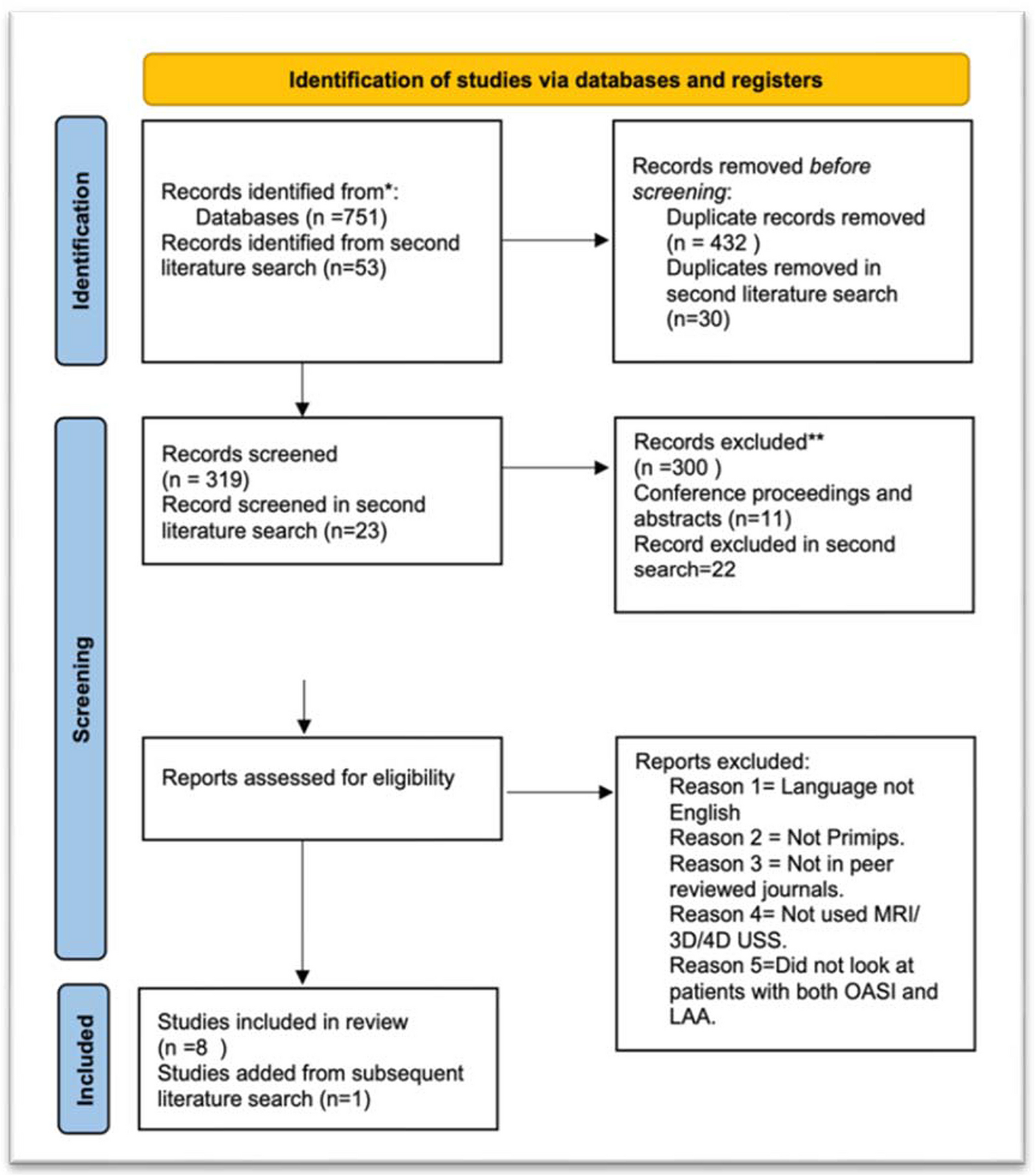


The PRISMA flowchart of the study is summarized in Fig. 1, and the process of the modified Delphi method is depicted in Fig. 2. Table 1 shows the percentage of agreement for each round for items that did not reach consensus after round 1, and Table 2 summarizes the recommendations.
Fig. 1
PRISMA flowchart of the systematic review of the literature
Fig. 2
Process of the modified Delphi method for the development of the present consensus ERAS guidelines for perioperative care for liver surgery
Table 1 Percentage of agreement (regarding summary, level of evidence, and grade of recommendation) after the different Delphi rounds for items that did not reach consensus (< 80% agreement) after the first roundTable 2 Summary of ERAS recommendations for liver surgery for each item, including the levels of evidence and the grades of recommendationPreoperative counselingNo RCT assessing preoperative counseling specifically in liver surgery exist. A recent RCT (PEDUCAT trial) compared a 1-h preoperative counseling and information seminar associated with brochure to brochure only with standard management (control group) in major abdominal surgery, including 25 liver resections [11]. No difference in complications or mortality was observed between both groups except for hospital falls, which were more frequent in the control group. Moreover, no difference in patient satisfaction was found. The preoperative information seminar was nevertheless beneficial for the training of patients and nursing staff. In one study, a mobile application for hepatopancreatobiliary (HPB) surgery within an ERAS pathway containing preoperative information was developed and was found to be feasible [12]. A systematic review on preoperative information before elective surgery did not show any differences in terms of perioperative anxiety and postoperative outcomes between specific formats and timings [13].
Summary and recommendation: Patients should receive preoperative information and counseling regarding the upcoming liver surgery. Brochures and multimedia supports might help to improve the verbal counseling.
Evidence level: Low.
Grade of recommendation: Weak.
PrehabilitationTwo recent systematic reviews (including 419 and 1377 patients) focusing on prehabilitation for liver surgery have been published [14, 15]. Both found no difference in terms of postoperative complications and LoS. Only a trend toward less postoperative complications and shorter LoS was found in the pooled analysis of the systematic review by Dewulf et al. [15]. Both reviews underlined that several included studies were underpowered and that standardized outcome measures should be defined in future analyses. A narrative review on prehabilitation for patients with steatosis suggested that the 4–6-week period before the operation could be used for prehabilitation including dietary intervention to decrease intrahepatic fat and improve postoperative outcomes [16]. Another further narrative review on older patients recommended a focus on high-risk patients who could benefit from prehabilitation [17]. Aging is often associated with sarcopenia and malnutrition, rendering these patients more at risk of a complication [17]. Frail patients might therefore benefit the most from prehabilitation [17]. In their review, Walcott-Sapp and Billingsley [18] recommended that candidates for major liver resection should have their nutritional and functional status evaluated preoperatively and improved if necessary. Two RCT on prehabilitation in liver surgery have been performed [19, 20]. One study, including a total of 51 patients, found that postoperative complications were similar but that serum insulin levels were decreased and anaerobic threshold increased in the prehabilitation group [19]. The other RCT of 35 patients found an improvement in cardiopulmonary testing and quality of life in patients who had prehabilitation [20]. Two other studies specific to liver surgery (one prospective study and one propensity score matching study) found improved outcomes in the prehabilitation group (decreased complications and LoS) [21, 22]. Nine systematic reviews and meta-analyses on major abdominal surgery found globally that postoperative complications were reduced in patients having prehabilitation but heterogeneity of the included studies was high and quality of the evidence low [23,24,25,26,27,28,29,30,31].
Summary and recommendation: Prehabilitation should be performed in high-risk patients (elderly, malnourished or overweight patients, smokers, or patients with psychological disorder) prior to liver surgery. Prehabilitation should be commenced 4–6 weeks before the operation depending upon the urgency of surgery. The content (physical exercises, dietary interventions, or anxiety reduction exercises) and duration of the prehabilitation program for liver surgery are not clearly established.
Evidence level: Moderate.
Grade of recommendation: Weak.
Preoperative biliary drainage (PBD)The results of 2 meta-analyses showed that the mortality rate was similar between patients with or without PBD for perihilar cholangiocarcinoma, but that PBD increased the incidence of complications such as pancreatitis, cholangitis, and surgical site infection (SSI) [32, 33]. In the meta-analysis by Moole et al. [34], PBD was associated with fewer overall major adverse events than surgery itself, especially in patients undergoing endoscopic PBD. Moreover, PBD has been proven beneficial in the presence of cholangitis, severe malnutrition, and coagulation abnormalities [35]. Most reports have described PBD on the future liver remnant side. Prolonged preoperative jaundice was associated with increased postoperative morbidity and mortality after hepatic resection because of severe cholestatic liver dysfunction [36]. Regarding hilar cholangiocarcinoma, an expert consensus statement (American Hepato-Pancreato-Biliary Association-sponsored consensus meeting) recommended PBD in patients with cholangitis, hyperbilirubinemia-induced malnutrition, hepatic insufficiency, or renal insufficiency and in patients undergoing preoperative chemotherapy or portal vein embolization [37].
Endoscopic biliary drainage (EBD) and percutaneous biliary drainage (PTBD) for hilar tumors are the 2 main strategies of PBD. According to different meta-analyses, PTBD is associated with a lower rate of complications such as pancreatitis and cholangitis than EBD, and PTBD has a higher therapeutic success rate than EBD [38,39,40]. Conversely, a meta-analysis by Wang et al. [41] showed that the incidence of seeding metastasis was significantly higher in the PTBD than EBD group, and EBD was superior to PTBD in terms of overall survival in patients with resectable perihilar cholangiocarcinoma.
Neither the timing of surgery nor the duration of PBD has been defined. Most institutions define these parameters based on the serum bilirubin concentration, which also shows variance. Some centers recommended PBD duration until the bilirubin level is <2 to 3 mg/dl (about 30–50 mmol/l) [37]. Only one study has assessed the optimal interval between PBD and liver resection [42]. Son et al. [42] classified patients into either a long-term (≥2 weeks) or a short-term (<2 weeks) group. They showed that PBD <2 weeks before surgery was associated with significantly fewer PBD-related complications after resection.
Summary and recommendation: Biliary drainage in cholestatic liver (>50 mmol/l) is recommended. For perihilar cholangiocarcinoma, percutaneous biliary drainage should be preferred to endoscopic biliary drainage. Surgery should ideally not be performed until bilirubin level drops below 50 mmol/l.
Evidence level: Moderate.
Grade of recommendation: Strong.
Preoperative smoking and alcohol cessationSmoking is a risk factor for overall complications, SSI, pulmonary complications, neurological complications, and admission to the intensive care unit after surgery [43]. Lv et al. [44] showed in a retrospective study of 425 patients that smoking was an independent risk factor for liver-related and infectious complications after hepatectomy in patients with hepatocellular carcinoma (HCC). No prospective study specific to smoking cessation and liver surgery has been published yet. Two older RCT found a benefit of preoperative smoking cessation in terms of complications before various types of operations [45, 46]. A systematic review of 25 articles published in 2012 confirmed that smoking cessation at least 4 weeks before surgery reduced the risk of respiratory and wound-associated complications [47]. Conversely, smoking cessation less than 4 weeks prior surgery did not improve postoperative outcomes. A Cochrane systematic review published in 2014 including 13 RCT found that an intensive intervention for smoking cessation prior to surgery reduced postoperative complications compared to no intervention (risk ratio 0.42) [48]. Two retrospective studies also suggested that smoking was a risk factor for higher recurrence and liver-specific mortality after hepatectomy for HCC [49, 50].
In a systematic review with meta-analysis including 55 studies, alcohol was found to be an independent risk factor for overall, infectious, and respiratory complications after surgery [51]. Nevertheless, low-to-moderate alcohol consumption was not associated with postoperative morbidity but data remained scarce [51]. In liver surgery, alcoholic hepatitis is a risk factor for postoperative complications [52]. Alcohol consumption should therefore be reduced and ideally stopped in the perioperative period.
Summary and recommendation: Preoperative smoking cessation should be counseled at least 4 weeks prior to hepatectomy. Alcohol cessation is recommended for heavy drinkers (>24 g/day for women or >36 g/day for men) 4–8 weeks before surgery.
Evidence level: Smoking: high, alcohol: high.
Grade of recommendation: Smoking: strong, alcohol: strong.
Preoperative nutritionPrior to hepatic surgery, a nutritional risk screening is required to determine patients at higher risk of postoperative complications. Numerous nutritional screening tools have been validated [53]. Multiple meta-analyses have prognosticated nutritional scoring systems utilizing a combination of serum albumin and lymphocyte count (prognostic nutritional index) [54, 55] and, in addition, serum cholesterol (controlling nutritional status score) [56] in patients undergoing hepatectomy for HCC.
Delaying surgery to optimize preoperative malnutrition (body mass index, BMI <18.5 kg/m2) and disease-related malnutrition (weight loss >10% or >5% over 3 months and reduced BMI or a low fat-free mass index) is necessary [57]. A number of adverse outcomes have been associated with poor perioperative nutrition, including septic complications [58, 59]. Perioperative enteral nutritional therapy should be utilized for a period of 7–14 days in such patients, preferably in an outpatient setting [57]. Parenteral nutrition should only be considered in patients where requirements cannot be met by enteral nutrition alone [57]. A single RCT has demonstrated that intraoperative blood loss can be minimized in obese patients undergoing hepatectomy by introducing a low-fat, low-calorie diet one week prior to surgery [60].
Summary and recommendation: A nutritional assessment is necessary prior to all hepatic surgery. Malnourished patients (i.e., weight loss >10% or >5% over 3 months and reduced body mass index or a low fat-free mass index) should be optimized with enteral supplementation at least 7–14 days prior to surgery.
Evidence level: High.
Grade of recommendation: Strong.
Perioperative oral immunonutritionImmunomodulation through the use of branched-chain amino acids (BCAA), L-arginine, omega-3 fatty acids, and nucleotides has been reported to control inflammation, prevent immunosuppression, and thus reduce postoperative sepsis [59, 61].
The reduction of inflammation and improvement in hepatic function as a result of immunonutrition may improve outcomes. Omega-3 fatty acid administration has been associated with a reduction in infections and improved liver functions in patients undergoing hepatic resection [62]. Yang et al. [63] suggested that omega-3 fatty acid administration in rats undergoing large hepatic resection reduced hepatic fibrosis and improved hepatic regeneration. Akbari et al. [64] failed to demonstrate this benefit in rats, although the hepatic resections were significantly smaller. Beppu et al. [65] concluded that BCAA supplementation in humans was beneficial in hepatic regeneration after portal vein embolization.
A few systematic reviews suggested promising results. Decreased postoperative complications, improved nutritional state, and shortened hospitalization have all been demonstrated [59, 66]. Numerous biochemical parameters (alanine aminotransferase, aspartate aminotransferase, white cell count and pre-albumin) have been used and have demonstrated a benefit of omega-3 fatty acids in hepatic surgery [67]. None of these beneficial aspects have shown any improvement in postoperative mortality [59, 66,67,68]. McKay et al. [59] noted that the majority of RCT in their systematic review were of poor quality. More recent RCT failed to demonstrate a benefit for immunonutrition in elective hepatic surgery [69, 70].
Ichikawa et al. [71] demonstrated an oncological benefit for the use of BCAA. Tumor recurrence (at 30 months) as well as alpha-fetoprotein (at 36 months) was significantly reduced as a result of BCAA use; however, overall mortality was unaffected.
The European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines currently do not support the use of glutamine, arginine, and omega-3 fatty acids in well-nourished patients; however, supplementation may be indicated in malnourished patients or patients that are unable to be fed enterally [57].
Summary and recommendation: Due to the lack of evidence, the use of immunonutrition in hepatic surgery is not recommended yet.
Evidence level: Low.
Grade of recommendation: Weak.
Preoperative fasting and preoperative carbohydrate loadThe ESPEN and the American Society of Anesthesiologists guidelines currently recommend fasting for solids for 6 h before anesthesia and for liquids no more than 2 h before anesthesia [57, 72].
The purpose of giving carbohydrate drinks the evening before and 2–4 h before surgery is to ensure hydration and to reduce insulin resistance [73, 74]. Preoperative carbohydrate drinks have been associated with reduced anxiety, postoperative nausea and vomiting, postoperative insulin resistance, and length of hospitalization [57]. Preoperative carbohydrate loading reduces the resistance to insulin after liver surgery [75,76,77]. Moreover, Kobayashi et al. [78] found that giving late-evening carbohydrate load and an amino acid snack preoperatively improved the nutritional status of patients with perturbation of liver function. A Cochrane meta-analysis found that carbohydrate loading before elective surgery (18 studies for abdominal surgery) allowed a small reduction of LoS [79]. No difference in terms of complications was found. In a network meta-analysis published in 2017, carbohydrate loading before surgery was associated with a reduction of LoS in patients who were fasting, but did not show any benefit compared to water or placebo [80]. A 2010 RCT on major abdominal surgery (including liver surgery) found that preoperative carbohydrate loading did not improve postoperative outcomes [81]. However, patients with carbohydrate loading who underwent open surgery without epidural analgesia had a trend toward a shorter median LoS (7 vs. 9 days, p = 0.054) [81]. A recent systematic review of RCT in general surgery concluded that carbohydrate loading up to 2 h prior to surgery was safe and could decrease insulin resistance [82]. Some data support the deleterious effect of insulin resistance on liver regeneration [83]. Type 1 diabetes or active gastroesophageal reflux is relative contraindication to carbohydrate loading in the 2–4 h period before surgery although type 2 diabetes can receive it [84].
Summary and recommendation: Preoperative fasting of 2 h for liquids and 6 h for solids before anesthesia is safe and can be recommended. Carbohydrate loading is recommended the evening before liver surgery and 2–4 h before induction of anesthesia. Preoperative carbohydrate loading is safe and improves perioperative insulin resistance, but it is not clear if it is associated with a reduction of length of stay in liver surgery.
Evidence level: Preoperative fasting: moderate, carbohydrate loading: low.
Grade of recommendation: Preoperative fasting: strong, carbohydrate loading: weak.
Pre-anesthetic medicationPre-anesthetic medication has traditionally been given to allay anxiety, but long-acting agents impair psychomotor recovery after general anesthesia. A Cochrane review on anxiolytic premedication for outpatient surgery showed that patients who received oral anxiolytics had psychomotor function impairment 4 h after surgery, reducing their ability to ambulate, eat, and drink [85]. In selected cases, short-acting anxiolytics (such as 1–2 mg midazolam) can be given to ease regional anesthesia before general anesthesia induction. The American Geriatrics Society Beers Criteria for potentially inappropriate medication use in older patient populations (aged 65 years and older) strongly advise against using benzodiazepines as they may cause cognitive impairment and increase the risk of delirium and falls in the elderly [86].
More recently, preoperative medication was more commonly used as perioperative multimodal analgesic adjuncts. In liver surgery, the use of nonsteroidal anti-inflammatory drugs (NSAIDS) preoperatively is not recommended because of the risk of acute kidney injury. A meta-analysis of 281 trials (n = 24,682 participants) examining the use of gabapentinoids in major surgery showed that although there was a mild analgesic effect, there were significant problems with blurred vision and dizziness [87]. These appeared to be dose-related but could occur with normal dosing in the elderly, so their use in liver surgery was not recommended. Acetaminophen has to be dose-adjusted if significant liver parench
留言 (0)