
記住我






The study is an open-label, two-arm randomized controlled trial with equal allocation between intervention and waiting list control arm. The psychoeducation intervention will comprise 8–12 sessions given over 12 weeks with assessments of outcomes at baseline, end-study, and at 3rd and 12th months follow-up of the study. An illustration of recruitment numbers, scheduled enrolment, interventions, and assessments is provided in Fig. 1.
Fig. 1
Planned flow chart of participants through the trial
Study settings and participantsParticipants diagnosed with BD type I or II were recruited from the two referral hospitals with mental health capabilities in Rwanda; CHUK and CARAES-Ndera Hospital.
CHUK is the largest referral hospital in Rwanda, located in the District of Nyarugenge, Kigali City. The hospital does not provide inpatient care for psychiatric patients, yet it is the second biggest outpatients’ mental health clinic besides CARAES-Ndera Hospital. The CHUK Mental Health Department offers a range of care and treatment for people experiencing common mental health disorders such as depression, bipolar disorders, psychotic disorders, panic and anxiety disorder, obsessive-compulsive disorder, and post-traumatic stress disorder (http://chuk.rw/about-chuk).
CARAES-Ndera Hospital is a mission health facility and the sole neuropsychiatric hospital in the country with inpatient care that offers specialized healthcare in psychiatry and neurology. The Hospital is located 17 kilometers from Kigali City, in Gasabo District (https://www.CARAES-Nderahospital.rw/1/overview).
Inclusion criteriaA diagnosis of BD type I or II that meets DSM-V given by a trained psychiatrist
Adults (18 years or older)
Signed informed consent provided
Exclusion criteriaPatients in a current depressive (above or equal to 17 on the Hamilton Depression Scale-17) or hypomanic- or manic phase (scores above or equal to 12 on the Young Mania Rating Scale)
Previous participation in any structured psychological intervention, such as psychoeducation or cognitive remediation
Mental retardation stated in medical records
Current alcohol or drug-use disorder
Insufficient understanding of Kinyarwanda
Deafness
Lack of informed consent
Recruitment proceduresClinical staff members at the two referral hospitals assisted in the recruitment of participants during their clinical work. Participants who had been in contact with the mental health department within the last year were prioritized.
The interventionParticipants will be divided into groups of 8–10 members. Each psychoeducation group will have two facilitators, one psychologist, and one mental health nurse. The facilitators will get training on how to facilitate group psychoeducation through workshops and seminars.
With the permission already obtained from Professor Mark S. Bauer, the structured manual will be inspired by the Life Goal Program by Bauer et al. [20, 22] but will need cultural adaptation to the Rwandese setting. For further information regarding the Life Goal Program, please refer to www.lifegoalscc.com/overview, where a new modular form can be found and utilized, without charge.
Planned focus group discussions and in-depth interviews have been conducted and assisted the transcultural adaptation of the program, which in turn ensured the involvement of patients. The participants of the focus groups will be former participants and facilitators in the psychoeducation program from 2014. In-depth interviews will be held with naive psychoeducation participants focusing on the living experience of BD in Rwanda. A total of 8–12 sessions are expected to be included in the final manual. Following the finalization of the intervention, subsequent evaluation interviews will be conducted with study participants. The adapted manual utilized in the intervention will be made in the language Kinyarwanda and translated into English by a professional translator.
Waiting list as the control groupAs a control group, we will use the “Early intervention versus delayed intervention strategy”. The participants randomized to the waiting list will do their group psychoeducation 12 months after the intervention group; consequently, they will be used as the control group. Evaluations and assessments will be done in parallel with the intervention group at the screening day, three months after the group psychoeducation, and 12 months after the intervention. While waiting, the participants on the waiting list will receive the standard treatment care, which in Rwanda, mainly consists of taking prescribed medication from the outpatient clinic.
Primary and secondary outcomesAll outcomes have been assessed at baseline and will be assessed at the first evaluation, which will take place immediately after 8–12 sessions of group psychoeducation (the intervention), then at the 3rd and 12th months follow-up. The outcomes are based on the most commonly used measurements for trials on psychoeducation for individuals with BD in high and middle-income countries [18, 19].
Baseline dataThe Mini-International Neuropsychiatric Interview (MINI) [23] was applied to confirm the psychiatric diagnosis. Demographic information regarding the participants’ living circumstances, past psychiatric history, and the use of mental health service data was collected from interviews. Finally, past traumatic events and history of suicidal behaviors were recorded using Life Event Checklist for DSM-5 (LEC-5) [24] and The Columbia-Suicide Severity Rating Scale (C-SSRS) [25].
Primary outcomesRelapse is defined as hospitalization or a new mood episode, such as mania when the participant scores above or equal to 20 on the Young Mania Rating Scale (YMRS) [26] or hypomania when the score is above or equal to 12 on the YMRS. For depressive episodes, the score should be above or equal to 17 on the Hamilton Depression Scale-17 (HDRS-17) [27], and for mixed episodes, the scores should be above or equal to 20 on the YMRS and equal or above 12 on the HDRS-17.
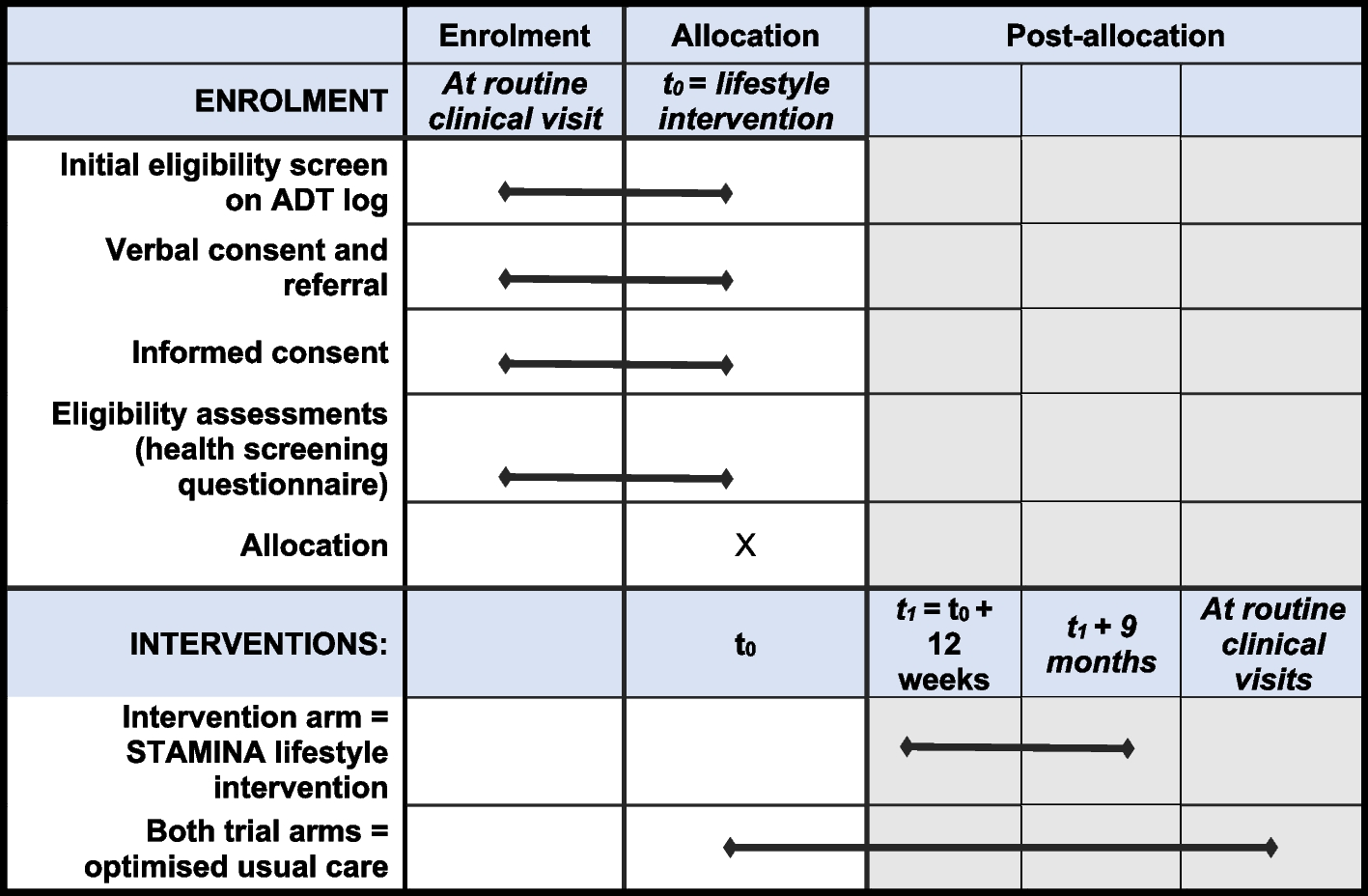
Secondary outcomesThe shortened version of the Clinical Global Impression Scale for Bipolar disorder (CGI-BP) will be used to assess improvement in symptom severity observed by the clinicians [28]. The Medication Adherence Rating Scale (MARS) will be used to evaluate medical adherence [29]. All participants filled in a knowledge test and questions about self-stigma, Internalized-Stigma of Mental Illness Scale (ISMI) [30], and suicidal thoughts before and after the psychoeducation. An illustrative overview is shown in Fig. 2: schedule of enrolment, interventions, and assessments.
Fig. 2
SPIRIT figure. Schedule of enrolments, intervention, and assessments
The only validated tools in Kinyarwanda are the MINI, LEC-5, and the HDRS. In parallel, data collection is ongoing in order to validate and culturally adapt the four remaining tools in Kinyarwanda.
Sample size calculationsIn the literature on group psychoeducation, 13 out of 18 RCTs have reduction in general psychiatric symptom severity, the incidence of relapse, and hospitalization as the main outcomes [18]. We reviewed 18 RCTs on group psychoeducation for BD before we selected a study by Colom et al. as the base of our power calculation [18, 31]. The incidence of relapse in the study was (92%) (55 subjects) in the control group vs. 67% (40 subjects) in the psychoeducation group. For our study, a sample size of 40 patients for each arm is required to achieve a level of 80% power with a 5% level of significance when comparing the mean change in each intervention with the control arm via a two-sample t-test. Adjusting for a drop-out rate of 20%, 40/(1−(20/100)), 50 participants will be needed for each group.
Randomization and blindingRandomization to either the intervention or the waiting list group followed immediately after baseline data collection. An independent statistician who is not involved in clinical assessments generated the randomization procedure. The allocation sequence was implemented using the REDCap (Research Electronic Data Capture) electronic system with a ratio of 1:1 and a block size of 4 and 6. When a patient was found eligible for inclusion by the clinical staff and signed the consent form, a third party who was not a part of the clinical staff at the hospital accessed the REDCap system, where the computer generated the allocation. Blinding of participants and clinicians is not possible due to the nature of the treatment intervention.
Adherence to the studyBefore each session, facilitators will be calling the participants to remind them about the next psychoeducation session.
Data collection, management, and integrityTo ensure the safety and high quality of the data, the data collectors will receive intensive training on data collection and how to use the outcome tools.
All data will be entered and stored in the Electronic Data Capture system, REDCap. This system is compliant with the EU General Data Protection Regulation (GDPR) and Good Clinical Practice guidelines (GCP). The study adheres to all GDPR regulations. A trial ID will be assigned to all participants, and personal information will be stored securely and separately. Data will be entered directly into electronic Case Report Forms (CRF) using REDCap. Questionnaire data will be filled out manually and entered directly into REDCap by the research assistants and the investigators at baseline and follow-up. If access to the REDCap system is not possible, data will be collected on paper CRF and entered into REDCap when access has been restored. The research team will regularly conduct quality checks and verification of entered data at the aggregated and individual participant levels. These checks include the identification of missing data, internal consistency, the range for data values, and obvious errors. Once a data collection form has been checked and verified, it will be locked for further editing. The hard copy questionnaires will be stored in the field office accessible by the two principal investigators.
Statistical analysisAll analyses will be carried out following the intention to treat principle, i.e., without regard to the compliance of individuals within their allocated study arm. Reasons for potential drop-outs will be accounted for and reported. Estimates of the effectiveness of the intervention and 95% confidence intervals will be adjusted for differences in baseline scores by analysis of covariance. Two-sided p values will be reported at a 95% confidence interval with a statistical significance level of less than 0.05. Continuous measures will be compared using t-tests, while binary outcomes will be analyzed using Chi-square or Fisher’s exact test if values are small. Multiple regression analysis will be performed to adjust for age, sex, and severity of illness. To check the robustness of the results, the primary outcome will also be analyzed using a per-protocol approach, including only participants who completed at least half of the psychoeducation sessions. Data analysis will be performed using STATA version 17 software (StataCorp, College Station, TX, USA).
Ethical considerationsThis study will be carried out in accordance with the Declaration of Helsinki. The study's ethical approvals have been granted by the University of Rwanda College of Medicine and Health Sciences-Institutional Ethical Review board and the CARAES-Ndera Hospital and University Teaching Hospital of Kigali-CHUK ethical review boards. Furthermore, the study investigators have obtained approval to carry out the research from the National Council for Sciences and Technology (NCST), as required for all researchers in Rwanda. Anonymity and confidentiality of participants will be ensured by assigning a study ID number to all participants. Informed consent will be obtained from all participants.
CompensationIt is anticipated from the experience of conducting psychoeducation in Rwanda for patients with BD that the trial brings nearly no risk to the study participants; for this reason, the study is without an insurance plan. As Rwandan regulation requires, each study participant will receive a small compensation — 10.000 Rwandan Francs — to cover their transportation expenses from their villages to the research venue.
Intervention fidelityThe fidelity of the study will be guaranteed, starting from the pre-intervention training of the facilitators. The facilitators will be explained the importance of enduring with all intervention constituents in the experimental arm. Moreover, the intervention will follow a structured guide manual that all facilitators will be trained in. Finally, participants’ attendance is registered after each psychoeducation session.
Dissemination planThe project aims to direct research and policy attention toward mental health globally and at national, and local levels. For the dissemination of the outcomes of the project, we will (a) publish articles in peer-reviewed scientific journals; (b) present results at international scientific meetings and conferences; (c) organize local meetings with key stakeholders during the full extent of the project; and (d) trial results will be communicated to participants in their routine clinical outpatient care.
The Vancouver rules for authorship will be followed. There will be no use of professional writers.
留言 (0)