
記住我




Chronic kidney disease (CKD) is a common lifelong disease in clinical science. It is prolonged and debilitating (1), posing a significant threat to public health. It has been estimated that there are more than 70 million CKD patients globally (2). According to the World Health Organization, 14 out of every 100,000 people will die from CKD in 2030. Patients with CKD must self-manage their illness to a large extent to slow disease progression (3). Lean implementation of chronic disease management (CDM) significantly benefits individuals, society, and the economy (4).
In general, there are four CDM models centered on CDM. Stanford model improves patient self-efficacy through a chronic disease self-management program (CDSMP) (5). The Flinders Model (FM) proposes that a patient is the ultimate decision-maker and emphasizes that doctors and patients make joint decisions and share responsibilities (6). Expert Patients Program (EPP) emphasizes that patients participate in medical decision-making and any self-management project to establish continuous feedback, evaluation, and assessment mechanism (7). The Chronic Care Model (CCM) emphasizes that patients should be involved in medical decision-making (8). The above CDM models show that patient self-management behaviors are crucial in optimizing diagnosis and treatment plans, ensuring patients' safety, and improving patient compliance with treatment (9). Self-management is generally defined as the daily management of chronic conditions by individuals during a period of the disease (10).
Although self-management behavior is a complex endeavor, which is influenced by the stage of the disease (11), demographic characteristics (12), and so on, with the joint participation of both medical staff and patients, it centers on the patient's sense of responsibility for their health, and requires the patient's adjustment and to control their behaviors (13), including beneficial behaviors such as daily diet, physical exercises, mental health, and disease treatment (14). Finally, it leads to a higher quality of life (15). Studies reported that the multiple self-management strategies adopted by chronic disease patients eventually follow a specific trend and pattern. These trends and patterns affect chronic disease progression (9). Patterns have certain differences (16). This is conducive to eliminating waste and improving medical efficiency and quality (17). Therefore, from the perspective of the influencing factors of self-management, self-management is not that patient finishing every management works by themselves, which need some lean support from the related stakeholders, such as a doctor, family, and society environment. So what kind of support should they offer from a broader?
This study identifies patient self-management behavior patterns to establish systematic lean healthcare support from the related stakeholders for chronic disease patients using data from patients' surveys. In the methodology, Behavior pattern recognition is to distinguish behavior differences from the environment and make decisions for different types of people (18), which aims to extract information features and classify them into different groups (19). In general, behaviors often have independent multi-attribute features; therefore, most studies use principal component analysis to reduce the dimensionality to extract key features (20) and recognize patterns (21). This study applied the Test and Principal component method to study Self-management behavior using the actual data survey of chronic disease patients.
The following contents of this study are organized as follows: Section Methods introduces methods, Section Results shows results, Section Discussion is the discussion, and Section Conclusions offers conclusions.
Methods Study designThis study used purposive sampling to enroll subject patients diagnosed with CKD in a general hospital in southwest China for one month. All of the included patients came from the CKD outpatient department. The estimated sample size in the empirical case was more than 100 subjects who could answer the survey questions face to face. Another inclusion criterion is that these outpatients had no disease progression, which can be a control variable to reveal some effective self-management behavior in the same disease group. This study enrolled the sample size of subjects to be not less than 130 subjects, thinking about a 30% questionnaire loss rate.
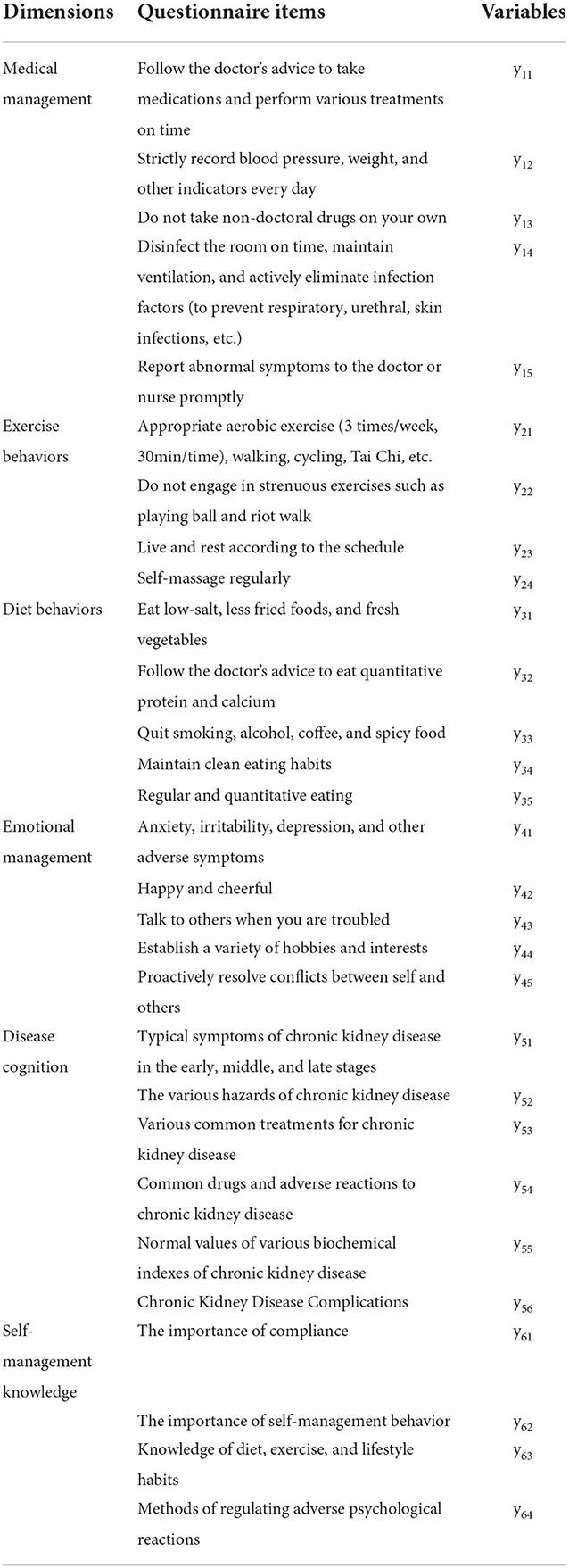
Behavior instrumentMost studies constructed an assessment scale for chronic disease self-management behavior based on some relevant theories in chronic disease self-management. Four self-management models, as mentioned before, put forward that different chronic diseases need to design with specific survey scales (22). The first part of the questionnaire is demographic characteristics designed for six items. The second part is based on the three major tasks of chronic disease self-management as daily life management, medical management of diseases, and emotional and cognitive management (23). This study designed six behavioral dimensions including 29 items, namely treatment management with five items, exercise behaviors with four items, diet behaviors with five items, emotional management with five items, disease cognition with five items, and self-management knowledge with five items. The questionnaire was scored using a five-point Likert scale, and each item was evaluated on an agreement scale of 1–5. Higher scores indicate preferring the self-management behavior of patients. These 29 items are all categorical variables, as shown in Table 1. The score variables of the six behavior dimensions are yij (i, jε(1…,6)).
Table 1. Questionnaire dimensions and items.
Ethical considerationsThis study was reviewed and approved by the ethics review committees of West China Hospital (2020-740). All participants provided informed consent before participation in the study. The research purposes and procedures were explained to each subject, and before the informed consent form was signed, each subject was informed that they could withdraw from the study at any time and that their rights would not be affected. They were also informed that the data obtained from the questionnaires would be provided only for educational use and would not be disclosed after the study was completed.
Data analysisA total of 131 valid questionnaires were distributed. The Cronbach's coefficient of each dimension of the questionnaire is greater than 0.7 databases, with high internal consistency. KMO values of all dimensions are greater than 0.7, with high validity. The encoded data were calculated and analyzed using the software SPSS 26.0. The statistical analyses included descriptive statistics, F-test, and principal component analysis for multiple variables. The F-test method was used to discriminate differences in self-management behavior dimension on demographic characteristics, which are control variables. α = 0.05 is the test level, and the P-values are two-sided probabilities.
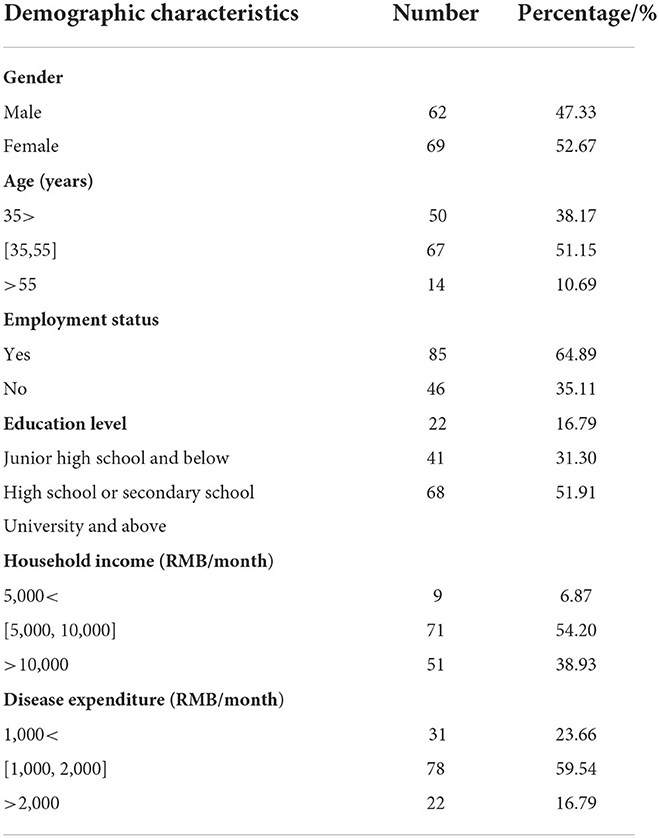
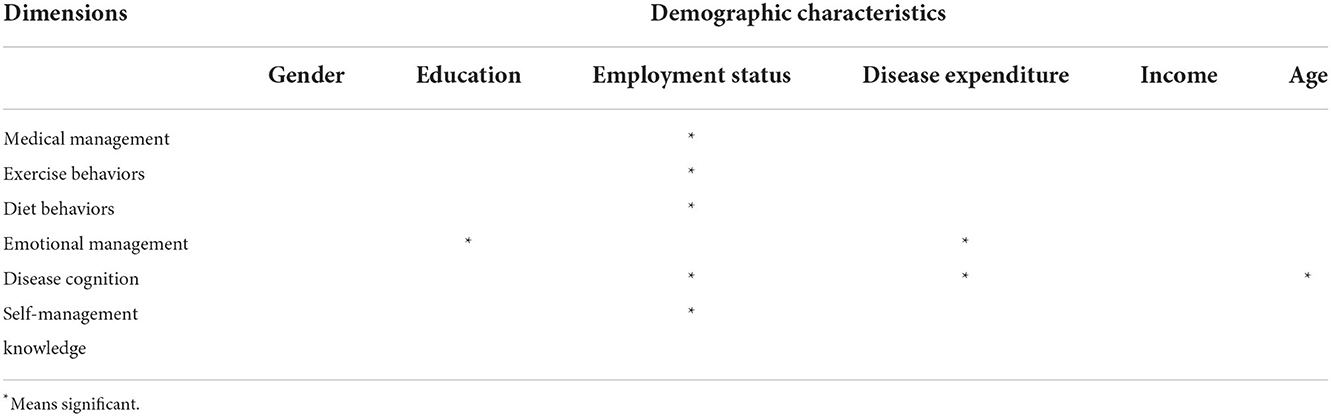
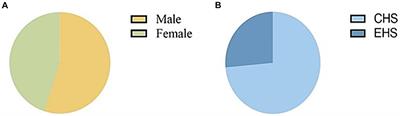
Results DemographicThe demographic information characteristics of the sample patients are shown in Table 2. The F test for six behavior dimensions on six characteristics can be seen in the Appendix on gender, education level, employment status, disease expenditure, household income, and age. The whole F test results show in Table 3 between demographic and behavior.
Table 2. Demographic information of CKD patients (n = 131).
Table 3. All F-test results.
According to Table 3 and the Appendix Tables, from the demographic insight, gender and income are not statistically significant for self-management, while educational background, employment status, disease expenditure, and age have significant differences, though the impact is uneven. Employment status substantially affects the five dimensions other than emotional management, and the patient's educational background and disease expenditure impact emotional management. The higher the education level and the less disease expenditure, the better the emotional management of patients. In the dimension of disease cognition, the patient's age, employment status, and disease expenditure are impact factors. Further analysis found that the poorer the patient's employment, the younger the patient, and the less the disease expenditure, the lower the patient's cognition of the disease. On the contrary, unemployed patients, middle education and middle age, have a high score in self-management, which is similar to Audulv's study (24).
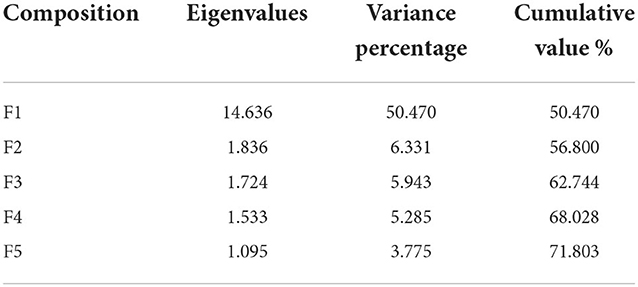
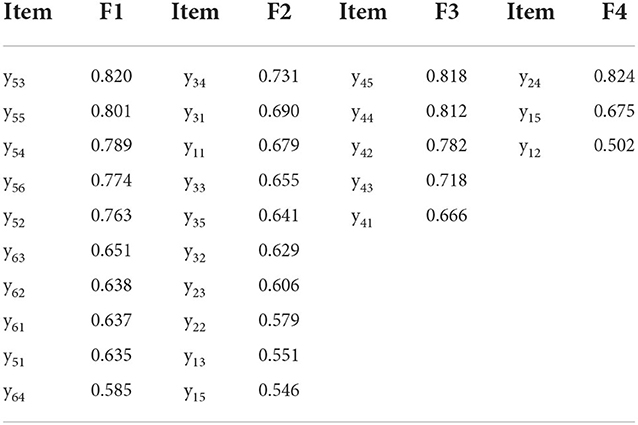
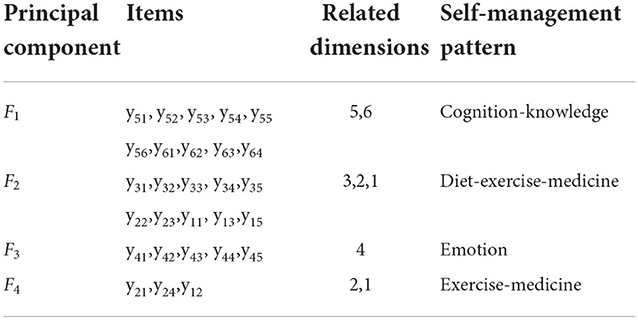
Principal componentWith principal component analysis of 29 items, five principal item components with eigenvalues >1 were obtained, which can explain 71.803% of the original information cumulatively (see Table 4). The explanation level of the fifth principal component is 3.775%, which is < 5%. The first four principal components are finally extracted, and the interpretation degree is 68%. The explanatory variables (items) are sorted according to the descending order of the factor load of 4 principal components in Table 5. According to the 4 principal components, the corresponding self-management pattern can be summarized. See Table 6 for principal components, explanatory variables, and patterns.
Table 4. Initial eigenvalues and variance.
Table 5. Principal component and factor (item) load matrix.
Table 6. Principal components, items, and patterns.
According to the eigenvalues of the 4 principal components in Table 6, F1 is the highest one which means disease Cognition-Knowledge pattern dominates. The component loads show that F2 has a strong positive correlation with ten items in the dimensions of diet, exercise, and medicine management. The eigenvalues of F2,F3 and F4 decrease in order; that is, among the self-management patterns of CKD patients, the preference for the Diet-Exercise-Medicine pattern, Emotion pattern, and Exercise-Medicine pattern decreases in order.
In the self-management pattern, exercise and medicine appeared two times among the four patterns, so it is the primary behavior that leads patients to self-management. Diet behaviors, emotional management, disease cognition, and self-management knowledge only appeared once in each self-management pattern.
According to the principal component analysis results, there is a progressive relationship among the four self-management patterns. Firstly, to improve patients' self-management behavior, patients' cognition of the disease and related knowledge of self-management should be strengthened so that patients understand the disease's causes and can better cooperate with the doctor's advice. After certain basic cognition, patients should be further told to control their diets, exercise appropriately, and cooperate with medication according to the doctor's requirements, namely the Diet-Exercise-Medicine pattern. Good emotions have a positive impact on patients' conditions. It is also vital for patients to manage their emotions well under the condition of ensuring good diet habits. Finally, the importance of exercise and medication management is emphasized again in the Exercise-Medicine pattern, indicating that these two aspects are challenging for patients to form habits, which need to be reminded again and paid more attention to it.
DiscussionAccording to social cognitive theory (25), a patient's self-management behavior, individual factors, and environmental factors interact. Based on these interaction results, the study puts forward the following suggestions for China outpatients with CKD to improve and support the patient's self-management ability.
For patients, the self-management ability of employed patients in the five dimensions is significantly lower than that of unemployed patients. So, employed patients need to strengthen their awareness and ability in self-management behaviors. Patients should increase interactive communication with medical professional institutions and follow expert opinions. They should maintain a certain exercise frequency and diet habits (24). Exercise intervention is also an effective way to improve CKD patients' self-management ability (26). At last, CKD patients should attach importance to multi-dimensional self-management of disease balance and actively accept systematic self-management services in personality.
For health care providers, medical service providers are an important subject for patients to receive self-management support in the chronic disease care model (CCM) (27), such as hospitals and public health communities (28). This article recommends that medical service providers provide customized intervention programs for patient groups based on chronic kidney disease. Medical service providers should identify patients' demographic characteristics, diagnose patients' self-management patterns, capture and improve the weaknesses of self-management capabilities and implement precise self-management interventions using information technology (29) from social insight (30). For example, for middle-aged and elderly, high-employment, high-education, and medium-expenditure patients with weaker diet behaviors capabilities, hospitals can popularize healthy diet knowledge courses and customize meal lists with the Internet and smart wearable devices to improve patients' cognition and knowledge behavior.
In the social environment, the public generally lacks emotional management (31). Some patients with CKD pay attention to emotional management only in this study. Compared with simply taking medication as prescribed by a doctor, it is more difficult for patients to change their lifestyles, which are hindered by chronic pain and fatigue, interrupted habits, and lack of family support (24). So support from the environmental aspects is added, such as online devices in the patient's home (32).
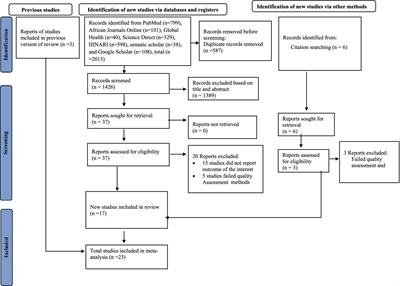
ConclusionsTo conclude, based on the inductive assumption that patient's self-management need supports from stakeholders, this study investigated and analyzed the cross-sectional data of 131 patients with CKD self-management scale, used the F-test to find some demographic characteristics of behavior, and the principal component method to identify the self-management pattern of chronic disease patients among outpatients. The analysis results show that patient with different demographic characteristics has formed four patterns, such as diet behaviors, emotional management, disease cognition, and self-management knowledge to manage their disease. Our study's results help to clarify the self-management behavior patterns and characteristics of different chronic patients, especially for employees, providing a basis for improving the self-management behavior of patients with CKD from three sectors: patients, providers, and society. However, this study only investigated the outpatients of the Nephrology Department and was limited by the scope and number of samples; the results still need more sample tests. This study also has other limitations, such as the lack of detailed patient clustering analysis and more explanations of why the employment status is the most significant, which will be further discussed in subsequent studies.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementThis study was reviewed and approved by the Ethics Review Committees of West China Hospital (2020-740). All participants provided informed consent before participation in the study.
Author contributionsXH supervised, reviewed, and edited. YW conceptualized and wrote the first draft. CF, LL, and UK participated in proofreading, reviewing, and editing. FR did formal analysis and editing. XZ reviewed and edited. All authors read and approved the final manuscript.
FundingThis work was funded by West China Nursing Discipline Development Special Fund Project, Sichuan University (Grant No. HXHL19013) and Natural Science Foundation for the Youth Fund Project of Sichuan University (Grant No. 71904138).
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.973488/full#supplementary-material
References1. Jeddi FR, Nabovati E, Amirazodi S. Features and effects of information technology-based interventions to improve self-management in chronic kidney disease patients: a systematic review of the literature. J Med Syst. (2017) 41:1–13. doi: 10.1007/s10916-017-0820-6
PubMed Abstract | CrossRef Full Text | Google Scholar
2. Shen H, van der Kleij R, van der Boog PJ, Song X, Wang W, Zhang T, et al. Development and evaluation of an eHealth self-management intervention for patients with chronic kidney disease in China: protocol for a mixed-method hybrid type 2 trial. BMC Nephrol. (2020) 21:1–16. doi: 10.1186/s12882-020-02160-6
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Havas K, Douglas C, Bonner A. Person-centred care in chronic kidney disease: a cross-sectional study of patients' desires for self-management support. BMC Nephrol. (2017) 18:1–9. doi: 10.1186/s12882-016-0416-2
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Aria R, Archer N. An online mobile/desktop application for supporting sustainable chronic disease self-management and lifestyle change. Health Informatics J. (2020) 26:2860–76. doi: 10.1177/1460458220944334
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Lawn S, Battersby MW, Pols RG, Lawrence J, Parry T, Urukalo M. The mental health expert patient: findings from a pilot study of a generic chronic condition self-management programme for people with mental illness. Int J Soc Psychiatry. (2007) 53:63–74. doi: 10.1177/0020764007075010
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Rogers A, Kennedy A, Bower P, Gardner C, Gately C, Lee V, et al. The United Kingdom Expert Patients Programme: results and implications from a national evaluation. Med J Aust. (2008) 189:S21–4. doi: 10.5694/j.1326-5377.2008.tb02205.x
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Stellefson M, Dipnarine K, Stopka C. Peer reviewed: the chronic care model and diabetes management in US primary care settings: a systematic review. Prev Chronic Dis. (2013). 10:E26. doi: 10.5888/pcd10.120180
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Booker S, Herr K, Tripp-Reimer T. Patterns and perceptions of self-management for osteoarthritis pain in African American older adults. Pain Med. (2019) 20:1489–99. doi: 10.1093/pm/pny260
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Adibelli D, Özkan I. Self-management of chronic disease in individuals with psychotic disorder: a qualitative study. Perspect Psychiatr Care. (2021) 57:702–8. doi: 10.1111/ppc.12598
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Araújo-Soares V, Hankonen N, Presseau J, Rodrigues A, Sniehotta FF. Developing behavior change interventions for self-management in chronic illness: an integrative overview. Eur Psychol. (2019) 24:7. doi: 10.1027/1016-9040/a000330
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Shneerson C, Taskila T, Holder R, Greenfield S, Tolosa I, Damery S, et al. Patterns of self-management practices undertaken by cancer survivors: variations in demographic factors. Eur J Cancer Care (Engl). (2015) 24:683–94. doi: 10.1111/ecc.12252
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Chuang LM, Wu SV, Lee MC, Lin LJ, Liang SY, Lai PC, et al. The effects of knowledge and self-management of patients with early-stage chronic kidney disease: Self-efficacy is a mediator. Jpn J Nurs Sci. (2020) 2022:18. doi: 10.1111/jjns.12388
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Meng HL, Ma LL, Zhang Y, Sun L. Status quo and influencing factors of self-management behavior of patients with early chronic kidney diease. Chin Nurs Res. (2016) 30:3699–701. doi: 10.3969/j.issn.1009-6493.2016.29.038
CrossRef Full Text | Google Scholar
16. Wu SV, Wang TJ, Liang SY, Lin LJ, Lu YY, Lee MC. Differences in self-care knowledge, self-efficacy, psychological distress and self-management between patients with early-and end-stage chronic kidney disease. J Clin Nurs. (2021) 31:2287–95. doi: 10.1111/jocn.16046
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Gao T, Zhang X, Gurd B, Liu Z. From self-management to a systemized process: the implementation of lean management in a Chinese hospital's pharmacy intravenous admixture services center. Leadersh Health Serv (Bradf Engl). (2020) 33:325–37. doi: 10.1108/LHS-12-2019-0085
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Paolanti M, Frontoni E. Multidisciplinary pattern recognition applications: a review. Comput Sci Rev. (2020) 37:100276. doi: 10.1016/j.cosrev.2020.100276
CrossRef Full Text | Google Scholar
19. Bhamare D, Suryawanshi P. Review on reliable pattern recognition with machine learning techniques. Fuzzy Inf Eng. (2018) 10:362–77. doi: 10.1080/16168658.2019.1611030
CrossRef Full Text | Google Scholar
20. Parajuli N, Sreenivasan N, Bifulco P, Cesarelli M, Savino S, Niola V, et al. Real-time EMG based pattern recognition control for hand prostheses: a review on existing methods, challenges and future implementation. Sensors (Basel). (2019) 19:4596. doi: 10.3390/s19204596
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Audulv, Å. The over time development of chronic illness self-management patterns: a longitudinal qualitative study. BMC Public Health. (2013) 13:1–15. doi: 10.1186/1471-2458-13-452
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Bailey WC, Kohler CL, Richards JM Jr, Windsor RA, Brooks CM, Gerald LB, et al. Asthma self-management: do patient education programs always have an impact? Arch Intern Med. (1999) 159:2422–8. doi: 10.1001/archinte.159.20.2422
PubMed Abstract | CrossRef Full Text | Google Scholar
26. Schmidt-Busby J, Wiles J, Exeter D, Kenealy T. Understanding ‘context'in the self-management of type 2 diabetes with comorbidities: A systematic review and realist evaluation. Diabetes Res Clin Pract. (2018) 142:321–34. doi: 10.1016/j.diabres.2018.06.003
PubMed Abstract | CrossRef Full Text | Google Scholar
27. Gammon D, Berntsen GK, Koricho AT, Sygna K, Ruland C. The chronic care model and technological research and innovation: a scoping review at the crossroads. J Med Internet Res. (2015) 17:e3547. doi: 10.2196/jmir.3547
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Washington T, Zimmerman S, Browne T. Browne, Factors associated with chronic kidney disease self-management. Soc Work Public Health. (2016) 31:58–69. doi: 10.1080/19371918.2015.1087908
PubMed Abstract | CrossRef Full Text | Google Scholar
29. Still CH, Jones LM, Moss KO, Variath M, Wright KD. African American older adults' perceived use of technology for hypertension self-management. Res Gerontol Nurs. (2018) 11:249–56. doi: 10.3928/19404921-20180809-02
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Liu Q, Jin Y, Wang Y, Feng J, Qiao X, Ji L, et al., Association between self-efficacy and self-management behaviours among individuals at high risk for stroke: Social support acting as a mediator. J Clin Nurs. (2022) 1–12. doi: 10.1111/jocn.16191
PubMed Abstract | CrossRef Full Text | Google Scholar
31. Donald M, Kahlon BK, Beanlands H, Straus S, Ronksley P, Herrington G, et al. Self-management interventions for adults with chronic kidney disease: a scoping review. BMJ Open. (2018) 8:e019814. doi: 10.1136/bmjopen-2017-019814
PubMed Abstract | CrossRef Full Text | Google Scholar
32. Zimbudzi E, Lo C, Misso ML, Ranasinha S, Kerr PG, Teede HJ, Zoungas S. (2018). Effectiveness of self-management support interventions for people with comorbid diabetes and chronic kidney disease: a systematic review and meta-analysis. Syst Rev. 7:84. doi: 10.1186/s13643-018-0748-z
留言 (0)