
記住我




This prospective non-randomized cohort study was conducted at the 1st Hospital of Lanzhou University, Department of Oral and Maxillofacial Surgery, from September 2017 to February 2020. Twenty-nine consecutive patients who underwent ORIF (RMA or SMA) for the unilateral subcondylar fracture were included. All patients were evaluated presurgical with clinical examination and Panoramic/CT-scan. An informed consent form, including explanation about the two approaches, was obtained from patients. The cohorts were informed of the right to refuse to participate in the study or to withdraw consent to participate at any time without reprisal.
This study followed the Declaration of Helsinki on medical protocol and ethics and the regional Ethical Review Board of Stomatology College, Lanzhou University approved the study. The postoperative 3-D CBCTs were used for radiological evaluation. The clinical assessment was conducted by malocclusion, mouth opening limitation, and postoperative pain.
Comparing between retromandibular and submandibular approaches was implemented. Also, the fracture side and non-fracture side were analyzed.
The patients included in this study were suffering from simple unliteral subcondylar fracture, with 5° to 40° deviation between the subcondylar and the ascending ramus, more than 2 mm shortage of ramus, older than 18 years old, and limitation of mouth opening. Patients with any history of TMD, less than 18 years old, bilateral subcondylar fracture, condylar head fracture, insufficient dentition, treated with closed treatment or endoscopic and patients with comminuted fractures were excluded from this study. Demographic data is included in Table 1.
The Comprehensive AOCMF Classification System by Neff, A., et al., 2014 was used in this study [13].
Clinical assessmentHelkimo index scoring system was implemented in the current study to evaluate TMJ function. Helkimo Ai has utilized the TMJ dysfunction subjectively. On the other hand, Di represented the objective assessment of the impaired TMJ function. Both subjective and objective symptoms were evaluated by the limitation of mouth opening, TMJ function impairment, pain in the muscle, and TMJ. The patient was classified as Ai0 (asymptomatic), AII (Mild symptoms), AiIII (severe symptoms). The score for the Di is shown in Table 2.
Patients were followed for six months (at least). Pain in the temporomandibular joint (TMJ) region, facial nerve weakness, occlusion disturbances, and interincisal mouth opening were assessed.
Surgical operationAll the Open Reduction and Internal Fixation was performed by one surgeon in consecutive pattern. Patients underwent ORIF under general anesthesia. The RMA and SMA procedures are outlined below:
In the RMA group, it was similar to what Ellis and Dean described. Shortly, gentian violet was used to mark the subcutaneous skin incision (3–4 cm) below the ear pinna and 1 cm behind the angle of the mandible. Dissection was made until the subplatysmal layer. Once the parotid gland fascia was identified, the blind dissection was carried out parallel with facial nerve direction; once facial nerves were encountered, they were first carefully dissected and retracted to decrease the tension. The periosteum was incised at the posterior border of the mandibular. After the subperiosteal dissection of the ramus and subcondylar region, the reduction and fixation of the fracture fragments were obtained. For providing enough working space on the fracture line, the manual downward pressure was applied. Two suitable 2.0 mm miniplates were used to fix the fracture sides, and then copious irrigation was applied. Sufficient care was paid to the parotid gland and masseteric capsules to complete closure by a resorbable suture, whereas the non-resorbable suture was used for skin closure.
In the SMA group, gentian violet was used to mark the 2–3 cm line below the mandible border. The incision was made and once the exposure was not enough the incision was extended in either direction. Dissection was performed to the platysma muscle, and a blunt scissor was used to bisect the muscle. The cervical fascia was then cut with the care of not causing facial nerve damage. The masseteric sling then incised above the lower border of the mandible, and subperiosteal dissection was achieved until the exposure of the subcondylar area and the reduction and fixation was made. The drilled hole at the angle of the mandible was used to fix the wire used for the reduction.
Radiological assessmentTen days after the operation, a Cone-beam computer tomography was applied to assess the reduction process. All CBCTs were collected spontaneously with patients record. CBCTs were taken in standardized protocol to have the same area of interest without a high discrepancy between patients. CBCTs were collected on DICOM form, and the exposure parameter was set at 20.27 Mas, 120KVP, and 14.9 s. The voxel of the image was also set at 0.4 mm. Three-dimensional analysis was carried out for both groups; RMA and SMA groups. The joint space volume was measured by the equation of sigma V \(\cong _A\left(_\right)\Delta \chi\). The whole joint space was sectioned; each section had a width of 1 mm. Tuberculo-metal line (TML), a line from Anterior Tubercle (AT) to Inferior Auditory Meatus (IM) points, was used as the.
inferior border to joint volume. The coordinate system with skeletal midline points was used previously ElBeialy et al., 2011 [14]. Each point was digitized and adjusted by a three-slice locator (Fig. 1).
Fig. 1
Slice locator position in different planes
Nasion point was considered the reference point. It was determined on three planes; axial (Y), coronal(X), and sagittal(Z), which were used to build the 3D mold. The three-dimensional equation was used to measure the planes d = \(\sqrt__)}^+(_-_^+(_-_^}\). The Skeletal landmarks, 3-D lines, planes, and measurements for condylar position and angulation are listed in Tables 3 and 4, Figs. 2, 3, 4 and 5 respectively.
Fig. 2
Condylar position and inclination to the midsagittal plane in RMA group. CDMP; condylar medial point, CDLP; condylar lateral point, CDAPi (MSP); condylar anteroposterior inclination to the midsagittal plane, CDML position; condylar mediolateral position
Fig. 3
Condylar position and inclination to the vertical plane in RMA group. CDPP; condylar posterior point, CDAP; condylar anterior point, CDVi(VP); condylar vertical inclination to Vertical plane, CDAP position; condylar anterior posterior position
Fig. 4
Condylar position and inclination to the horizontal plane in SMA group CDLP; condylar lateral point. CDLP; condylar lateral point, CDMP; condylar medial point, CDSP; condylar superior position, HP; horizontal plane, CDV position; condylar vertical position, CDMLi (HP); condylar mediolateral inclination to horizontal plane
Fig. 5
Joint spaces PJS; posterior joint space, SJS; superior joint space, AJS; anterior joint space, MJS; medial joint space, AT; anterior tubercle, IM; auditory meatus, ML line; tuberculo-meatus line
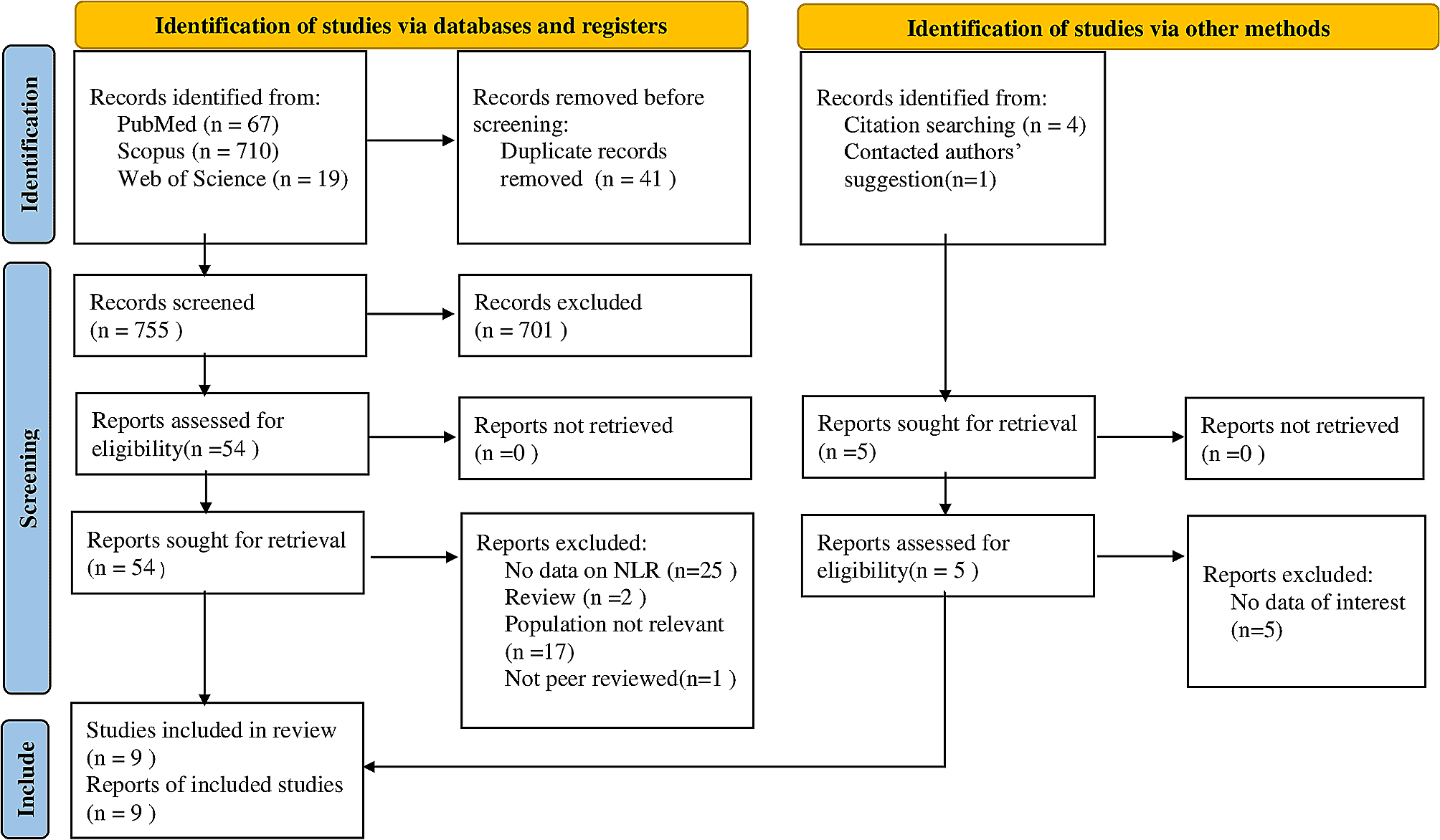
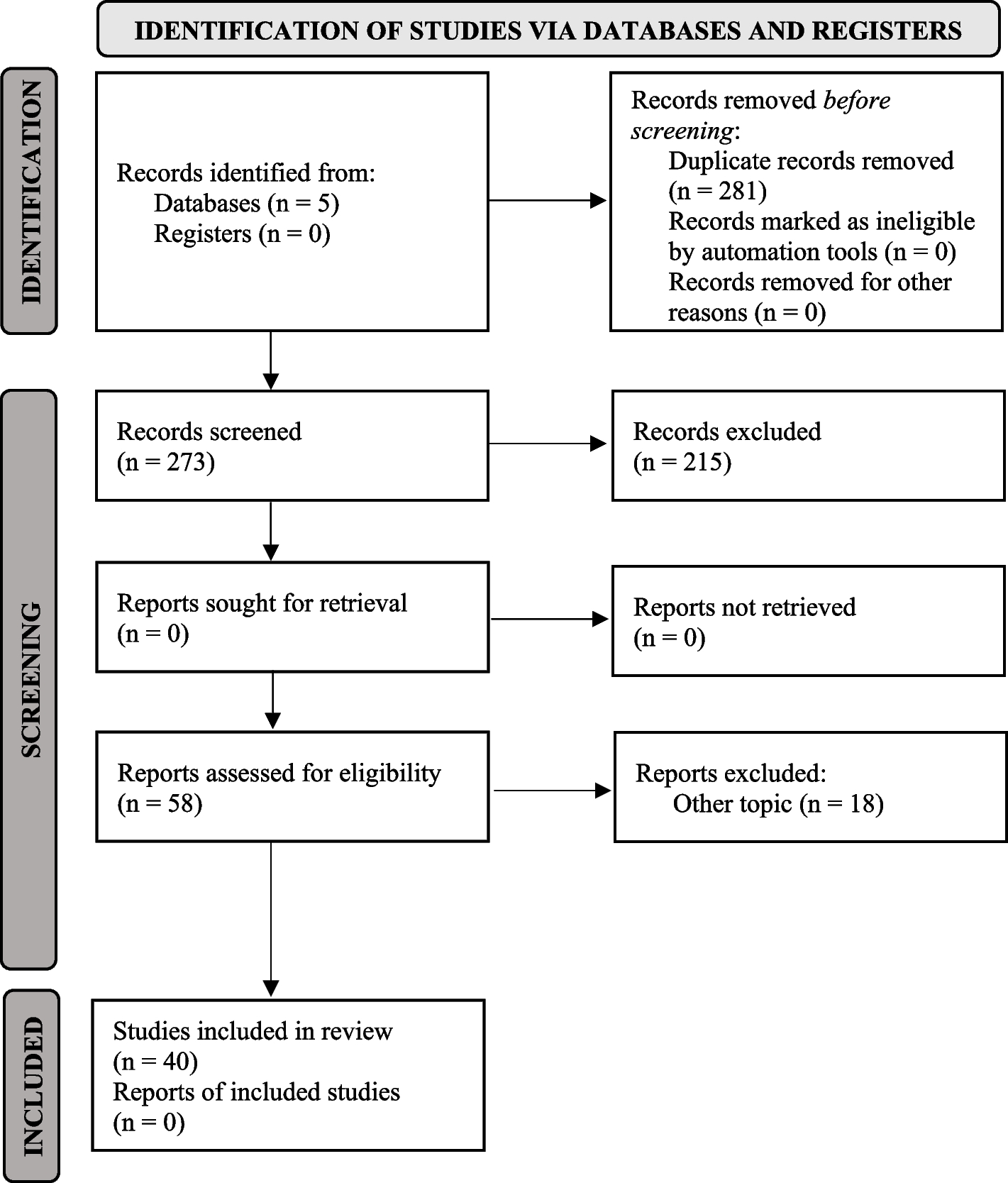
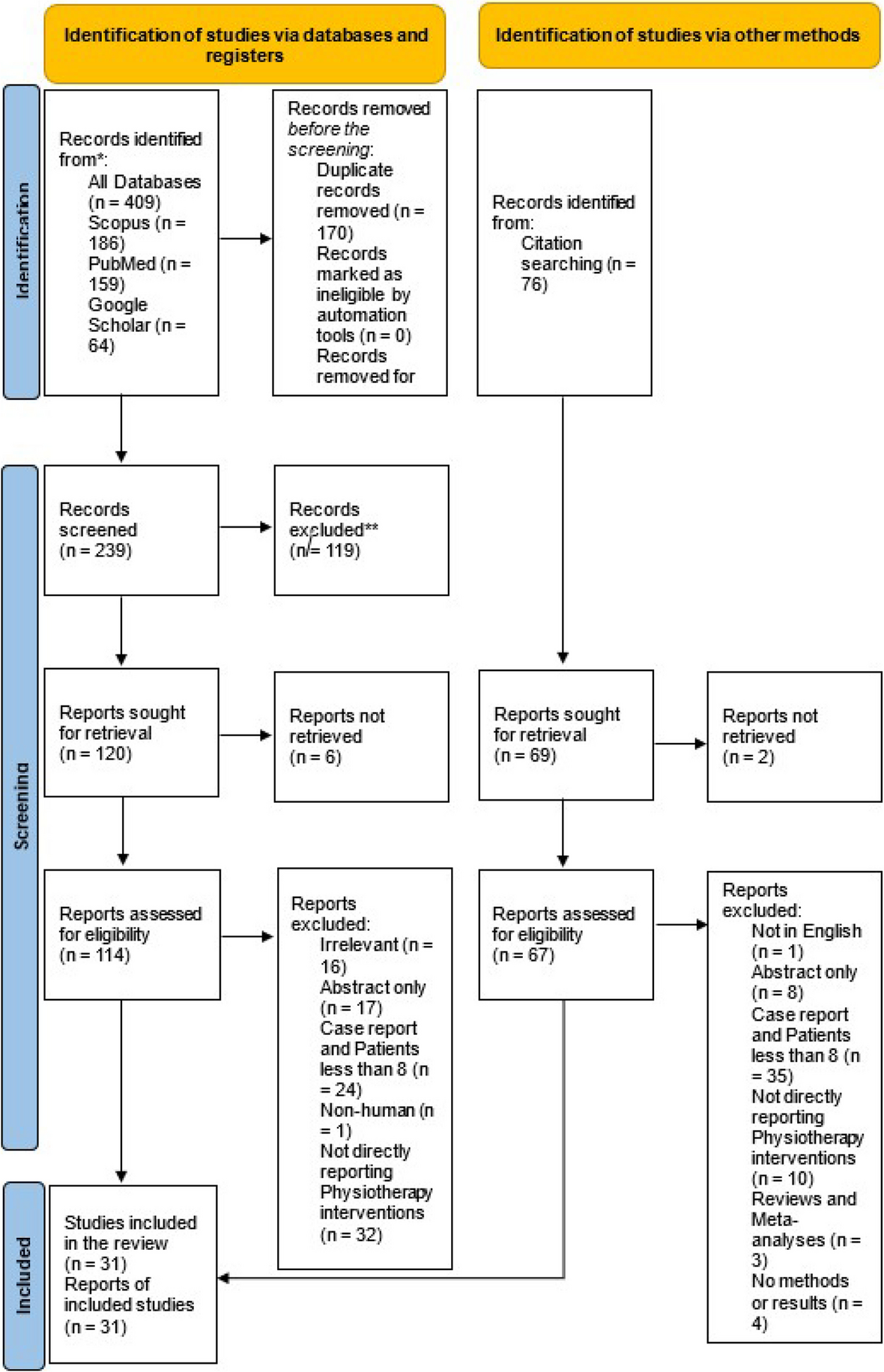
National Institutes of Health Database (PubMed) was conducted for the literature review.
Statistical analysisDescriptive information was reported as mean and standard deviation. The difference in mean between the two groups was assisted by the independent t-test. Pearson’s correlation analyzed the correlation between the joint space, and condylar position and angulation. Also, the relation between the clinical finding and the fracture side measurement was tested. The interclass correlation was utilized to check the agreement between two independent observers. The P-value was set at 0.05 or less to indicate the statistical significance. All analysis was performed by the IBM SPSS Statistics version 26 (IBM Corp., Armonk, NY, USA).
留言 (0)