HTN-C is a relatively rare event and is associated with end-organ damage. One study has reported that 18.9% of children with HTN-C were caused by RAS [12]. The incidence of RVH in both adults and pediatrics is about 5%-10% [8, 13]. The difference between RVH and other causes of hypertension is that RVH can be cured by medication, intravascular intervention or surgery. In this study, we evaluated the clinical manifestations, diagnosis, treatment, and therapy results of 54 patients with heterogeneous renal artery disease leading to pediatric RVH, and represents one of the largest series of pediatric RAS studies to date, besides studies from Lobeck et al. [14], Agrawal et al. [15] and Wu et al. [16].
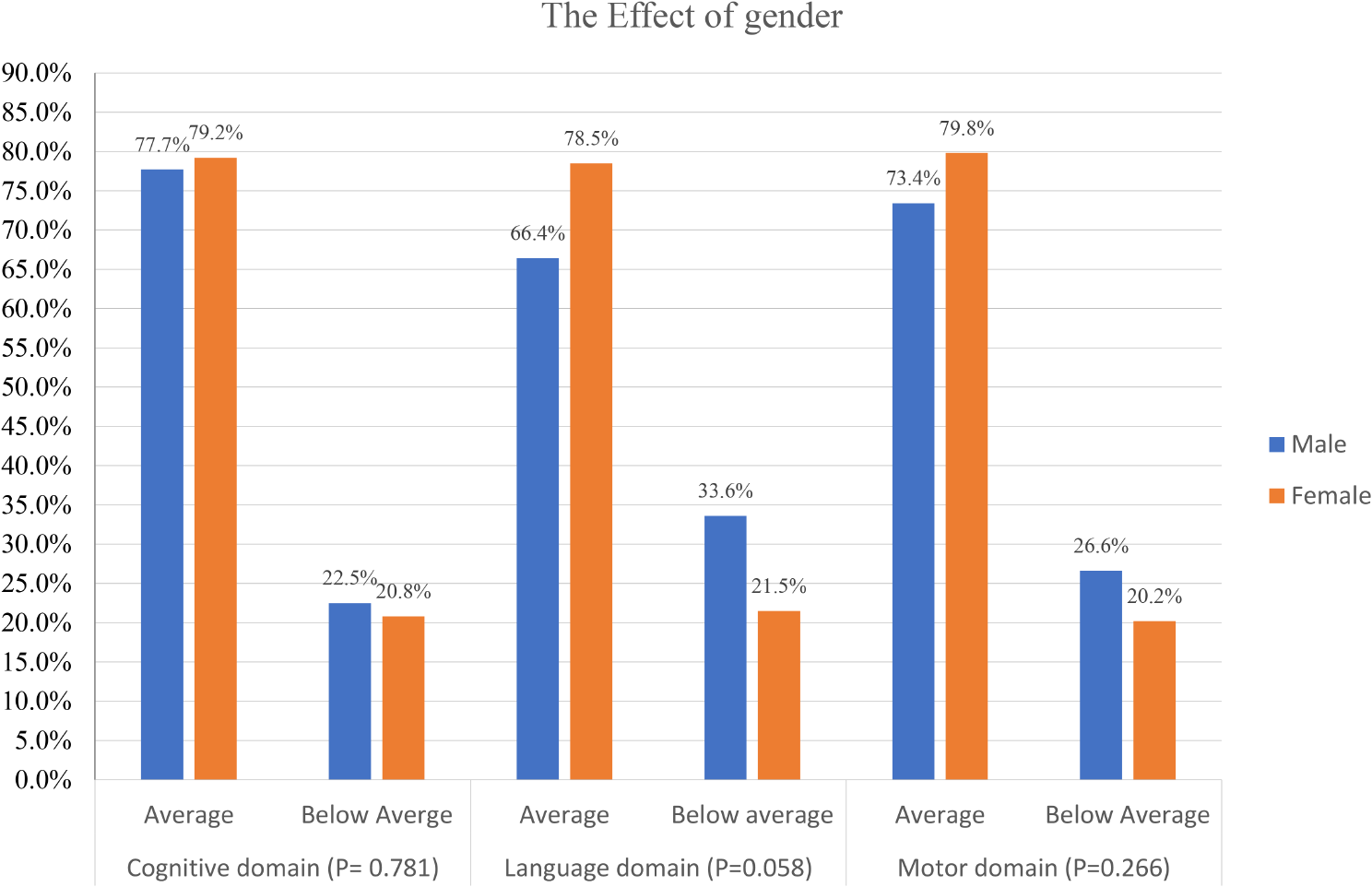
This study found that the detection rate of RVH in children was 5.5%, accounting for 6.8% (54/792) of 792 children with secondary hypertension. 83.3% of the RVH patients were male children over 6 years old. The ratio of male to female was about 3:1, which is consistent with a previous study[8]. We observed that the detection rate of HTN-C in children with RVH was as high as 94.4%, of whom 64.7% (33/51) were hypertensive emergencies. Lee et al. [5] reported RVH as the main cause of HTN-C, indicating that despite the incidence of renovascular hypertension may not be high, however, its clinical manifestations could be life-threatening if not diagnosed and treated on time. For children with hypertension, proper awareness and guidance should be provided to the caretaker regarding the first manifestation of HTN-C and male children for a timely diagnosis of RVH.
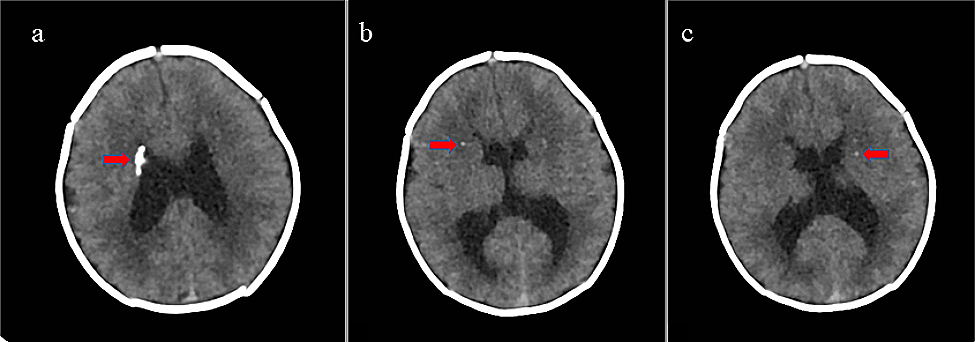
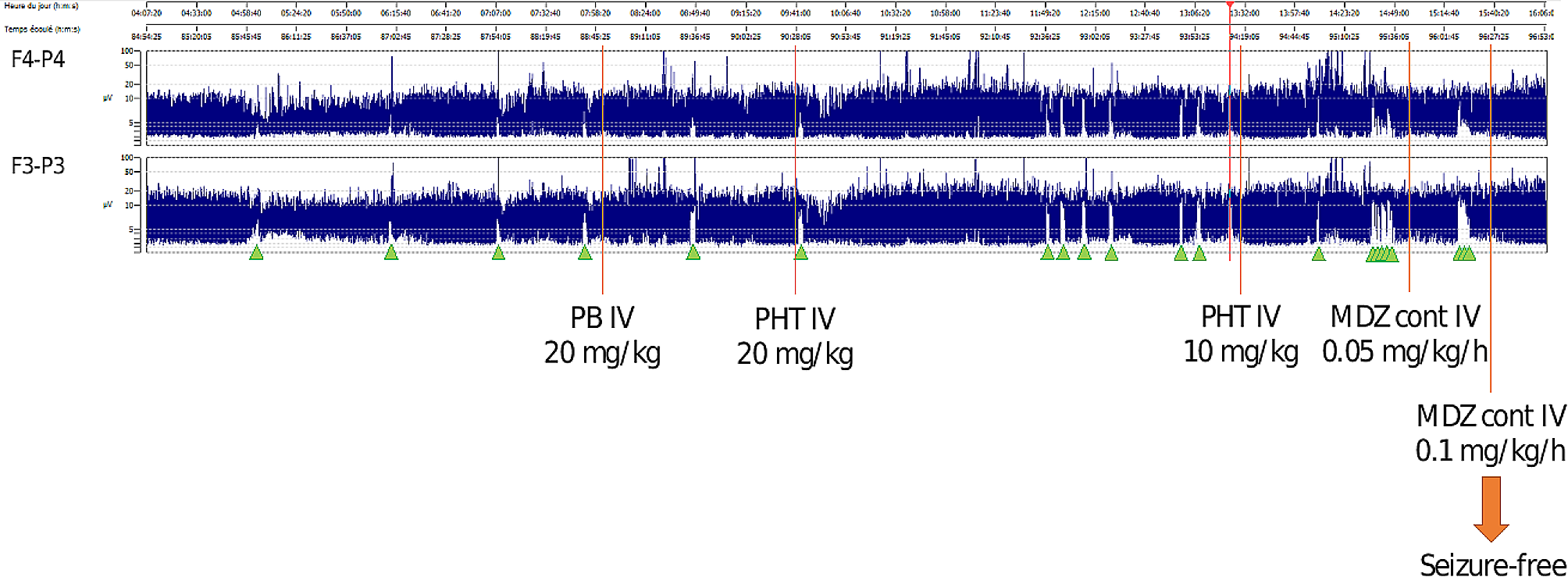
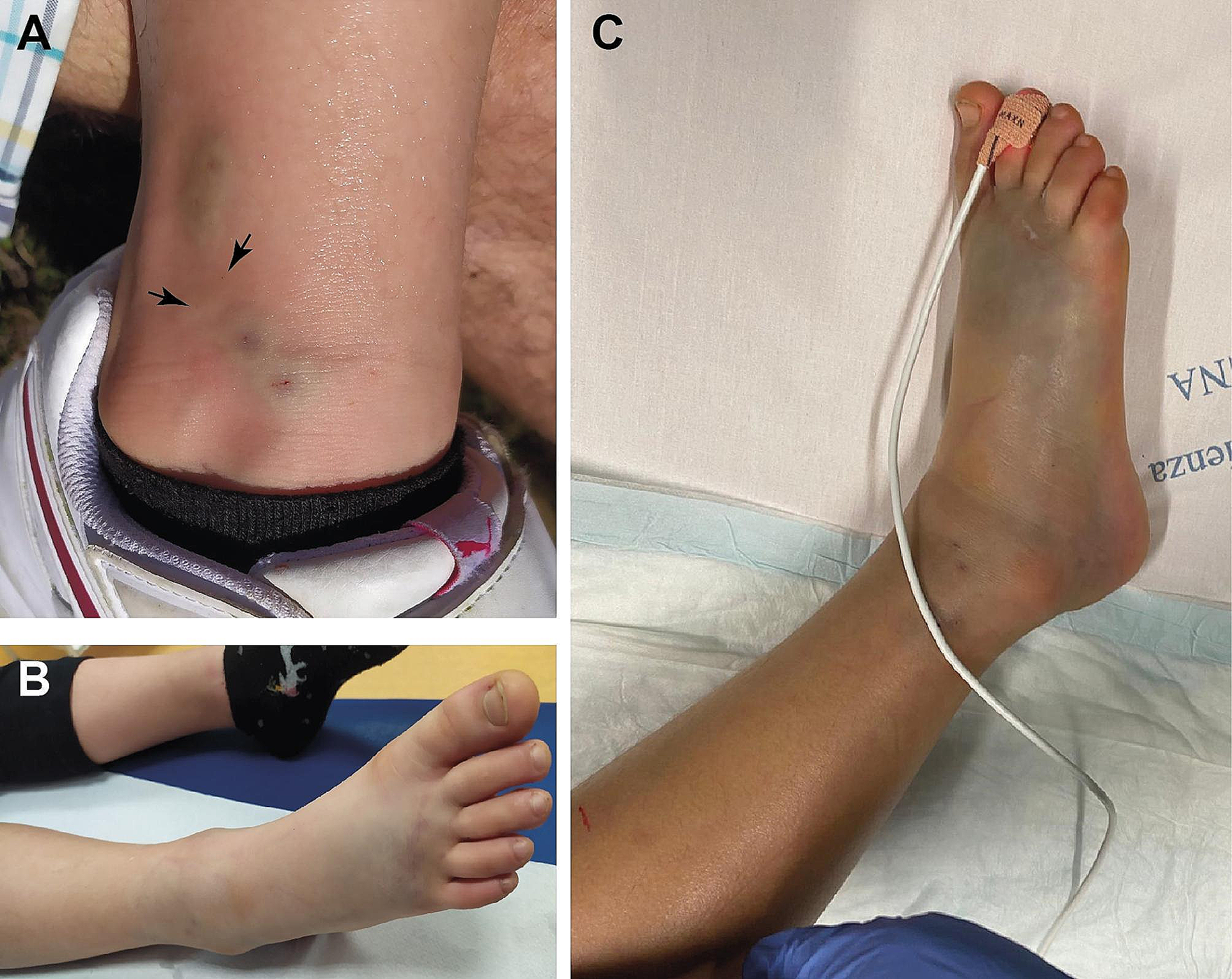
The clinical manifestations of RVH in children may vary greatly. They may be asymptomatic, or may have obvious headaches, dizziness, and even severe neurological symptoms such as convulsions and hemiplegia. Similar to the results reported by Lobeck et al.[14], the vast majority of children with RVH in this study had HTN-C at the time of treatment, and the main symptoms were hypertensive emergencies. We also found that most of the children in the HTN-U group were asymptomatic. Therefore, we suggest that it is necessary to monitor the blood pressure of children during routine physical examinations to screen for hypertension. The first symptoms of the HTN-E group were headache and blurred vision as the main neurological symptoms, which is consistent with a previous report [14]. Moreover, the HTN-E group had higher SBP and DBP than the HTN-U group, and the SBP was higher and more obvious than the HTN-U group. The difference between HTN-E and HTN-U groups was statistically significant, which is consistent with the results of a study by the Institute of Clinical Medicine in Taiwan [16]. Therefore, for severe hypertension with neurological symptoms, it is necessary to provide timely blood pressure control, especially for elevated SBP, and actively screen for RVH to avoid progression to hypertensive emergency.
Our study found that 77.8% (21/27) of children with RVH had retinopathy, 40.0% had hypertensive encephalopathy and 71.4% had left ventricular hypertrophy, which was consistent with the results reported by Tullus et al. [8]. These were higher than the detection rates of retinopathy [17], hypertensive encephalopathy [16], and left ventricular hypertrophy reported in previous literatures and could be related to ethnic differences and the high salt diet habits of Chinese children [5, 18]. Further, because most of the children with RVH in this study were asymptomatic and were found to have high blood pressure during outpatient clinics or physical examinations (or even reached sub-emergency hypertension), lack of awareness among their parents could have contributed to delayed treatments, for several months or even more than a year, before a formal diagnosis and treatment of hypertension. Some patients after having obvious headaches and other neurological symptoms were not properly treated, leading to the majority of children with RVH in this study who were in the HTN-C group, and target organ damage being more common in them. Therefore, children with RVH should be routinely evaluated for target organ damage.
RAS is mostly caused by conditions such as FMD, Takayasu’s arteritis, neurofibromatosis as well as some unexplained factors that lead to RAS. Tullus et al. [8] reported that there could be variable etiologies of RVH in children, and could also be associated with regional differences. FMD is the most common cause of RVH in children in North America and Europe, with an incidence rate of 35%-76% [14, 19, 20]. However, Takayasu's arteritis is the main cause of RVH in children in Asia and South Africa [8]. McCulloch et al. [21] reported that 89% of children with RVH were mainly caused by TA. Studies on children with RVH in China and Turkey reported that the incidence of Takayasu's arteritis was 60%-72% [22, 23]. In this current study, we found that 59.3% (32/54) of children with RVH were of unknown etiology. Among the identified causes, Takayasu’s arteritis was the main cause, accounting for 50%, followed by congenital renal dysplasia (27.3%) then FMD (13.6%), and was different from the incidence of the etiology reported in a previous study[8]; and could indeed be related to the unknown etiology and regional differences of most patients in this study.
The arterial lesions of RVH can be different. About half of patients with RVH have bilateral renal artery involvement, with or without intrarenal and (or) extrarenal vascular disease [8]. In this study, the incidence of bilateral RAS was 22.2%, which was similar to the incidence of 24%-28% reported in other literatures [14, 24]. It was also observed in our study that 14.8% (8/54) of children with RVH had extracranial and intracranial cerebrovascular diseases, and most of the RAS was mainly proximal stenosis.
RVH is considered to be the prototype of renin-dependent hypertension. Therefore, the measurement of basal and stimulating plasma renin activity (PRA) in peripheral and renal venous blood is widely used for diagnosis. However, the findings from a study [25] showed that the release of renin on the stenotic side of RAS required 10% to 20% of the aortic-renal pressure gradient. When the pressure gradient reached 50%, the renal vein blood renin release of the stenotic side was the largest. This study found that not all children had elevated blood renin levels, which was inconsistent with the severity of renal artery stenosis. Unilateral RAS was the main cause of RVH and it was mostly related to peripheral venous blood sampling to detect renin levels. This indicates that low levels of peripheral blood or renal venous blood renin levels could not rule out RVH. Hypokalemia and increased plasma renin and angiotensin levels are considered to be clues to the diagnosis of RVH [8]. In this study, 13 children with RVH had hypokalemia, and most of them were accompanied by high renin levels. This further confirmed that the diagnosis of renovascular hypertension should be carefully assessed, when hypertension is complicated with hypokalemia. Therefore, our study findings may provide clues to improve the diagnosis and treatment of pediatric RVH.
Limitations
The main limitation of this study is its retrospective single-institution design, which involved only hospitalized patients, spanned on about three decades and included different practice models, possibly leading to some extent of selection biases. Further, as this was a retrospective study, laboratory results were incomplete in some cases, and none of the cases could be suggested to undergo genetic testing, leading to a possible failure to diagnose NF1 and Williams' diseases. Also, some cases could not be included due to limited availability of early part of their electronic records for patient retrieval and assessments using diagnostic codes.





留言 (0)