
記住我





The main finding of this study is that trochlear coronal alignment of arthritic knees and that of current TKR implants differ significantly (Table 2). According to the analysis, only 58.55% of knees in the sample would fall in a matched PTA-NTA range if all the studied models were available for implantation, using the mechanical alignment technique (Fig. 4). With a non-mechanical technique, the PTA-NTA would further change; typically, positioning the femoral component in valgus will orientate the prosthetic trochlea in varus (and vice versa), increasing the NTA–PTA discrepancy (as 60.6% of knees have a valgus NTA). It is noteworthy that two-thirds of all primary knee prostheses implanted in Australia in 2014–2021 have been included in this analysis [1], which emphasizes the potential significance of this mismatch in the clinical scenario.
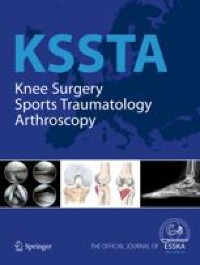
Fig. 4
Distribution of native trochlear angles (NTA) in the study cohort. Green bars represent varus alignment, while blue bars correspond to valgus alignment. Shaded area reflects the prosthetic trochlear angle (PTA) range
Dejour et al. conducted a morphologic analysis of trochlear design in 14 TKR models available in 2014, with similar results. All trochleae were valgus-oriented (mostly in the 5°–8° range) except for one, which was neutral [5]. Therefore, at least in regards to trochlear coronal orientation, there has been little evolution during the last decade. The trochlear design of current TKR models is based on the assumption that most native knees present a valgus trochlea [2]; this concurs with the present results showing a mean PTA of 6.18° of valgus. However, the analysis also suggests that NTA range is more varus (or less valgus) than it has been generally considered [10].
There are a handful of previous reports rejecting valgus alignment as the natural conformation of the femoral trochlea. Ekhoff et al. and Koh et al. described a neutral orientation of the femoral trochlea, with means of 0.4° ± 5° and − 0.1° ± 9°, respectively [8] [16]. The cadaveric study by Barik et al. revealed an average varus orientation (1.8° ± 2.1°) of the femoral groove [3], while Grassi et al. also encountered 20% of varus-aligned trochleae in a navigation study with 110 arthritic knees [9]. In the present sample, which is by far the largest published, the mean value was valgus (1.6° ± 6.6°), but 39.4% of knees had a varus-oriented trochlea. Therefore, the consideration of a laterally oriented femoral trochlea as a standard feature of the femoral component should be approached with caution. High variability has been observed in the axial plane morphology of arthritic trochleae, too [12].
Riviere et al. reported a high degree of discrepancy between native and prosthetic trochlear alignment in kinematically aligned TKR, with a more valgus orientation of the latter [25]. In additional studies, this discrepancy was also shown for mechanical alignment [13, 26]; this could be interpreted as an inherent limitation of implant designs. Barink has already proposed a more truly anatomical femoral configuration, with a more medially oriented trochlea [2]. In fact, one of the implants with a neutral (0°) PTA showed good patellofemoral performance, with just 5.6% of residual anterior knee pain in a cohort of 1482 TKRs [7]. In addition, according to manufacturers, several models have a ‘widened trochlear angle’, in theory enabling the accommodation of a range of NTAs within a limited extent. Further analysis is warranted to determine the biomechanical and clinical impact of this concept. Besides that, the inception of patient-specific implants may represent a genuine solution to accommodate the wide variability of trochlear [20] and other knee parameters [22]. Longer follow-ups are required to evaluate clinical superiority [31], and a significant reduction in current costs is also required to permit more widespread use. Ultimately, manufacturing companies may need to take this wide variability into account, finding ways to accommodate outlying anatomies, and probably, offering a wider range of prosthetic trochlear orientations.
Positioning of the femoral component with a mild external rotation (3° according to Insall) has been a general recommendation to favor adequate patellar tracking in TKR [23]. However, a previous publication revealed that native trochleae were internally rotated in 27.1% of the cases [10]: external rotation of the femoral implant may exaggerate the NTA–PTA discrepancy. Moreover, it has been analyzed how femoral component rotation critically affects tibial rotation, ligament forces, retropatellar stress, and varus–valgus position [32], highlighting the narrow margin a surgeon has for balancing patellar tracking only by adjusting this parameter.
The results of this study suggest the NTA–PTA mismatch as a feasible cause for biomechanical imbalance and dysfunction. Hochereiter et al. concluded that “any valgisation in TKA will increase (…) lateral PFJ contact pressure” [11]; the present article highlights that PTA is indeed more valgus than native values. This mismatch can be only identified preoperatively by means of 3D CT analysis, allowing surgeons to anticipate a surgical planning to accommodate wide discrepancies. Navigation can also be of extreme usefulness, even if 3D CT is lacking. However, these routines are still not a standard procedure in many settings; a 2021 review revealed that the proportion of navigated TKR was only 32% in Australia (2019), 30% in Germany (2014), 6.3% in USA (2014), and 3% in the UK (2014) [28]; not to mention less wealthy regions. In consequence, substantial variations in NTA may be left unappreciated, potentially compromising current clinical outcomes.
This study has some limitations. Native data have been extracted from arthritic knees; it could be argued that the results are not a reflection of undamaged knees. This would occur only after some degree of bone loss due to advanced disease being present; patients in Australia generally present at early stages of OA, and the sample size would probably eliminate this theoretical deviation. Notwithstanding that, these knees are the ones requiring a replacement, and therefore, the comparison of such anatomical features to those of implants in use has been considered adequate. Either way, a previous study on healthy knees revealed a trochlear valgus orientation of 1° ± 5° [14], a result equally distant from the average PTA values. Another limitation was the inability to source PTA details of all implants currently on the market. Dejour et al. already sentenced that manufactures tend to provide scarce details in regard to trochlear parameters [5]. Nonetheless, it appears unlikely to have missed models with significantly different PTAs, as this would probably have been advertised as a genuine feature in the brochures available for all systems. Further, the authors acknowledge that there are other trochlear parameters such as congruity, depth, lateral height, and the patellar component shape itself that can influence balance, tracking, and functional outcome. Finally, the clinical correlation of patellofemoral complications and trochlear mismatch within the studied cohort has not been analyzed. The fact that this cohort encompasses the records of multiple surgeons across Australia, employing varied surgical protocols and implants, has hindered this analysis, which remains as a future objective. As a consequence, the clinical implications of the NTA–PTA incongruity are still to be defined.
留言 (0)