
記住我









The study was performed as a double-blind, parallel, randomized controlled clinical trial on volunteers with xerostomia referred to the School of Dentistry of Tehran Islamic Azad University of Medical Sciences in 2020. Purpose-based sampling was conducted among male and female volunteers aged 18 to 60 who were literate and suffering from xerostomia. Xerostomia was diagnosed when volunteers responded yes to four questions of the Fox questionnaire [26, 27]. The questions were as follows; 1) “Does the amount of saliva in your mouth seem to be too little, too much, or you do not notice it?” 2) “Do you have any difficulty swallowing?” 3) “Does your mouth feel dry when eating a meal?” 4) “Do you sip liquids to aid in swallowing dry food?” They were also asked about their problem’s severity regarding each question according to VAS (visual analog scale) from 1 to 10 and then converted to 0.1–1.
In addition, the exclusion criteria of the sampling included: 1) present pregnancy or lactation, 2) presence of an oral lesion, 3) infection or burning mouth, 4) use of prosthetic dentures, 5) history of previous contact dermatitis or allergic reaction caused by pilocarpine, connective tissue or systemic diseases affecting salivary gland function like Sjögren’s syndrome, Rheumatoid arthritis, systemic lupus erythematosus, progressive systemic sclerosis (PSS), 6) history of head and neck radiotherapy, 7) acquired immunodeficiency syndrome (AIDS), 8) hepatitis B or C, 9) hypertension (above 140/90 mmHg), cardiac or renal diseases, 10) Parkinson’s disease, 11) asthma, 12) chronic obstructive pulmonary disease (COPD), 13) glaucoma, 14) chemical or herbal medication and salivary enhancers intake, and 15) alcohol and tobacco products except for cigarettes [20, 25].
The present study’s protocol followed the Declaration of Helsinki. The ethics committee of the Islamic Azad University Faculty of Dentistry, Tehran, Iran (IR.IAU.DENTAL.REC.1399.282) also approved it on 03/03/2021, and it was subscribed to the Iranian registry of clinical trials (IRCT20210208050302N1). After explaining the steps to the volunteers, all eligible volunteers were asked to complete and sign the informed consent form to participate in the study. The participants were then asked to fill carefully in the demographic information form and the standard xerostomia questionnaire [27] to determine the individual’s initial xerostomia severity [26, 27].
Additionally, using PASS 15 software considering β = 0.2, α = 0.05, and a standard deviation of 0.85 to achieve the effect size of 0.52, the minimum sample size for each group was 16 [24]. The recruitment of volunteers took place from April 2021 to October 2021. After that, the 48 individuals were divided in a 1:1:1 ratio into three groups of 16 by simple randomization by Arezoo Alaee. The groups were almost homogeneous regarding age, gender, smoking, systemic disease, and educational status [20, 24].
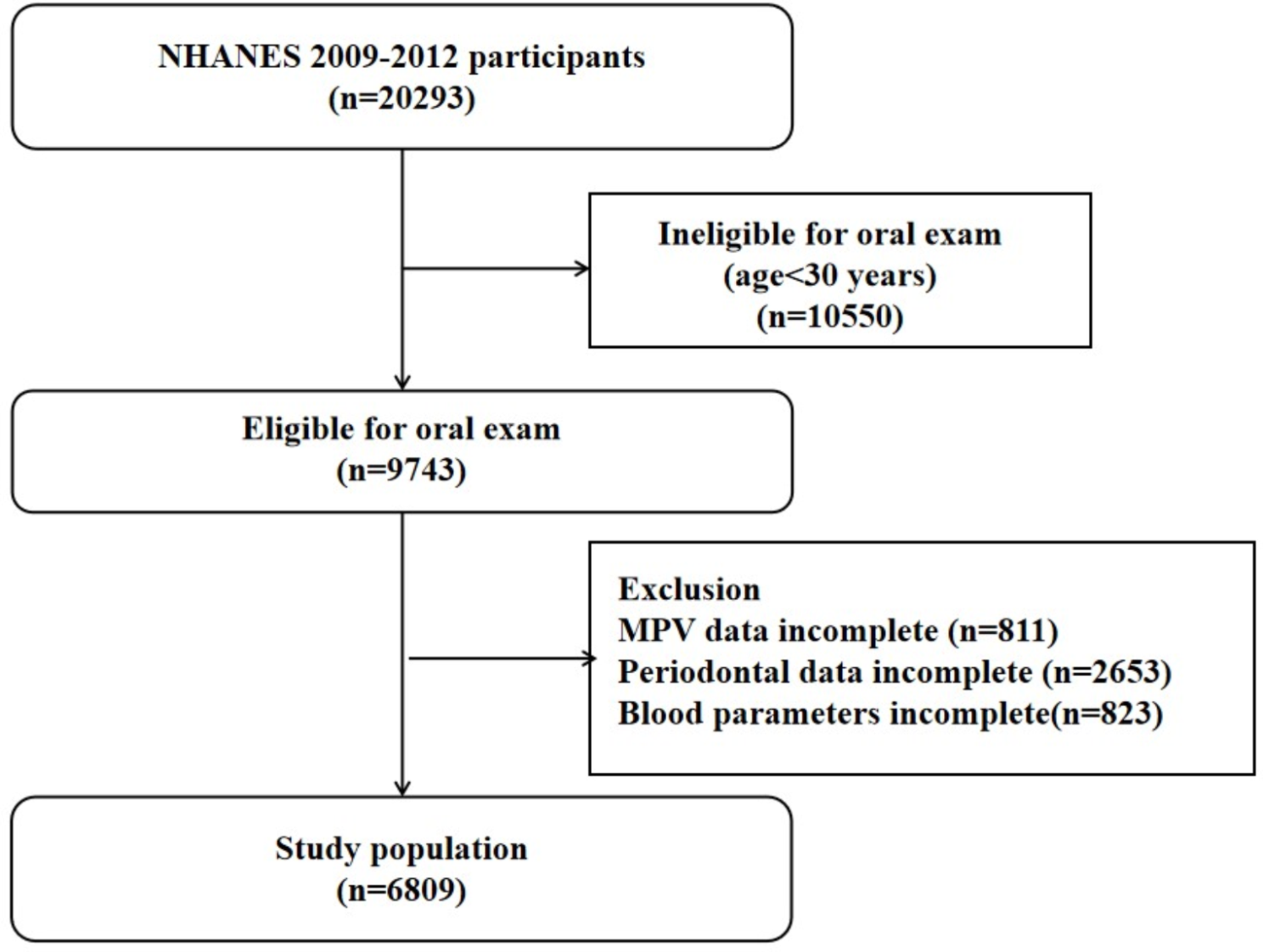
As demonstrated in the CONSORT flow diagram (Fig. 1), three types of medicinal intervention were administered:
1)Group A: 2% pilocarpine mouthwash, three times a day,
2)Group B: 1% pilocarpine mouthwash, three times a day, and
3)Group C: Placebo mouthwash, three times a day.
Fig. 1
Consolidated Standards of Reporting Trials (CONSORT) diagram of participants’ flow
Since pilocarpine 2 and 1% mouthwash was not available in the Iranian pharmaceutical market, it was prepared in the laboratory of the Pharmaceutical Sciences Research Center of the Faculty of Pharmacy, the Islamic Azad University of Medical Sciences, Tehran, Iran. The 4% pilocarpine eye drops (Glaupin® 4%, Sina Darou, Iran) were diluted with Vi-one junior mouthwash (Rojin Cosmetic, Iran) to prepare 2% pilocarpine mouthwash and improve the taste and acceptance of participants. Vi-one junior mouthwash is a flavored, alcohol-free product specially designed for kids that contains harmless sweeteners, disodium phosphate agents, 0.05% sodium fluoride, and 0.05% cetylpyridinium chloride [28]. Moreover, the 2% pilocarpine mouthwash was diluted with water to make 1% pilocarpine mouthwash. Furthermore, Vi-One junior mouthwash (Rojin Cosmetic, Iran) was diluted with water to create a similar taste and color as other mouthwashes for the placebo group.
It is worth noting that the pharmacologist author of the current study (Hoda Jahandar) coded the three types of mouthwashes and packaged them like each other. Hence, the participants and the researchers were unaware of the medicines in the package. Besides, high-performance liquid chromatography (HPLC) was utilized (SCL-10AVP, Shimadzu, Japan) to evaluate the stability of this product during the study period (14 days). It was considered that maintaining at least 90% of the area below the pilocarpine curve relative to day zero indicates product stability.
In addition, blood pressure (mmHg) and pulse rate (pulse per second) were recorded on the 1st and 14th day before and 75 mins after medicine application by a hand-held sphygmomanometer (KaWe, Germany). The participants’ weights were also measured with minimum clothing and without shoes with a ± 0.5 kg accuracy. A participant stood next to the wall without shoes, legs paired to each other, head leaning against the wall, to determine their height. Furthermore, body mass index (BMI) was obtained by dividing body weight (kg) by the square of a person’s height (m2) [16].
On the 1st day, the amount of unstimulated saliva was measured before mouthwash administration and 45, 60, and 75 mins after gargling the mouthwash for all three groups. The unstimulated saliva was measured by absorption or swab-based technique for participants before intervention. Additionally, the participants were asked to avoid eating, drinking, smoking, and brushing their teeth for at least 2 hrs before accurately measuring the amount of non-stimulated saliva. After rinsing their mouth with 15 ml of distilled water, the participants rested in a room with adequate comfort and ventilation for one min and sat upright on a dental chair.
Afterward, the volunteers in all three groups were asked to gently gargle 5 ml of their mouthwash solution for 1 min without swallowing the contents and then drain it completely. Then, observing the complete principles of sterilization and wearing a mask and face shield, the researcher (Babak Motamed) placed the previously weighed dry cotton roll (1 × 4 cm2) in the participant’s mouth. After 1 min, the researcher removed the wet cotton roll with dental pliers, placed it in a coded bag, and sent it to the laboratory for further weighing using a digital scale with ±0.01 g accuracy.
Saliva content (cc or gr/ml) = wet cotton roll weight - dry cotton roll weight.
All salivary measurements were carried out between 9 and 11 AM [29] as saliva secretion may fluctuate during the day. Saliva samples were kept at 4 °C to prevent further changes. The participants’ medication-related side effects were recorded on the first day using an 11-item questionnaire based on the VAS (visual analog scales) before the study [24, 30]. These 11 side-effects were 1) visual difficulties or blurred vision, 2) tremors, 3) indigestion and heartburn, 4) diaphoresis, 5) tachycardia, 6) anxiety, 7) headache, 8) hot flashes, 9) epiphora, 10) sialorrhea and 11) urinary frequency. The xerostomia questionnaire was also filled out again on the 14th day for all three groups of participants. Furthermore, saliva was measured on the 14th day at 0, 45, 60, and 75 mins. On the 14th day, possible side effects of the volunteers based on VAS were also recorded at 0 and 75 mins.
Besides, during these 14 days, the participants had constant contact with the researchers through phone calls to find answers to their questions or possible problems. The participants were also barred from taking medicines that relieve dry mouth or increase saliva. However, water intake, chewing gum, and topical local anesthesia agents were unimpeded.
Statistical analysisSPSS software version 26 was used for data analysis. Moreover, Kolmogorov–Smirnov test was used to determine the normality of the data. Chi-square, one-way ANOVA, repeated-measures ANOVA, Tukey, and Independent Samples T-Test were also employed to analyze the data. In addition, values less than 0.05 were considered statistically significant.
留言 (0)