
記住我
What is known about the topic?
Mentoring has been used by nursing and medicine to improve knowledge translation capability. Benefits of mentoring have included improved clinician knowledge. It is not known how allied health professionals have used mentoring as a knowledge translation strategy to improve the use of research in practice.What does this article add?
Allied health professionals have used mentoring as a knowledge translation strategy. Mentoring has been used to support the implementation of research into practice, but also to teach the processes of knowledge translation. Mentoring has mostly been used by allied health professionals alongside other knowledge translation strategies such as education. IntroductionA core principle of being an evidence based health care professional is the use of research evidence to inform decision making.1 This process is known as knowledge translation.2–5 Using research evidence to inform practice has resulted in improved health outcomes for healthcare recipients.6 Alternatively, poor knowledge translation practices can result in a delay of care7 or healthcare consumers receiving interventions which are harmful or not effective.8 Due to the difficulties for health care professionals in identifying and appraising the research evidence9 and the presence of implementation barriers which can exist in a local health care context,10,11 translating research into practice can be challenging and complex.4,5Allied health professionals use multiple knowledge translation strategies to overcome the barriers to implementing research evidence into practice.12 Mentoring is one such strategy to support the translation of research into practice,13 and is the focus of this scoping review.
Mentoring is a process to provide support to an individual who has identified learning needs related to a specific topic.14 A mentor is considered to have established knowledge and skills in the relevant topic,13 and the mentee is the person with the learning needs.15 The strategy of mentoring differs from other professional supports such as coaching and clinical supervision. In contrast to coaching, mentoring uses interpersonal relationships to the benefit of both the mentor and mentee.16 While both mentoring and clinical supervision include a focus on learning and professional support, the scope of clinical supervision usually includes restorative, administrative and evaluative functions.17,18 The reported benefits of mentoring include being able to deliver positive clinical outcomes,15 improve the communication skills of clinicians,19 career advancement of mentees and mentors13 and the ability to create change in a work setting.14 Alongside the reported benefits, challenges associated with mentoring have been reported when there is poor quality of communication in the mentor/mentee relationship or due to ineffectual mentoring program structures.19
The benefits of mentoring as a knowledge translation strategy have been explored in one systematic review including health professionals20 and one scoping review including disciplines from the social sciences.21 Within the included studies of the previous reviews, neither identified mentoring as being used by any of the allied health professions.20,21 However, the systematic review of randomized control trials reported that the included studies demonstrated an improvement in clinician knowledge, clinician evidence-based practice beliefs and organizational capability.20 Furthermore, the review reported varying levels of efficacy in changing professional behavior and clinical outcomes after health professionals were involved in a mentoring program. The findings support using mentoring as a knowledge translation strategy in healthcare.20
The characteristics of mentoring as a knowledge translation strategy have been described as related to medicine, nursing and social sciences disciplines.20,21 The duration of mentoring was reported to span from one to 24 months, and the number of sessions completed ranged between two and 10 sessions. Mentoring was also described as a standalone strategy or in combination with other knowledge translation strategies such as education and skills training. The mentoring intervention was included in interventions labeled as opinion leaders, academic detailing or mentoring. Mentoring was delivered in a group, face to face or in combination with electronic formats. Additionally, variation in the structure, goals and content of mentoring exist.20,21 As neither of the knowledge synthesis studies included allied health professionals, it is not known how the combined knowledge of using mentoring as a knowledge translation strategy relates to allied health. To date there has been no synthesized study investigating how mentoring has been used as a knowledge translation tool by allied health professionals.
The primary objective of this review is to describe allied health mentoring strategies which aim to improve knowledge translation capability. In doing so, a description will be given about the characteristics of mentoring, how mentoring's impact is being measured, and what enables or impedes the use of mentoring as a knowledge translation strategy.
Review question(s) i. How has mentoring been used by allied health professionals to enable the use of research knowledge in practice? ii. What are the barriers to using mentoring as a knowledge translation strategy? iii. How has the impact of mentoring been measured? Inclusion criteria ParticipantsThe review considered studies that included participants from allied health disciplines as described by the Australian Government Health Workforce Program.22 If studies also included participants from medical or nursing professions, only those studies where the majority of participants were allied health were included.
As this review focused on the use of mentoring by qualified allied health professionals employed in healthcare settings, studies were excluded if they reported that participants were in the majority students.
ConceptThis review included studies that explored the concepts of both mentoring and knowledge translation.
For a study to be considered as investigating mentoring, it needed to demonstrate (a) involvement of at least one mentor and one mentee, (b) an interactive process over time between a mentee and a mentor, and (c) a mentoring relationship aiming to promote a benefit for the mentee. Mentoring could be used as either a singular or as a part of a multi-faceted strategy for knowledge translation.
For a study to be considered as investigating knowledge translation it needed to report on an outcome or experience relating to the use of research evidence in a health care setting. Outcomes that could be reported on included behavior, knowledge, policy or clinical outcomes. Experiences could describe the perceptions and viewpoints of allied health professionals who were participating in mentoring to influence the use of research evidence in practice.
The review excluded a study if mentoring was solely supporting allied health professionals to conduct research activities in a health care setting.
ContextThis review considered studies in healthcare settings where mentoring enabled knowledge acquisition and/or knowledge translation skills of allied health. Studies could include participants of any gender, geographical location, cultural background and health care setting.
Types of sourcesThis scoping review considered quantitative, qualitative and mixed methods study designs for inclusion. Knowledge synthesis reviews and grey literature that met the inclusion criteria were eligible. Opinion papers were not eligible for inclusion.
MethodsThis scoping review was conducted in accordance with the JBI methodology for scoping reviews23,24 and has been written using the JBI System for the Unified Management, Assessment and Review of Information (JBI SUMARI).25 This review was conducted in accordance with an a-priori protocol.26
Search strategyThe search strategy aimed to locate both published and unpublished primary studies and reviews. An initial limited search of MEDLINE (Ovid) and CINAHL (EBSCO) was undertaken to identify articles on the topic. The text words contained in the titles and abstracts of relevant articles, and the index terms used to describe the articles, were used to develop a full search strategy. The search strategy, including all identified keywords and index terms, was adapted for each included information source. The final search was repeated on 9 March 2021. The full search strategy is provided in Appendix I, https://links.lww.com/IJEBH/A90. The reference lists of eligible studies included in the review were screened for additional papers.
Only studies published in English were included. Studies published from database inception to the date of the search were included as to identify all eligible research.
The databases that were searched were: MEDLINE (OVID), EMBASE (OVID), CINAHL (EBESCO), PscyhInfo (OVID), PDQ-Evidence (www.pdq-evidence.org), and Cochrane. The source of unpublished studies and grey literature was Open Grey (www.opengrey.eu/).
Study/source of evidence selectionFollowing the search, all identified records were collated and uploaded into EndNote (Clarivate Analytics, PA, USA) and duplicates removed. Following a pilot test, titles and abstracts were screened by two independent reviewers for assessment against the inclusion criteria for the review. Potentially relevant papers were retrieved in full and their citation details imported into the Covidence Systematic Review Management platform27 and those that did not meet the inclusion criteria were excluded. A full list of exclusion reasons is provided in Appendix III, https://links.lww.com/IJEBH/A90. Any disagreements that arose between the reviewers were resolved through discussion or with the involvement of a third reviewer.
Data extractionData were extracted from included studies by two independent reviewers (OH and CO) using a data extraction tool (for a copy of the tool, refer to Appendix II, https://links.lww.com/IJEBH/A90) developed by the reviewers. A framework developed by Karcher et al.28 was used to inform the mentoring characteristic section of the data extraction tool. The data extraction tool collected information concerning the allied health participants, study design, research evidence being translated into practice, mentoring characteristics (context, structure, goals, content, required infrastructure and dosage), barriers and facilitators to using mentoring as a knowledge translation strategy and how mentoring impact was measured. Barriers and facilitators were extracted verbatim onto the extraction form, then a consensus agreement was made between two authors regarding how these barriers would be paraphrased in the scoping review table.
Authors of studies were contacted to request missing or additional data where required.
Data analysis and presentationThe extracted data are presented as narrative descriptions and in tabular form. Table 1 provides a summary of included trials, Table 2 describes mentoring characteristics and Table 3 presents the facilitators and barriers to using mentoring as a knowledge translation strategy.
Table 1 - Summary of included trials Author (year) Methodology Data collection method Participants Translated evidence Measurement of the multifaceted strategy Measurement of mentoring Anaby et al. (2015) Qualitative Individual interviews Occupational therapists (n = 8)Physiotherapists (n = 3)Psychologist (n = 1)Specialized educator (n = 1)Speech pathologist (n = 1) Participation in community leisure occupations by children with disabilities N/A Professional evaluation and reflection on change tool Ashburner et al. (2015) Mixed Self-report surveys Occupational therapists (n = 42) Occupational therapy assessment and intervention techniques for children and adolescents with a diagnosis of Autism Spectrum Disorder Self-rated questionnaire on knowledge and confidence Self-rating questionnaire enquiring about mentoring usefulness Banerjee-Guénette et al. (2019) Mixed Self-report surveys and forms Physiotherapists (n = 7)Occupational therapists (n = 3)Rehabilitation assistant (n = 1) VR and active video gaming VR usage data collection formSelf-report questionnaire to identify technology usage patternsADOPT-VR2 to measure the adoption of VR technology by therapists N/A Bennett et al. (2016) Qualitative Case report Occupational therapists (n = 20) Knowledge to action framework Case study reportingStaff attrition N/A Campbell et al. (2013) Quantitative Outcome measures Physiotherapists (n = 32)Occupational therapists (n = 49)Speech pathologists (n = 36)Psychologists (n = 8)Social workers (n = 10) Evidence-based practice behavior as related to cerebral palsy research Self- and peer-rated EBP behavior was measured using the Goal Attainment ScaleKnowledge and attitudes were measured using exams and the Evidence-based Practice Attitude Scale N/A Ferro and Quinn (2020) Mixed Self-report surveyAudit of written goals Physiotherapists (n = 22) Goal setting Self-rated questionnaire on perceptions about goal settingGoal evaluation Self-rating questions enquiring about mentoring usefulness Fritz et al. (2019) Mixed Time use logs, individual interviews and researcher notes Physiotherapists (n = 15) Behavioral physiotherapy N/A Time allocation and rank score of facilitation methodsInductive content analysis of interviews McCluskey et al. (2020) Quantitative Before and after study Occupational therapists Constraint induced movement therapy No. of participants receiving constraint induced movement therapyNo. of repetitions per sessionUpper limb outcomes N/A Molfenter et al. (2009) Qualitative Case study design Speech pathologists (n = 4) Surface electromyography biofeedback N/A Qualitative interview questions enquiring ‘What was the influence of having mentorship available?’EBP, evidence based practice; N/A, not applicable; VR, virtual reality.
KT, knowledge translation; KTA, knowledge to action; sEMG, surface electromyography; VR, virtual reality.
KT, knowledge translation.
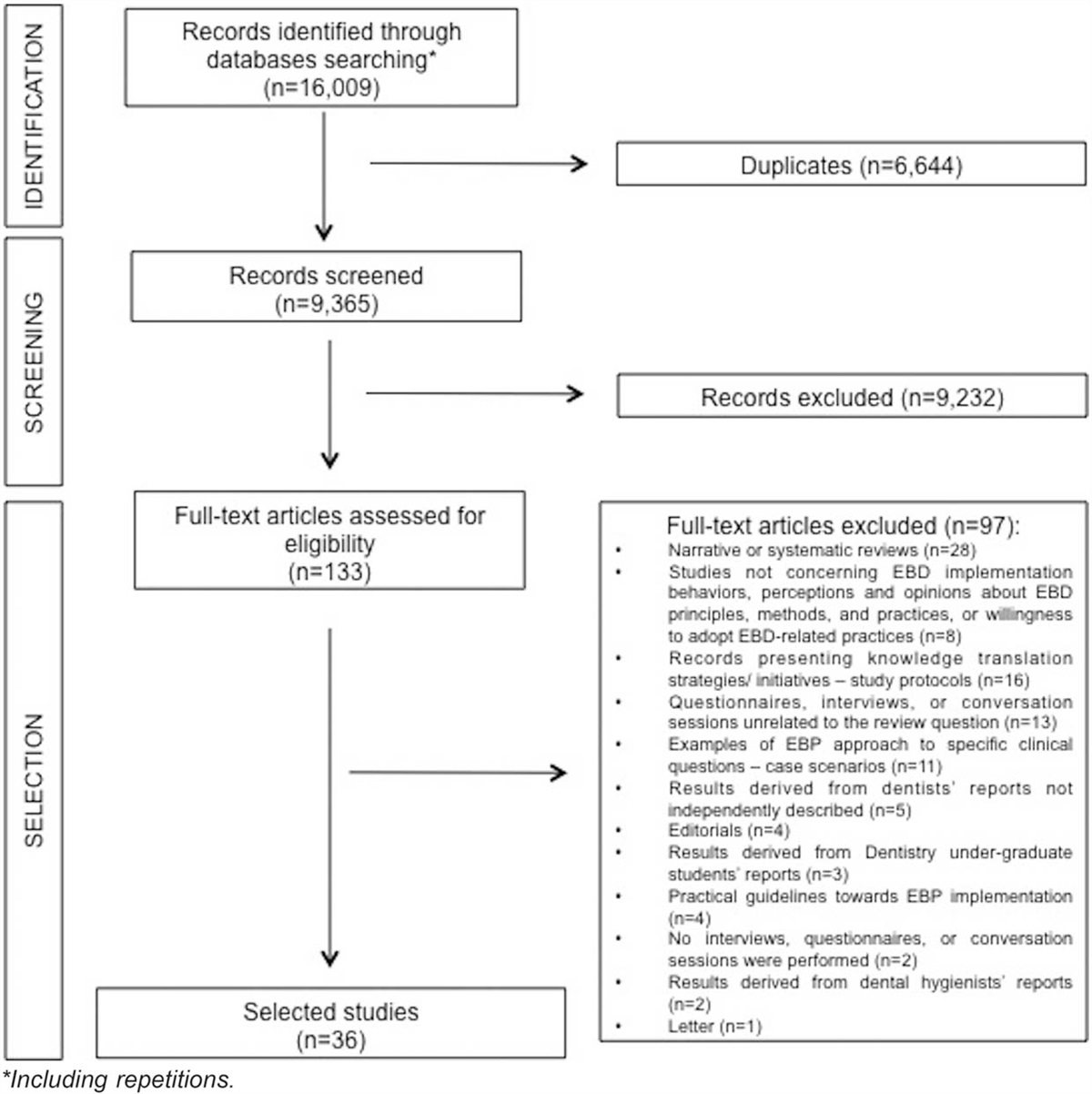
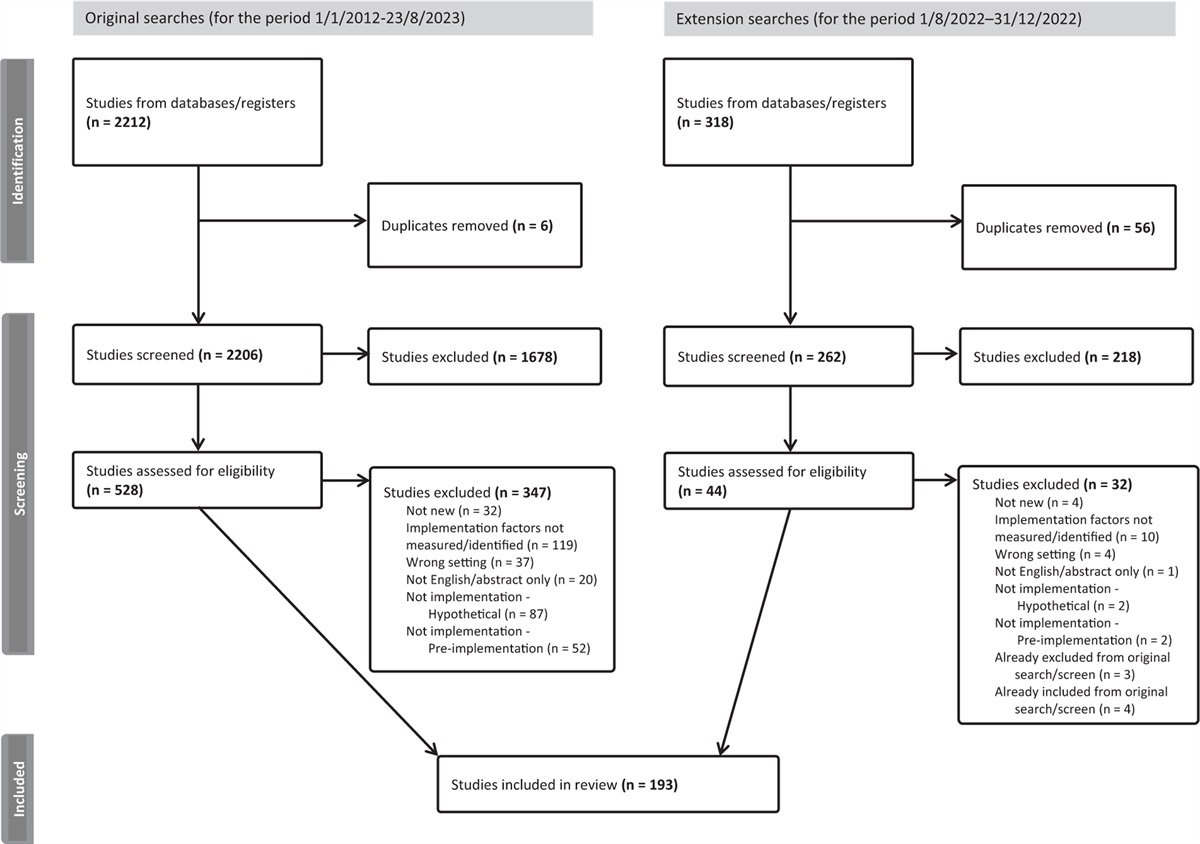
The search identified 2053 citations after duplications were removed. After screening title and abstract, 1956 were excluded from the review. A review of reference lists identified three potential further studies for inclusion for full text review screening. After full text review, nine studies were eligible for inclusion (refer to Fig. 1 for PRISMA flow chart showing flow of trials with reasons for exclusion). A full list of reasons for inclusion and exclusion at full text stage is provided in Appendix III, https://links.lww.com/IJEBH/A90.
 Figure 1:
Figure 1: Search results and study selection and inclusion process.
Characteristics of included studiesRefer to Table 1 for a description of the characteristics of included studies.
Study designData collection methods varied; two studies reported a quantitative approach,29,30 three studies used qualitative methods30–32 and four studies reported a mixed methods approach.34–37 Data collection methods included individual interviews,31,32,36 self-report surveys,34,35,37 case reporting,33 outcome measures,29 fidelity measures,30 time use logs,36 researcher notes,34 forms35and case reports.35
Translated evidenceThe research supporting targeted evidence-based practice was reported in eight studies,29–32,34–37 whereas one study reported the translation of the research evidence supporting a knowledge translation process.33
Measuring the impact of mentoringThe impact of the specific component of mentoring was measured in five studies31,32,34,36,37 establishing the mentee's experience and view point about the mentoring used. The impact of the multifaceted knowledge translation strategies including mentoring was measured in six studies.29,30,33–35,37 These included the measurement of interventional research knowledge,33 intervention adoption measures30,35,37 and evidence-based values and behaviors.29 A complete list of outcome tools used for measuring impact are listed in Table 1.
The characteristics of mentoring as a knowledge support strategyA complete description of mentoring characteristics described in included studies is provided in Table 2.
ContextMentoring as a knowledge translation strategy by allied health has been investigated in the United States of America,37 Australia,29,30,33,34 Canada31,32,35and Sweden.36 A range of settings were described including regional,30,34 metropolitan30,33,34 and urban environments.35
StructureMentoring was primarily delivered on an individual basis,29,30,32,34–37 although two studies used mentoring in a group environment.31,33 Participants in mentoring programs included those from single disciplines 30,32–34,36,37 or multiple disciplines.29,31,35 Mentoring was used by occupational therapists,29–31,33–35 physiotherapists,29,31,35–37 speech pathologists,29,31,32 rehabilitation assistants,35 psychologists29,31 and social workers.29 An expert mentor was provided in eight of the studies.29–33,35–37 Two studies reported using a peer-mentoring structure, with each mentee also acting as a mentor in the mentoring relationship, as they were acknowledged as having clinical expertise as well as learning needs.30,34 Mentoring was predominantly used as part of a multifaceted knowledge translation strategy.29,30,32-37
For the studies which used additional knowledge translation strategies alongside mentoring, the number of other knowledge translation strategies ranged from two32 to 10.33,36 Only one study reported mentoring as the sole knowledge translation strategy.30
The goal of the mentoring programAll of the included studies reported that the common goal of mentoring was to facilitate the learning of knowledge and skills from the research being translated to clinical practice.29–37 The range of mentoring goals are described in Table 2.
Mentoring contentMentoring included multiple individual activities across all studies.29–37 Mentoring activities with similar content included the use of case studies to direct mentoring discussions,31,33 content that was directed by learning goals,31,33–35 providing feedback about videotaped intervention sessions,34,35 barrier identification29,30,32 and problem solving issues that were discussed.29,32,33,36
InfrastructureResources described to support mentoring included a workbook,33,34 a self-monitoring diary,36 stickers to highlight important strategies to learn,36 mentoring guidelines,34 specialized intervention equipment,32,33 educational material,35–37 protected time,29,32,36 video recording equipment,34,36 embedded outcome measurements within workflow,29 reference lists,37 normative data tables37 and client documentation infrastructure.29
DosageThe number of contacts between a mentor and mentee/s varied from two to nine.31,33–37 Contact delivery spanned between two and six months,33,34,36 and each contact lasted between 33 and 120 min.30,31,34,35
Barriers and facilitators to using mentoring as a knowledge translation strategyThe barriers and facilitators are reported in Table 3. In total, 10 individual barriers for using mentoring as a knowledge translation strategy were listed, spanning three studies.32,33,35 Those barriers included the ever changing departmental staffing profile impacting staff engagement,33 patients declining to be involved in key activities which were to be used in the mentoring sessions36 and difficulties in scheduling suitable times for people to meet.34 Four distinct facilitators were identified,31,32,34 including the mentor actively acknowledging the mentee's values and the mentee's level of knowledge31 and the mentor's awareness of the research supporting the interventional technique.32
DiscussionThis scoping review confirms that allied health professionals have used mentoring as a knowledge translation strategy29–37 and adds to the existing knowledge that mentoring as a knowledge translation strategy has been used in the fields of social science, medicine and nursing.20,21 This review demonstrates that allied health have predominantly used mentoring as one component of a multi-strategy approach to enable the translation of research evidence.29,32–36 Multifaceted knowledge translation strategies have been frequently reported in allied health literature,38 however, the incorporation of mentoring as a knowledge translation strategy has been reported more frequently in the past seven years.29–31,33–37 While the use of multifaceted strategies have not been identified as superior to singular strategies to date,39 they provide the opportunity for strategies to be targeted and tailored to overcome the barriers to translating evidence into practice.10
The findings from this review demonstrate that allied health professionals have used mentoring for two main purposes as related to knowledge translation. In one group of studies, allied health professionals used mentoring to facilitate the translation of specific interventional research evidence,31,32,34–36 for example surface electromyography32 or virtual reality.35 In the second group of studies, mentoring was used to facilitate the establishment of skills and knowledge related to applying the research evidence into the everyday practice context alongside the translation of research evidence specific to clinical topics.29,33 Regardless of the type of evidence being translated, various stakeholders, such as the mentee,31 mentor,34 organization29,33 and the health care consumer,36 were actively involved in engaging in the mentoring process.
Similar to previous reviews including those in social science disciplines, nursing and medicine,20,21 the characteristics of allied health mentoring as a knowledge translation strategy were broad ranging in relation to its context, goals, structure, content and dosage. Regardless of the context or structure, this scoping review identified that mentoring was accompanied by an educational and training component delivered either individually36 or in a group setting.29,31–35,37 Educational strategies alone have previously been reported to have limited influence on changes to clinician's knowledge and behaviors.40,41 Therefore, the tailored use of mentoring alongside educational workshops may provide benefit to the mentee in the form of a flexible approach to their learning needs whilst providing a mechanism to model desired behaviors and knowledge acquisition.13
In the studies which reported the use of mentoring as a knowledge translation strategy by allied health professionals, few studies reported the barriers33,34,36 or the facilitators31,32 to delivering a mentoring knowledge translation strategy. The barriers of mentoring varied,33,34,35 whereas the facilitators of mentoring were related to the approach and expertise of the mentor.31,32 Previous knowledge synthesis studies about the use of mentoring as a knowledge translation strategy by nursing and medicine also reported that very few studies have investigated the components which impede or facilitate the use of mentoring.20 Our findings reinforce that there is very little understanding to how the mentoring relationship, and the structure of the mentoring program, influences the capability of mentees to translate research into practice.
Future studies focusing on the use of mentoring to support knowledge translation would be strengthened by considering a broader range of outcome measures to quantify the impact of mentoring when it is used as a stand-alone strategy. This review has found that when considered as an individual strategy, mentoring was only measured from the perspective of a clinician's experience.32,35,36 In contrast, the multifaceted strategies that involved mentoring measured a range of aspects of impact such as clinician behavior,34 intervention adoption
留言 (0)