
記住我
What is known about the topic?
Stroke can cause physical dysfunction and impaired ability of daily living. In addition to medical expenses, caregivers often undertake various complex tasks, and roles. Caregivers experience tension, stress, and fatigue, which may affect the long-term prognosis of patients after stroke. Family resilience can help family caregivers facing the consequences of adversity and stress to have a positive outcome. Assessing resilience and intervention is essential to family caregivers of stroke in community; however, it is not commonly implemented due to various barriers.What does this article add?
Standardized, evidence-based family resilience care project for family caregivers of stroke in community should be implemented. Based on transformational leadership theory, integration of implementation strategies to build consensus and develop the nurses’ commitments contributed to the success of this implementation project. The current evidence-based practice project demonstrated how to develop resilience evidence translation care standards with the key stakeholders to implement best practice standards for family caregivers of stroke in the community. IntroductionStroke is the main cause of disability among many chronic diseases. Stroke is the in top 10 causes of death.1 Particularly, stroke remains the second leading cause of death worldwide, with 5.5 million deaths attributed to this cause in 2019.2 The rate of disability after 1 month of stroke is as high as 61.2, and 51.72% after 6 months. Regardless of the type of ischemic stroke or hemorrhagic stroke, about half of stroke patients are disabled 1 or 3 months after the stroke.3–5
With the aging population, increasing rates of chronic illness, and the emphasis from institutional to home-based care, caregiver support is increasingly important, particularly within the area of stroke, considered the most common disabling chronic condition.6–8 Caregivers who experience tension, stress, and fatigue9,10 may affect the long-term prognosis of patients after stroke. The research shows that primary caregivers have a 63% higher risk of death after 4 years than nonprimary caregivers.11 The stroke patients and the caregiver are intertwined and affect each other in their lives. That will be an important reason to promote resilience of the family caregiver.
The current study was based on the Program from Pei-Fan Mu's Project title: ‘Recreating an opportunity for the caregiver of patients with stroke’ by the Department of the Ministry of Health and Welfare, Taiwan, ROC.12 The family caregivers of patients with stroke should receive psychosocial support throughout the stroke recovery care to ensure the sustainability of the care arrangement and enhance caregivers’ wellbeing. Resilience is the ability to recover quickly from an illness, calamity, or change, and is a ‘positive adaptation’ after a stressful or adverse situation.13,14 Resilience is a positive perspective to stimulate the superior strength of family caregivers. Resilience helps family caregivers facing the consequences of adversity and stress to have a positive outcome.15–19 The family caregivers suffering from stroke at home can not only help family caregivers to recognize the family functions to increase confidence but also enable family caregivers to understand the existence of the family; from the moment the stroke patient is discharged from the hospital, the primary caregiver is faced with the responsibility of independently caring for the disabled patient, worrying about the patient's prognosis, disability, and affecting family stability and physical, mental stresses.
The current implementation project was conducted at a home care service of the National Yang Ming Chiao Tung University Hospital. There were nine home care nurses. They have on average 10.5 years’ experience of nursing. The average number of cases receiving home care service per month is about 320, and the average number of home visits per month is 600; stroke patients account for about 60% of the home care cases. The home care service only provides regular home care for stroke patients, and we regularly evaluated the Zarit caregiver burden interview (ZBI) for caregivers of patients with stroke.18 ZBI score was designed by Zarit in the 1980s and was translated into Chinese by Lie Wang in 2006.19 ZBI score includes two dimensions (personal burden and responsibility burden) of 22 entries. The reliability coefficient (Cronbach's Alpha) of ZBI (Chinese version) is 0.87. ZBI score uses the five-level rating method, and the total score is 0–88. The burden level can be divided as follows: less than 21 means mild or no care burden, 21–39 means moderate care burden and more than 40 means severe care burden. On analysis of Care Burden Scale assessment data in 2020, we found that most of the caregivers for patients with stroke had moderate care burden. The care burden level was 27.7%. Therefore, the family caregivers of stroke patients take the moderate severe to severe disability reported higher scores.
There are some problems that are currently prevalent in the clinic. The caregivers provide for the long-term care of postsurvivors and have replaced care from healthcare systems. The core processes in family resilience are mutually interactive, both within and across domains. For example, shared meaning-making facilitates communication clarity, emotional sharing, and problem-solving; and effective communication processes facilitate shared meaning-making.20 This study that was conducted also has the problems of home care service and mainly focuses on the physical care of patients with stroke, mainly for caregivers’ long-term care and referral of social resources. There is lack of care and guidance on the psychosocial level of caregivers, and there is no assessment or promotion related to the resilience of the primary caregiver. Home care nurses lack the importance of resilience assessment and care for primary caregivers. To assess what consequences these problems lead to, and what the best evidence suggests should be done to address these problems, this team used the assessment and management of the family resilience of the primary caregivers of stroke patients at home care recommended by JBI for evidence translation and implementation. The team implemented JBI's recommendations include the following:
(1) Caregiver Resilience: Assessment (a) Evidence indicates there is no gold standard measure to assess resilience and the choice of measure should take into consideration the dimensions assessed and the psychometric properties of the instrument [e.g.,: CD-RISC, RSA, Brief Resilience Scale (BRS), PCQ] (Grade A). (2) Stroke (Older Adults): Family/Caregiver Resilience Interventions in Community Settings (a) Support programs should include relative and friend support, social support (practical, emotional, and moral), family-coping coherence strategies, and education (Grade B). (b) Community-based support programs may be used to enhance resilience for families of an older adult with poststroke dysfunction (Grade B). (c) Support programs should include psychoeducation and practical, emotional, and moral support from family and friends (Grade B).Regarding institutional barriers, the Criterion 3 Support programs should include psychoeducation and practical, emotional, and moral support from family and friends. Currently, this project is only focusing on the home care situation, thus, we are only focusing on the (1) Caregiver Resilience: Assessment, and (2) the first two audit criteria of Stroke (Older Adults): Family/Caregiver Resilience Interventions.
Objective(s)The aim of this evidence implementation project was to contribute to promoting the evidence-based practice of the resilience model for primary caregivers of stroke patients at home. The following were the specific goals:
(1) To conduct a baseline audit determining current compliance, identifying barriers and facilitators to achieve compliance, and developing strategies to address areas of noncompliance with best practice for family caregivers of stroke in the community. (2) To increase resilience of the primary caregivers of stroke patients at home by improving their knowledge of best practices for resilience. (3) To improve the implementation of the resilience model as part of the evidence-based translational care program for primary caregivers of stroke patients at home. (4) To undertake a follow-up audit to assess the extent of compliance with evidence-based practice project for primary caregivers of stroke patients at home. MethodsThe current evidence implementation project started from 1 September 2018, to 30 September 2020. This evidence implementation project used the JBI Practical Application of Clinical Evidence System (JBI PACES) and Getting Research into Practice (GRiP) audit and feedback tool. The JBI PACES and GRiP framework for promoting evidence-based healthcare involves three phases of activity:
(1) Establishing a team for the project and undertaking a baseline audit based on criteria informed by the evidence. (2) Reflecting on the results of the baseline audit and designing and implementing strategies to address noncompliance found in the baseline audit using the JBI GRiP framework. (3) Conducting a follow-up audit to assess the outcomes of the interventions implemented to improve practice and identify future practice issues to be addressed in subsequent audits. Ethical considerationsThe current project was considered a quality improvement project within The National Yang Ming Chiao Tung University Hospital in Taiwan and has received ethical approval (IRB 2019A003).
Phase 1: Stakeholder engagement (or team establishment) and baseline auditPhase 1 involved establishing a quality improvement project team consisting of various stakeholders with evidence-based practice to promote the family caregivers of stroke patients. The team members were engaged early in the process to identify the setting and sample size and to conduct the baseline audit.
Establishment of the audit teamThe JBI implementation approach is grounded in the audit and feedback process along with a structured approach to the identification and management of barriers to compliance with recommended clinical practices. A core group of key stakeholders was formed to support the work of this project. The project team consisted of the project leaders (the deputy director and the head nurse), and eight nurses at the home care service. Each of the members within the team had their roles and responsibilities. The project team carried out a training course and a consensus meeting regarding the current evidence summary available for home care, PACES steps, teaching, and learning methods. It used the Objective Structured Clinical Examination (OSCE) skill test designed to assess the presence of nurses in education sessions and their knowledge of management strategies. The project leader was responsible for undertaking the JBI Clinical Fellowship Program and overseeing the project. Professor Mu, the JBI group, and project leaders also designed and carried out a formal education session of the Ministry of Health and Welfare about home care adequacy management during the project's second phase. The eight nurses were responsible for designing the nursing strategy and training and the quality control of the evidence-based resilience adequacy management practices in the units, which were implemented during and after the implementation project. The project leaders were responsible for education on the resilience for an evidence-based translational care model of home care management. A baseline audit to assess the unit's current adequacy resilience care practices using the JBI-PACES program was conducted from 1 September 2018 to 30 September 2020, with team training held in the first week of March 2018.
We followed three evidence-based audit criteria (Table 1). We used various methods to collect data, including a documentation review.
Table 1 - Audit criteria, samples, and methods to measure compliance with resilience evidence care model for caregivers of stroke patients Audit criteria Sample Method used to measure % compliance with best practices (1) Evidence indicates there is no gold standard measure to assess resilience and the choice of measure should take into consideration the dimensions assessed and the psychometric properties of the instrument (e.g., CD-RISC, RSA, BRS, PCQ) (Grade A) Eight home care nurses The rate of completion of resilience assessment tools for primary caregivers of stroke patients at home (BRS, 15 min) (%)Monitoring method: the head nurse evaluated the nursing records of eight home care nurses. The home care nurses who conducted assessments of primary caregivers of stroke patients at home were purposively selected. The rate of completion of resilience assessment tools for primary caregivers of stroke patients at home (BRS, 15 min)First, if the home care nurse administered a resilience assessment tool (BRS, 15 min) for all primary caregivers, ‘Yes’ who recordSecond, assessment of monitoring items in the resilience assessment tool (BRS, 15 min) for primary caregivers. Was a resilience assessment (BRS) completed in the first home visit (1–2 weeks)? (yes/no)Goal: 100% rate of completion for resilience assessment tools for primary caregivers (BRS, 15 min) (2) Support programs should include relative and friend support, social support (practical, emotional, and moral), family-coping coherence strategies and education (Grade B) Thirty caregivers of stroke patients at home Assessment of the health education of 30 caregivers of stroke patients at home after the caregivers received care. The head nurse assessed caregiver health education through telephone communicationFirst, did the primary caregivers receive psychoeducation from home care nurses (yes/no)? The content of the intervention plan (weeks 1–8) for primary caregivers included stress management, problem solving skills, and finding care resourcesSecond, was the psychoeducation received by the primary caregivers from home care nurses helpful for stress management (yes/no)? If related health education was not received, this question was not applicableThird, was the psychoeducation received by primary caregivers from home care nurses helpful for developing problem solving skills (yes/no)? If related health education was not received, this question was not applicableFourth, was the psychoeducation received by primary caregivers from home care nurses helpful for finding care resources (yes/no)? If related health education was not received, this question was not applicableGoal: 85% compliance with the care plan based on the checklist for the resilience care plan (weeks 1–8) for primary caregivers of stroke patients at home (3) Community-based support programs may be used to enhance resilience for families of an older adult with poststroke dysfunction (Grade B) Thirty caregivers of stroke patients First, the percentage of home care nurses who completed 20 h of training for the resilience model within the translational care program for primary caregivers of stroke patients at homeSecond, checklist for the resilience care plan (weeks 1–8) for primary caregivers of stroke patients at home to monitor the rate of implementation of the care planGoal: 100% of home care nurses complete 20 h of training for the resilience model within the translational care program for primary caregivers of stroke patients at homeBRS, Brief Resilience Scale.
The evidence literature shows that older adults with poststroke dysfunction can use community support programs to increase resilience. Community support plan suggestions include relatives, and friends, support, social support, family adjustment strategies, and education. This plan is part of the opportunity plan for recreating the primary caregivers of stroke patients in the Ministry of Health and Welfare's 107 ‘Clinical Care and Guidance Training Program for Nursing Institutions Empirical Application’ by Mu et al.12 The program establishes guidelines for the empirical care plan for returning home stroke patients, develops a ‘family resilience model for the main caregivers of stroke patients’, and provides on-the-job education for home nurses and health education for the primary caregivers of stroke patients. The model for promoting family resilience of the primary caregivers of stroke patients includes two parts:
The first part is assessing the needs of the primary caregivers and the family, including first, applying Calgary's 15-min family assessment. The assessment content includes establishing therapeutic relationships, therapeutic dialogue, and storytelling, family genogram (including ecomap), understanding the development of the family's internal and external structure, and consulting on therapeutic issues that the primary caregivers actively mention. The second consideration for the primary caregivers of stroke patients consists of the information needs of the primary caregivers for self-management, emotional needs, and social participation needs23–25. The needs assessment questionnaire will be used for the needs assessment of the primary caregivers of stroke patients, which consist of the information needs of the primary caregivers for self-management, emotional needs, and social participation needs.
The second part is to provide nursing consultation and health education. Intervention measures that will strengthen resilience after assessment include assessing the resilience and needs of caregivers, coordination of internal resources in the family, interactive communication within the family, problem-solving and positive thinking, and consultation and health education for the primary caregivers to restore care. Following this healthcare intervention, the main goal of the implementation team was to strengthen the degree of resilience.23,25–27 This project uses two JBI evidence summaries of Caregiver Resilience: Assessment and Stroke (Older Adults): Family/Caregiver Resilience Interventions in Community Settings25,26 and adopts the content of ‘Promoting the Family Resilience Model of the Primary Caregiver in Stroke patients’ for evidence translation. All of the team members, except the head nurse, participated in the data collection process that included direct observation, asking the caregivers, reviewing nursing documents, and checking the medical records. There are five RNs (75%) with university degrees. Eight home care nurses and 30 home caregivers for stroke patients participated in the program evaluation. The aim was to improve compliance with best practices by discussing the audit results with project team members.
Following the baseline audit, the project team analyzed the audit results to identify the gaps between current practice in the community and best practice recommendations. At this stage, the aim is to develop implementation strategies to reduce the barriers and gaps in implementing empirical nursing care programs. The team adopts a bottom-up approach, introduces the baseline audit to home nurses, collects feedback from home nurses, discusses, and discovers the obstacles that fail to meet the standard goals, and proposes strategies to improve the implementation rate. In addition, the implementation process increased the number of members to hold a face-to-face discussion meeting once a week, a total of 30 times discussion from January 2020 to September 2020, to review obstacles and possible strategies to increase the resources required for the implementation of the proposed plan for the evidence-based translation care program. These meetings are open communication and participation meetings with stakeholders to discuss and document the GRiP architecture. Based on the feedback from these meetings, team members analyze and formulate improvement plans.
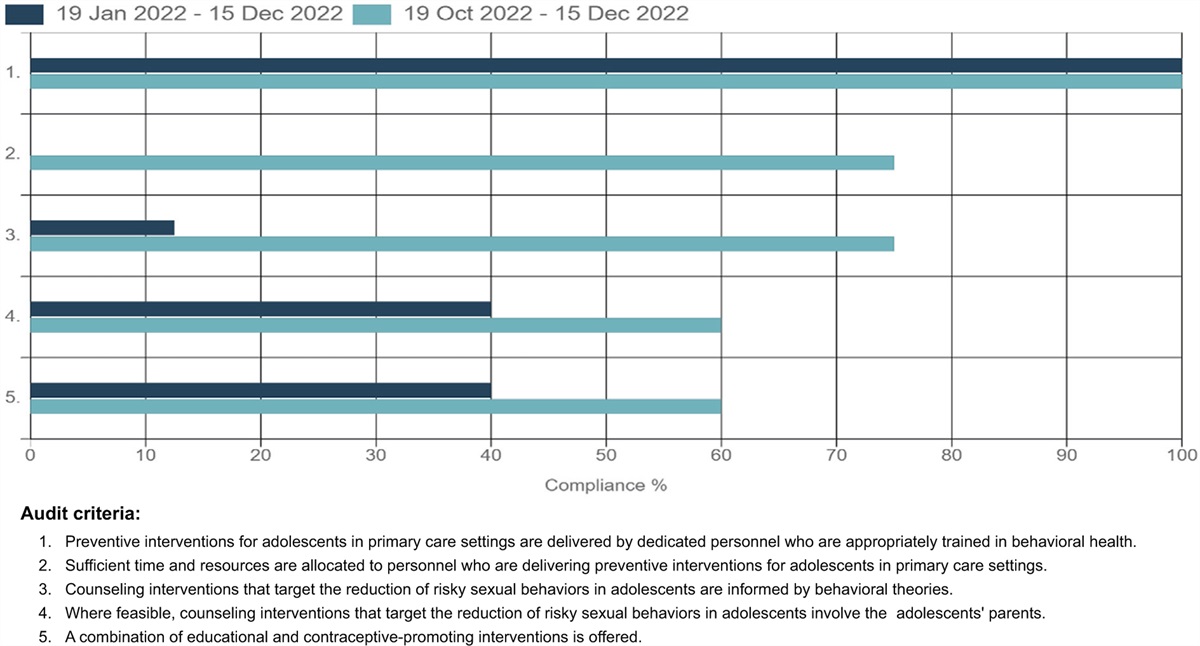
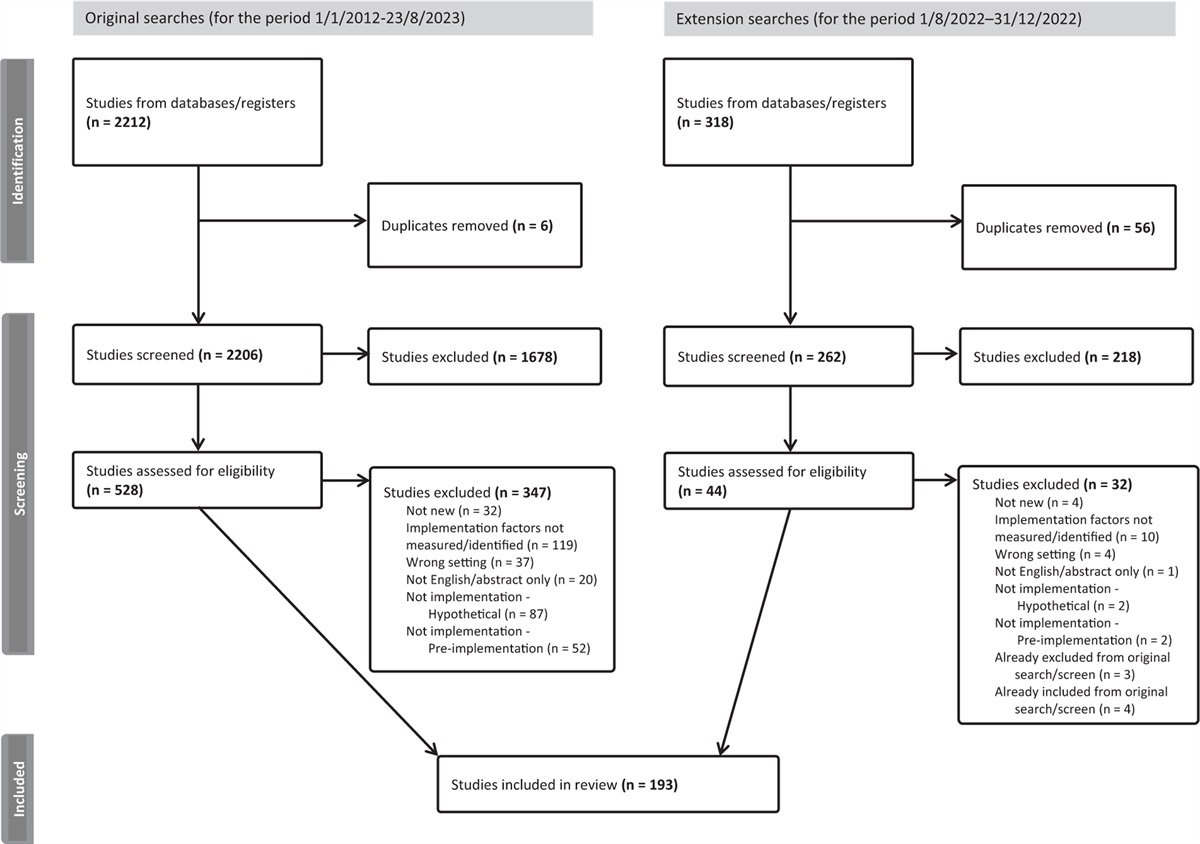
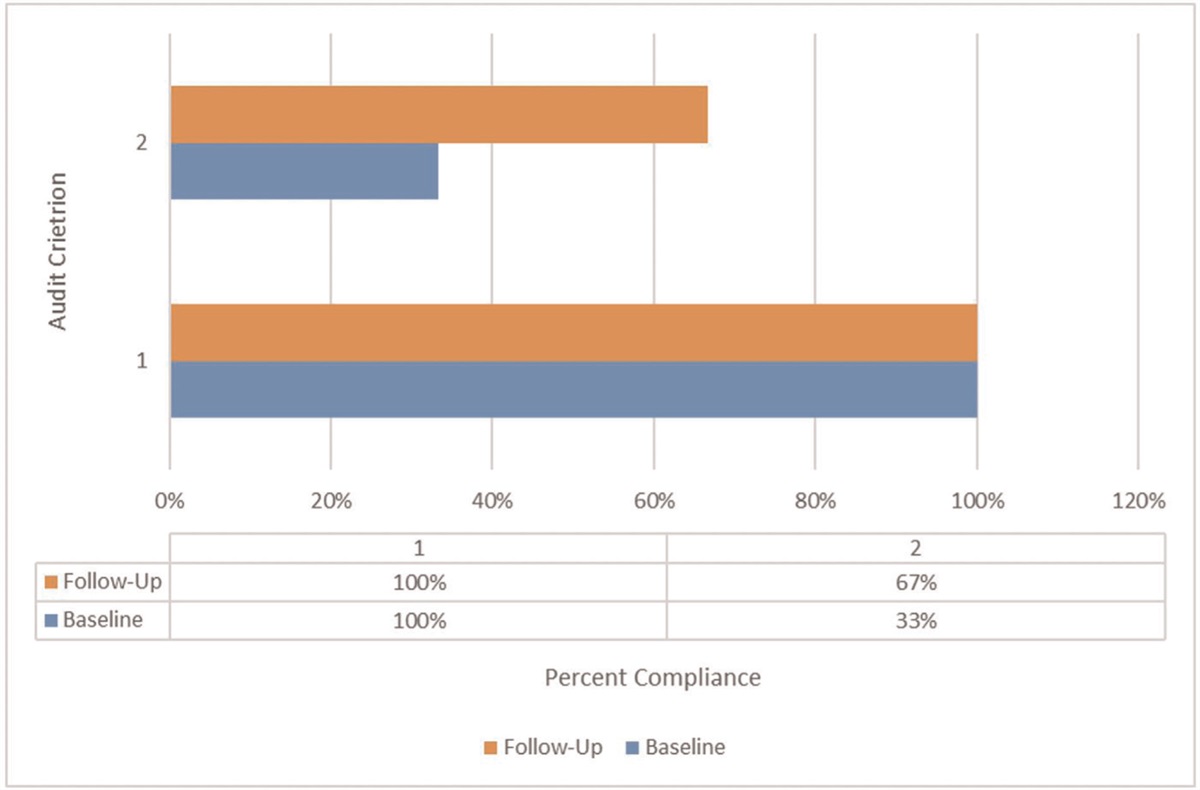
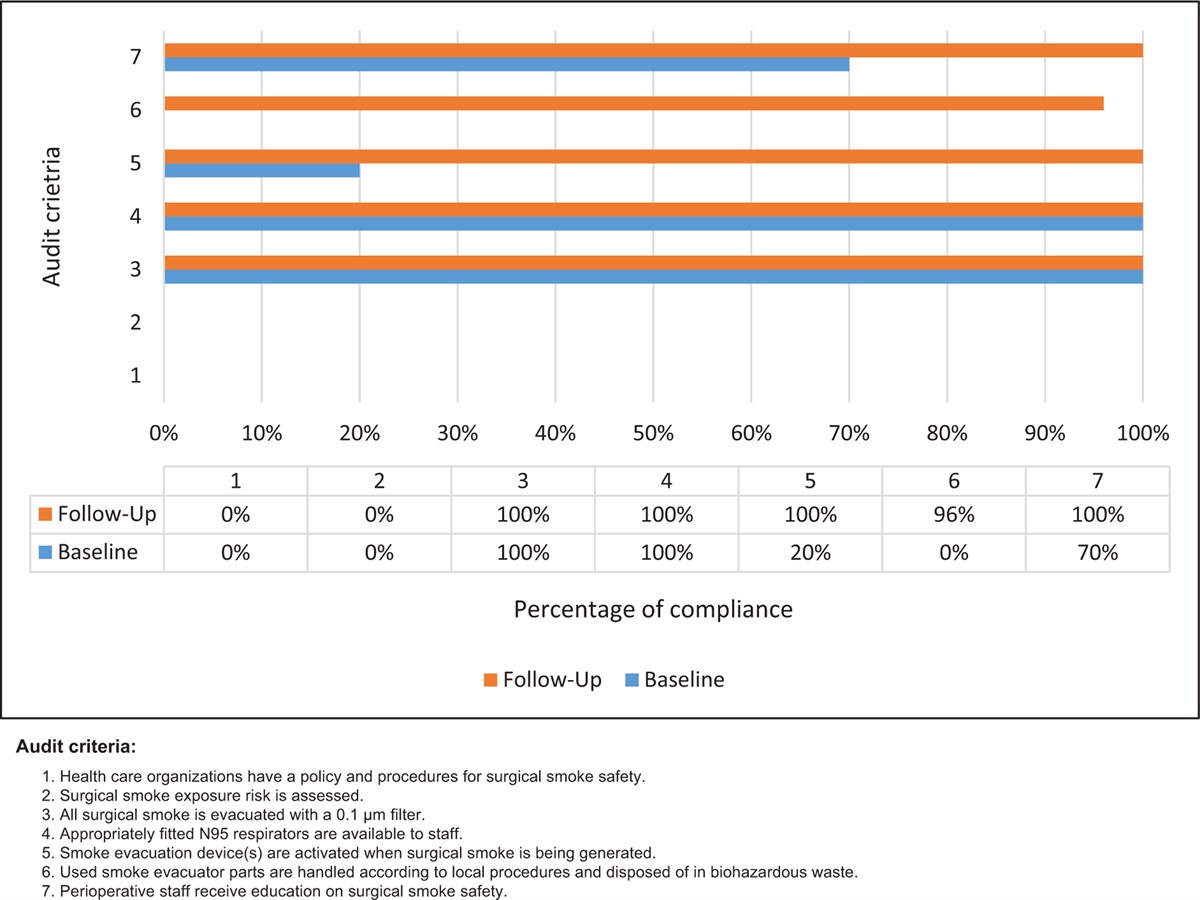
Results Phase 1: Baseline auditThe results of the baseline audit (Fig. 1) demonstrated that there were three criteria. There was 0% compliance rate with initial assessment of the staff education regarding the initial assessment of the resilience conducted using validated tool protocols (Criterion 1). A compliance rate of 0% was found for the caregivers’ education regarding community-based support programs to enhance resilience for families of an older adult with poststroke care protocols has been conducted. (Criterion 2). A total of 0% of caregivers were assessed using a validated resilience scale, for the caregivers with standard resilience care project, including using the support programs, include relative and friend support, social support, social support, family-coping coherence strategies, and education for caregivers (Criterion 3).
 Figure 1:
Figure 1: Compliance with best practice for audit criteria in follow-up audit compared with baseline audit (%) for the family caregivers of stroke patients on the resilience-based care model in the community setting.
For the implementation baseline audit, eight home care nurses and 30 caregivers of stroke patients at home were invited to participate in this project. The results of the postimplementation audit are compared with the preimplementation (baseline) audit in Fig. 1 and demonstrated that three criteria had poor compliance (0%). The validated tool conducted showed 0% compliance rate with the initial resilience assessment (e.g., BRS and 15-min assessment tool) (Criterion 1). The completion rate of home care nurses was 0%, and the achievement rate of home care nurse courses was 0%. We found a compliance rate of 0% for community-based support programs that may enhance resilience for the family caregiver of the poststroke patient (Criterion 2). Using the 8-week support programs should include relative and friend support, social support (practical, emotional, and moral), family-coping coherence strategies, and education (Criterion 3) had 0% compliance rate. We found poor compliance for the three criteria. There was only 0% compliance with staff education regarding assessment of resilience and resilience care protocols have been conducted.
Phase 2: Strategies for Getting Research into PracticeTable 2 shows the obstacles that were identified in the baseline review and the strategies for overcoming these obstacles. Seven major obstacles were identified:
Table 2 - Getting Research into Practice matrix Barrier Strategy Resources Outcomes (1) Focus on patient care and lack of resilience assessment tools for primary caregivers Based on ‘Family Resilience Model for the Primary Caregiver in Stroke Cases’, a primary caregiver assessment tool: BRS, 15-min (1 March 2019)Provide medical records of assessments (including BRS, 15 min) of primary caregivers of stroke patients at home Caregiver of stroke patient assessment guidelineLocal SOP, Audit criteria checklist (Appendix I, http://links.lww.com/IJEBH/A78) The rate of completion the checklist for medical records of assessment tools to primary caregivers of stroke patients at home (including BRS, 15 min) (2) Nurse staff lack training for providing resilience care to primary caregivers Based on ‘Family Resilience Model for the Primary Caregiver in Stroke Cases’, program, a 20 h education training program for providing resilience care to primary caregivers (including OSCE) was performed ()20-h education training methods: classroom teaching, 15-min home assessment and resilience assessment practice, OSCE) and OSCE teaching assessment () (including after passing the trial period (20 March 2019) Education team, Ministry of Health and Welfare project The percentage of home care nurses who complete the trainingThe rate of home care complete the training above 80% (3) Lack of psychoeducation intervention plans for primary caregivers Establish the contents an 8-week intervention plan for primary caregivers that includes stress management, problem solving skills, and finding care resources Staff time designing of an audit form, printing of audit forms, education team, Ministry of Health and Welfare project The rate of implementation (%) of the 8-week intervention plan related to providing psychoeducation to primary caregivers (%) (4) Lack of monitoring the implementation of the care plan for primary caregivers of stroke patients at home Establish a checklist for the 8-week resilience care plan for primary caregivers of stroke patients at home and monitoring of the implementation of the care planDiscussions regarding the implementation status of care plans for primary caregivers of stroke patients at home every Monday and discussions of new patients and the implementation progress of newly received patients during the week to monitor the implementation of care plansDiscussion of the medical records of new patients and visit new patients each week Education team, Audit criteria checklist (Appendix I, http://links.lww.com/IJEBH/A78) The rate of implementation for discussions related to each accepted patientBRS, Brief Resilience Scale; OSCE, Objective Structured Clinical Examination; SOP, standard operating procedure.
First, lack of tools for assessing the resilience of the primary caregivers; second, nurses’ lack of training for providing resilience care to primary caregivers; third, lack of psychoeducation for primary caregivers; fourth, lack of intervention plans for the psychoeducation of primary caregivers; fifth, nurses’ focus on individual patient care without providing the content of assessment records for the primary caregivers of the stroke patients at home; sixth, lack of regular discussions with the primary caregivers of stroke patients at home; and seventh, lack of monitoring of the primary caregivers’ implementation of the evidence-based nursing care plan.
Strategies adoptedFirst, home care nurses were trained to participate in the implementation of the resilience model within the evidence-based translational care program for primary caregivers of stroke patients at home, and a 20-h training in resilience care by the primary caregivers was established based on the content of the evidence-based course ‘Promoting the Family Resilience Model for the Primary Caregivers in Stroke patients’ [including Organization for Security and Co-operation in Europe (OSCE) events on 9 March, 23 March, and 30 March in 2018]. Second, the assessment tool for the primary caregivers, the BRS, was used according to the ‘Promoting the Family Resilience Model for the Primary Caregivers in Stroke patients’ course. Third, the contents of an intervention plan (weeks 1–8) for primary caregivers, including stress management, problem-solving skills and finding care resources, was established based on the ‘Promoting the Family Resilience Model for the Primary Caregivers in Stroke patients’ course. Fourth, health education content for providing resilience care to the primary caregivers, including stress management methods, problems that might be encountered, a leaflet describing problem-solving skills, the coordination of internal resources within the family, support among family members, communication with family members, methods for fostering positive thinking and care resource manuals. Fifth, the home care nurses underwent a 20-h training on resilience care education (including the OSCE) for primary caregivers based on the ‘Promoting the Family Resilience Model for the Primary Caregivers in Stroke patients’ course. The in-person training consisted of stroke case assessment, family function assessment, family function assessment exercises, assessing the needs and resilience of primary caregivers, 15-min family assessment and resilience assessment exercises, planning (care) guidance for the information needs of the primary caregivers, planning (care) guidance for the emotional needs of the primary caregivers, planning (care) guidance for the social needs of the primary caregivers, a practical discussion of special care situations and an OSCE teaching evaluation (Table 3). A policy was formulated to make the training course a requirement for home care nurses. Sixth, assessment tools for the primary caregivers of stroke patients at home, including the BRS and the 15-min assessment, were established. Seventh, a checklist of the 1–8-week resilience care plan for the primary caregivers of stroke patients at home was established and was reviewed by the head nurse to monitor the implementation of the care plan. Eighth, a weekly meeting on the implementation of the care plan by the primary caregivers of stroke patients at home was arranged to discuss new cases and the implementation progress of existing cases over the past week to monitor the implementation of the care plan. Ninth, the week's patient visits were discussed based on the medical records of new cases, and the implementation progress was tracked using the checklist. The implementation of this plan lasted 13 months, from September 2019 to September 2020.
Table 3 - Home care nurse education regarding resilience care: 20 h of primary caregiver's education training (including Objective Structured Clinical Examination) Content of the training Training hours Assessment of stroke patients 45 min Assessment of the stroke patient's family function 45 min Assessment of primary caregiver needs 45 min Assessment of primary caregiver resilience 45 min Situational practices of the functional assessment of stroke patients 1 h Assessment of the situational practices of family function 1 h Assessment of primary caregiver needs 1 h Assessment of primary caregiver resilience and practice 1 h The (nursing) guidance plan for the information needs of the primary caregiver 1 h Plans of the emotional needs for primary caregivers 1 h Plans of social participation for primary caregiver's needs 1 h The situational discussion of special care 1 h The situational exercise of the information needs plan for primary caregivers 1 h The situational exercise of the emotional needs and plan for the primary caregiver 1 h The situational exercise of the primary caregiver's social participation demands and plan 1 h Developing a video on OSCE practical instructions 1 h OSCE 3 h (1) Clinical Examination and group arrangement description (2) Comprehensive assessment of primary caregiver needs and plan Total hours 20 hOSCE, Objective Structured Clinical Examination.
The purpose of the postimplementation follow-up review is to evaluate whether improvements to the best evidence have been achieved and identify areas requiring further attention or improvement. Conduct a review of the effectiveness of the implementation strategy within 3 months. The method used in the postimplementation audit is the same as that of the pre-implementation audit. The resilience evidence translation care of family caregivers of stroke patients was implemented by eight home care therapists and 30 patients. The data were collected from September 2019 to September 2020, and the data were entered into JBI PACES, and data analysis was performed to compare the follow-up results with the audit results to check for any changes in the implementation rate of the evidence translation care implementation project. Thirteen months after implementation, we will conduct a follow-up review (a follow-up review after the implementation of the empirical translation care program) and a 12-week posttest on the concise resilience scale.
Phase 3: Follow-up and auditThe postimplementation audit on eight home care nurses and 30 home caregivers for stroke patients showed good compliance. The results of the postimplementation audit are compared with the preimplementation (baseline) audit in Fig. 1. One hundred percent of the eight home care nurses had received training for using effective and reliable tools to assess the resilience of caregivers, which was a significant improvement over the 0%. Criterion 2: Support programs should include relative and friend support, social support (practical, emotional, and moral), family-coping coherence strategies and education. Psychological education of primary caregiver: 1–8-week intervention plan content implementation rate (%), caregiver's health education evaluation checklist implementation rate (%), complete the intervention plan content according to each case, confirm the implementation rate of each case. The implementation rate of caregivers’ health education evaluation has been increased from 0 to 100%. The results of home care nurses complete the training course: the mean of the OSCE score was 98.13(+3.72). Criterion 3: Community-based support programs may be used to enhance resilience for families of an older adult with poststroke dysfunction. The effectiveness indicators of this standard are the completion rate of medical records of the evaluation tool, the implementation rate of case discussions, and the rate of completion of training by home care nurses. The OSCE test will be conducted 1 week after completing the training course, and the medical records (including BRS, 15-min family assessment) of the assessment tools for tracking the main caregivers of a stroke at home each month will increase the completion rate from 0 to 100%, and each case will be discussed. Implementation rate: The implementation rate of each accepted case discussion increased from 0 to 90%. The main reason was that the implementation rate was because three of the clinical home nurses did not follow the schedule. This study shows that the resilience model of primary caregivers of stroke patients at home through the project of implementing evidence care can effectively help the caregivers enhance their family resilience. After the home care nurses have completed their training, they will establish the resilience model of the primary caregivers of stroke patients at home. The empirical translation care plan and implementation will be implemented. From September 2019 to September 2020, the implementation of the improvement plan lasted 13 months, and a total of 30 home-based stroke caregivers were accepted. The concise resilience scale was used to evaluate the resilience of the primary caregivers before and after a single group. The results showed that the resilience of the primary caregivers of stroke patients at home increased from 17.47 points (SD + 1.94) in the pretest to 18.33 points in the posttest score (SD + 1.54), and the test results before and after the resilience scale reached a significant difference (P value <0.001).
DiscussionThis study was conducted in a home care service in Taiwan. The findings of this project showed improvement in several criteria: home care nurses were lacking knowledge about the resilience care, the compliance of resilience assessment. The findings of this project showed improvement in the three criteria: nurses who received education about resilience care protocols increased from 0 to 100%. The percentage of home care nurses who complete the training from increased 0 to 100%. The rate of implementation (%) of the 8-week intervention plan related to providing psychoeducation to primary caregivers (%) increased from 0 to 100%. The rate of implementation for discussions related for primary caregivers of stroke patients at home increased from 0 to 90%.
Furthermore, in the community, there was a lack of evidence-based support programs for the caregivers of stroke patients. Following the implementation of strategies reported in the GRiP phase, the compliance with all three criteria were significantly improved by the study. Among them, the criteria ‘education and training on nurses’, and ‘used reliable and valid instrument to assess resilience in caregivers’ all reached 100% compliance, while ‘using community-based support programs to enhance resilience’ reached 90% compliance, and finally, over the whole project results showed that the average resilience of caregivers increased from 17.47 (SD ± 1.94) to 18.33 (SD ± 1.54). The resilience scale of pretest and posttest scores were significantly different (P value ≤0.001). The inadequacy of family caregivers’ knowledge and skill may decrease their support for the patient and consequently affect their quality of life. The caregiver support program is an intervention to improve chronic disease patients’ adaptability and quality of life by empowering the family caregiver.21,22 According to Sadler,33 establishing evidence-based support intervention to promote resilience after stroke was effective for enhancing caregivers’ resilience. Building a multidisciplinary group to implement a new protocol and appointing a team leader to monitor the outcomes are important strategies, as we discovered throughout our project. We successfully used evidence-based knowledge to promote the family caregivers of stroke patients. Clinical guidelines indicate that using caregiver resilience assessment protocols and the support programs for caregiver resilience interventions in community settings attempt to improve the resilience of the caregiver of patients in the community.38 Three factors contributed to the success of this project, which included leadership, clinical situation education, and situation monitoring. The project's leaders included the nursing deputy director and head nurses related to the first success factor.
Success factors in the implementationDuring the baseline audit, it was found that the nurses had not received enough educational training regarding the resilience assessment and resilience model for caregivers of stroke patients in community. In view of this, education courses were provided in accordance with JBI empirical guidelines; the aims were to strengthen the professional resilience assessment and education of, to implement correctly nursing assessment, and to improve the guidance provided by nurses to provide the resilience support program of caregivers. The integrated teaching model was used to design a 20 h training program. Each team of the nurse started with a ‘15-min family functional assessment’ and arranged the 10 h practice of the actual operation. The OSCE classroom situation was used for the operation to allow nurses to effectively implement resilience care model assessment skills, effectively increasing the resilience care strategy, and enhance their sense of responsibility and motivation; the overall aim was to promote better resilience care of the caregivers.
We utilized the following three essential factors to improve resilience adequacy compliance during this project.
LeadershipThe current project uses the transformational leadership strategies26,27 to build consensus and develop the commitment of the nurses to promote evidence-based resilience care of family caregiver implementation. Transformational leadership motivates followers by appealing to higher ideas and moral values. This leads to followers acting to sustain the greater good, and supportive environments where responsibility is shared.28,29 This was done via the leadership of the deputy director and head nurse of our team members. The deputy director and head nurse explained the care burden of the family caregiver clinical problems and situation analysis, then presented how to maintain the home care nurses’ roles and tasks, made the point of resilience care recommendation, cared for the individual nurses, discussed with home care nurse individually, and taught, counseled, guided, and motivated the staff to move toward their goals. Furthermore, the empirical improvement strategies not only enhanced resilience care professional knowledge, but also promoted caregivers’ care by establishing a partnership relationship with patients and caregivers. Caregivers may affect the long-term prognosis of patients after stroke.28 They need a well-planned preparation, a tender loving home care team, and strong support by a network of resources from the community. Such a comprehensive care carries out the idea of whole person, whole family, and whole community, so that family's emotional distress can be reduced. This was also helpful because it improved the quality of patients’ and caregivers’ care, created a more friendly workplace, and brought about a reliable relationship between nurses and patients’ whole family. Furthermore, our organization was able to adapt evidence-based ideas into policy reforms using standard operating procedures.
Clinical situation educationBased on the updated theoretical and evidence-based knowledge and practice skills identified as part of this study, the deputy director and head nurse and JBI team members developed teaching and learning strategies that included clinical situation learning and OSCE; these were able to enhance the nurses’ knowledge and provide motivation for enhanced their knowledge, skills, and attitude when caring for caregivers while at the same time achieving improved resilience care.
Situation monitoringThe deputy director and head nurse and team members developed an assessment and monitoring plan that measured the accuracy of the nurses’ resilience assessments of caregivers and created individualized nursing care plans for the family caregivers in community.
ChallengesThere were some challenges encountered with this project. The first challenge was that it was the project team member's responsibility to check whether the caregiver could perform resilience care by themselves correctly, but team members also had their own daily workload or they might not have been on duty. Therefore, to overcome this barrier we trained two audit members on each caregiver of stroke patients to ensure that audits could be completed. Build trust in the language of individual cases, clarify case problems, and needs, provide timely emotional support, communicate and solve problems. Therefore, the implementation project should establish personalized family caregiver clinical problems and situation analysis.28,29,34 Through the implementation of these two strategies, the project explained the care burden of the family, caregiver clinical problems and situation analysis, then presented how to maintain the home care nurses’ roles and tasks, made the point of resilience care recommendation, cared for the individual nurses, and discussed with home care nurses individually.
The current project was only implemented in a home care service. In the future, this best practice implementation project should be more widely used for all caregivers of stroke patients, when they are undergoing a primary caregiver, and keep an ongoing resilience care audit. Following the implementation of measures to increase clinical professional knowledge and enhance nurses’ ability to follow practice guidelines, the implementation rate of the eight nurses (100%) who were provided with information on the caregivers of stroke patients on resilience care protocols was increased. The implementation rate of the health education checklist for caregivers increased by 30 (100%). The thirty caregivers (90%) were fully participated into the implementation of support programs, including relative and friend support, social support, and family-coping coherence strategies, as well as providing the above related enhancing resilience education for caregivers.
留言 (0)