Recent advances in in vitro and in vivo studies have highlighted the diverse antimicrobial properties of HMOs. They serve as metabolic substrates for gut microbiota, improve gut barrier functions, act as decoy receptors in preventing pathogen adhesion on the mucosal membrane, regulate immune responses, and thereby reduce the rate of infections.
4.1. HMOs Shape Gut Flora and Gut Immune FunctionThe human gut is a vital organ needed for maintaining all the functions of the human body. Colonization of the gut by microbes plays a critical role in host metabolism, mostly established in a child’s life during 2–3 years of age. The human gut also helps in maintaining the immune, gastrointestinal, and neural systems [
61]. In the gut, intestinal epithelial cells absorb acidic HMOs by the nonspecific paracellular route and neutral HMOs by the receptor-mediated transcellular pathway [
37,
62]. Studies have shown that HMOs modulate protein expression of gut epithelial cells. In an in vivo study, supplementation of sialylated HMOs in rats reduced the expression of genes responsible for the secretion of IL-12, L-8, NF-kB, and TNFα by activating the anti-inflammatory peptidoglycan recognition protein 3 (PglyRP3) [
63,
64]. It is also well established that HMOs, specifically 2′FL, inhibit the secretion of proinflammatory cytokines in HT-29 and Hep-2 cell lines that significantly reduce the invasion of C. jejuni [
65].Furthermore, HMOs strengthen the intestinal barrier by modulating the synthesis of mucin [
66]. It was observed that HMO supplementation restores goblet cells in rats with necrotizing enterocolitis. Goblet cells synthesize Muc2 and other factors that form the protective mucous layer over the intestinal epithelial cells [
67]. It was also demonstrated that 2′FL and LNnT induce the expression of claudin-5 and claudin-8 proteins, which are significant in strengthening the tight junctions and limiting the permeability of molecules through the intestinal walls [
68,
69].HMO molecules enrich the gut microbiome, specifically by promoting the colonization by a Bifidobacterium-dominated bacterial community [
70]. Among Bifidobacteria, a distinct class of gene cluster encoding fucosidase and sialidases enzymes and their specific transporters is required for breaking down the complex HMOs [
51].In Bifidobacteria, HMO molecules are degraded by either intracellular or extracellular strategies [
71]. Intracellular digestion includes the transportation of HMOs inside the cell via ABC transporters and enzymatic hydrolysis of the HMO molecule into monosaccharides by glycosyl hydrolases [
72]. In the extracellular process, the HMOs are degraded into their monomers outside the cell by cell-surface-associated glycosidases and the monosaccharides are transported inside the cell. The digested HMOs are then assimilated into the bacterial central metabolism pathway, which releases short chain fatty acids (SCFA) as end products [
33,
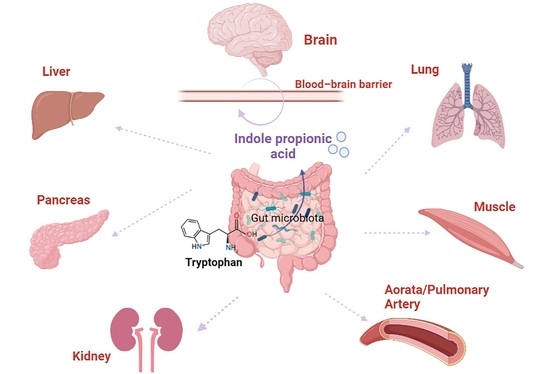
73]. SCFA serves as an intermediate molecule in connecting gut flora with the immune system. They modify gene expression, differentiation, and apoptosis of epithelial cells; inhibit the function of histone deacetylases; and activate G-protein coupled receptors (GPCRs). GPCRs, along with other transcriptional factors, modulate the function and development of leukocytes. All the SCFAs also possess other specific functions. For instance, acetic acid and butyric acid act as a source of energy for muscle and skeletal tissue and colonocytes, respectively. Butyric acid also improves the gut epithelial barrier, regulates the proliferation and activity of regulatory T cells, and enhances the metabolism of intestinal epithelial cells [
74,
75]. The SCFAs are crucial for appetite as they activate free fatty acid receptors that, in turn, elevate the circulation of intestinal anorectic hormones [
76]. Additionally, they exhibit antimicrobial properties against viral, bacterial, and protozoal infections. The SCFAs, along with sphingomyelin, promote the myelination of the central nervous system [
53]. Moreover, the synthesis of SCFAs reduces the pH of the colon, which is non-conducive for the survival of pathogenic bacteria [
77]. The HMOs also promote the growth of other commensal bacteria such as Akkermansia and Lactobacillus. Akkermansia increases the secretion of mucin which reduces the colonization of harmful bacteria [
78]. In 2022, an in vivo study by Kathryn and group demonstrated the protective activity of pooled HMOs against Group B Streptococcus (GBS) colonization in the vagina without altering the vaginal flora [
79].Finally, the metabolism of HMOs and the end products are selective among different bacterial strains. It is dependent on the specific gene clusters present in bacteria and the molecular structure of HMO molecules. For instance, B. breve and B. longum actively degrade LNT, whereas digestion of fucosylated HMOs is more conducive for B. bifidium and B. infantis [
80,
81]. 4.2. HMOs Prevent the Growth and Colonization of Pathogenic Bacteria
As discussed above, HMOs serve as a selective substrate and specifically favor the growth of symbiotic bacteria. As a result, the gut flora outcompetes the pathogenic bacteria for space and nutrients. Additionally, the end products of HMO metabolism, such as SCFAs, lower the intestinal pH that stunts the growth and proliferation of harmful bacteria.
Furthermore, HMO molecules act as anti-adhesive molecules and prevent the colonization of pathogenic bacteria.
The first step of bacterial colonization involves the adhesion of bacteria to the host cell surface, which is mediated by the binding of bacterial surface ligands to the host cell oligosaccharide receptors. HMOs behave as decoys and bind efficiently to the pathogen adhesins due to their smaller size [
82,
83]. Thus, HMOs act as receptor analogs that bind to pathogens and prevent their colonization, thereby reducing the incidence of infectious diseases (
Figure 5) [
25]. Another mode of eradicating pathogens adopted by the HMOs is due to their ability to compete with the pathogens for binding to the cell surface receptors. HMOs prevent pathogens from adhering to the cell surface carbohydrate receptors by behaving as carbohydrate-binding ligands or soluble ligand analogs which compete with bacterial adhesins to bind to these receptors and thus competitively inhibit their attachment, further preventing their colonization (
Figure 6) [
25].The anti-adherence properties of HMOs are reported against Shigella sp., Campylobacter sp., and various pathotypes of E. coli [
84,
85]. The HMOs also prevent the attachment of L. monocytogenes and S. pneumoniae to the host cell surface [
53,
86]. Several in vivo and in vitro studies have displayed compromised GBS colonization in the vagina without affecting the pre-existing vaginal microbiome. This can evolve as a promising preventive therapy against vaginosis [
79]. Studies revealed that the acidic fraction of HMOs effectively alters the expression of genes responsible for the arrangement of surface receptors, which affects pathogen binding. This type of interaction was observed in the presence of 3′-SL against enteropathogenic E. coli [
87]. The anti-adhesive properties of HMOs are influenced by the charge and molecular weight of the oligosaccharide and the targeted pathogen [
35].In the neutral HMOs, fucosylated fractions have been reported to exhibit intermediate levels of adhesion inhibition (up to 50%). Neutral HMOs exhibit antipathogenic functionalities depending on their molecular weight and pathogenic species. The high molecular weight fragments (HMWF) are known to inhibit adhesion in E. coli and Vibrio cholerae, and low molecular weight fragments (LMWF) inhibit the adhesion of E. coli and Salmonella fyris. However, HMWF failed to inhibit S. fyris and LMWF failed to inhibit V. cholerae, indicating their pathogen specificity [
88]. Pathogen-inhibiting activity also depends upon the fucosylation patterns. Research demonstrated that 2′-FL has shown inhibitory activity against several pathogen species. Studies using 2′-FL against C. jejuni have reported the inhibition of the pathogen to human intestinal epithelial cells [
65,
89]. In other work, 2′-FL has also shown anti-adhesive effects against enteropathogenic E. coli (EPEC) and V. cholerae to intestinal epithelial cells (Caco-2). Additionally, 2′-FL also retards Pseudomonas spp. infection [
56]. The anti-adhesive activity of 2′-FL was also observed against Neisseria meningitides, whose adhesion to salivary agglutinin was effectively inhibited. Recent studies involving the use of 2′-FL against S. agalactiae, and its serotypes have shown an adhesion inhibitory effect [
89]. It has been found that 2′-FL competes with pathogens to bind to the cell surface glycan receptors, which prevents colonization and invasion of the pathogens. The unbound pathogen is then eliminated without causing any infections [
89]. Like 2′-FL, 3-FL also exhibits anti-adhesive effects; 3-FL inhibited the adhesion of E. coli by 30% and S. fyris by 16%. It also reduced the binding of P. aeruginosa to the human respiratory cell line A549 by up to 23% [
90]. Neutral N-containing HMOs such as LNnT are also efficient in inhibiting the adhesion of S. pneumoniae [
88]. Furthermore, acidic HMOs also contribute towards the inhibition of pathogen adhesion. One study showed that 3′-SL, in particular, has inhibited cellular adhesion in E. coli serotype O119, H. pylori, and V. cholerae [
88], and 3′-SL is also known to reduce the invasion of uropathogenic E. coli (UPEC) [
91]. Similarly, 6′-SL has shown anti-adhesive effects against S. pneumoniae. It also inhibited the adhesion of Salmonella fyris to buccal epithelial cells [
88]. Studies showed that the presence of acidic HMOs inhibited the expression of several fimbrial types in E. coli. Unlike neutral HMO fractions, sialylated oligosaccharides have reduced pathogen specificity. This is because sialylated oligosaccharides, being negatively charged, readily commute with the oppositely charged segments present on the cell surface [
34]. Furthermore, HMOs are reported to avert necrotizing enterocolitis (NEC). NEC etiology can attribute to the extensive establishment of bacterial and mucosal neutrophil infiltration. In vivo studies revealed that the introduction of HMOs resulted in the elevated expression of muc2, resulting in the release of mucin proteins, which makes enterocytes impermeable to dextran, thereby inhibiting microbial adhesion, reducing the activation of neutrophils, and thus lowering mucosal neutrophil activity [
76,
92]. In addition, HMOs containing galactose and mannose monosaccharide moieties were observed to prevent adhesion in many bacterial species, which include C. jejuni, Citrobacter rodentium, Cronobacter sakazakii, EPEC, Enterobacter cloacae, Salmonella pullorum, and. S. typhimurium, and have shown both anti-adhesive and anti-invasive effects in the presence of GOS [
93,
94,
95]. Studies using FOS, which contains fructose monosaccharide in its structure, against E. coli resulted in the inhibition of adhesion to human intestinal epithelial cells [
96,
97].
Apart from the anti-adhesive properties of HMOs, several studies have demonstrated the antibacterial activities of HMOs against different pathogenic bacteria.
A large portion of protein in milk that imparts a significant barrier to pathogen invasion in the gut is N-glycans. The milk oligosaccharides attached to the protein called N-linked glycans are more active than the free oligosaccharides. Yue et al. (2020) reported the MIC values for N-linked and free milk oligosaccharides against S. aureus as 256 nmol/mL and 32,768 nmol/mL, respectively. This implies that N-glycans are more active than free milk oligosaccharides [
98]. The antibacterial activity of N-glycans is comparable with commercially available antibiotics, such as kanamycin. The growth inhibition of S. aureus and S. typhimurium by N-glycans exceeded the activity of kanamycin, whereas a moderate inhibition was observed against E. coli and L. monocytogenes [
99]. Another study, however, showed a notable decline in the growth of E. coli, Peptostreptococcaceae, and C. jejuni in the presence of LNnT. Interestingly, LNnT also exhibits stronger antibacterial activity against GBS, S. agalactiae strain GB590, and S. agalactiae strain GB2 [
100]. The fucose moiety of N-glycans is responsible for the antipathogenic effect as defucosylation of N-glycans resulted in lowered or negligible inhibition for all the pathogens [
101]. Furthermore, the growth inhibitory effect of neutral HMOs is also reported against S. agalactiae (GBS) and its different serotypes. Growth reduction above ~95% was observed in GBS serotype III, Ia, and V [
91]. One of the studies demonstrated that neutral HMOs from different donors decreased S. agalactiae GB590 growth by 80% and S. agalactiae GB2 growth by 95%. The same study also showed a reduction in S. agalactiae strain GB2 viability by 36% [
98]. In particular, 2′-FL reduced the growth of S. agalactiae strain GB590 by 20% within 4 h and 11% after 24 h [
89]. In another study, 2′-FL successfully prevented the invasion of Campylobacter jejuni, E. coli, and Peptostreptococcaceae, thus retarding their growth and colonization [
35]. Growth of Deferribacteres, Anaerotruncus, Parabacteroides, Eubacterium, Mucispirillum, Patescibacteria, and Alistipes was sharply suppressed in the presence of 2′-FL [
57]. Acidic HMOs such as 6′-SL effectively inhibit P. aeruginosa, a crucial opportunistic pathogen that leads to detrimental infections, such as infection of human pneumocytes in cystic fibrosis. HMOs enter the systemic circulation from the gut and then reach the respiratory system where they modulate the pathogen–host interaction by binding to the pathogen and not to the respiratory cells [
101]. 4.3. Antibiofilm Activity of HMOsConsidering the immense benefits of HMOs and their diverse antibacterial properties, researchers have evaluated the antibiofilm potential of HMO molecules. The presence of HMOs has shown inhibitory effects against biofilm assembly. Up to 93% biofilm inhibition by HMOs was observed against the S. agalactiae strain and up to 60% inhibition was observed against methicillin-resistant S. aureus (MRSA) [
102]. A recent study demonstrated that GB2 had pronounced vulnerability towards HMOs [
103]. The same study also showed that HMOs decreased biofilm production in S. aureus by 30–60% [
104]. An in vitro study showed that the presence of HMOs caused a significant decline in the formation of biofilms in multi- and pan-drug-resistant A. baumanii. HMOs mainly act by suppressing the formation of pellicles (floating biofilms). The same study also revealed that HMOs potently inhibited biofilm establishment but were not effective in distorting pre-existing biofilms [
105]. The biofilm matrix aids the dilution of antibiotic molecules either by lowering their diffusion into the biofilm or by other machinery. This calls for novel techniques that disrupt these mechanisms and facilitate the action of antibiotics. HMOs are shown to potentiate the action of several antibiotics such as clindamycin, erythromycin, gentamicin, and minocycline against GBS [
106]. HMOs with varying monosaccharide constituents have shown a greater capability in inhibiting biofilm formation. Neutral HMOs, specifically 2’-FL, lack efficient antibiofilm activity. However, the conversion of 2′-FL to an anionic, amino derivative illustrated significant results [
107]. The alteration of 2′-FL by amination (Kochetkov amination) forming the cationic molecule 1-amino-2′-fucosyllactose showed biofilm inhibitory activity. The mechanism of biofilm inhibition was not clearly understood but it was hypothesized that the inhibitory action was due to the interactions between the cationic fucosyllactose entity with the anionic EPS matrix and the negatively charged DNA structure, which led to the inclusion of a positive charge in the biofilm structure. The introduction of cationic charges in the biofilm structure thus dismantled the biofilm. Therefore, the use of 2′-FL derivatives executed biofilm inhibitory activity against S. agalactiae GB2 and GB590 and reduced the biofilm production by 46% in GB2 and 37% in GB590 [
108]. The antibacterial and antibiofilm activities of different HMOs are listed in
Table 2. In a recent study by Sylwia Jarzynka et al., the antibiofilm activity of total and fractionated HMO molecules were evaluated against mature biofilms of different clinically relevant Gram-negative and Gram-positive bacteria. They observed isolate and strain-specific reductions in the number of biofilm cells among Gram-positive bacteria, specifically in E. faecalis and S. aureus. However, HMOs did not show any significant activity against pre-formed biofilms of Gram-negative bacteria [
109].Summarizing all the results, we can conclude that HMO molecules can modulate the initial stages of biofilm formation and prevent bacterial colonization. However, the underlying molecular mechanism is not yet well understood. Researchers hypothesize that the antibiofilm activity of HMOs may be due to their structural resemblance with the bacterial polysaccharides, that in turn modulate the gene expression profile of bacterial EPS, needed to maintain a structured biofilm community [
104,
113,
114]. Focused in vivo studies in this context are, therefore, necessary to prove this hypothesis.




留言 (0)