
記住我

CD19-directed chimeric antigen receptor (CAR) T cell therapy has given rise to a long-term efficacy for relapsed or refractory B cell lymphoma and even a potential cure for patients who have attained complete response (CR) (1–4). Zuma-1 showed that the 5-year overall survival (OS) of Axi-cel for large B-cell lymphoma (LBCL) was 42.6% with more than 5 years of follow-up (5). Moreover, Zuma-5 and other clinical trials showed higher rates of durable responses of CD19-directed CAR T cells for indolent non-Hodgkin lymphomas, such as follicular lymphoma and marginal zone lymphoma (6).
Three approved products of CD19-directed CAR T cells are all manufactured by viral gene transfer (7); however, there have been emerging preclinical and clinical trials using non-viral gene transfer-prepared CAR T cells in the treatment of lymphomas or solid tumors. The advantages of the latter method include lower production cost, well-tolerated toxicities, and higher composition of stem cell memory T cells in the products (8, 9). Transposons, as natural non-viral gene delivery vectors, have three types including Sleeping Beauty (SB), Piggy Bac (pb), and Tol2. The pb system is constituted by the pb transposase and a separate transfer plasmid carrying the desired genetic cargo (CAR construct, for instance). It has a higher transposition activity than SB and a larger cargo size than viral vectors; however, the electroporation process for the delivery of transposon vectors might be toxic to the cells, and the transfection efficiency lower than viral vectors (9). In a preclinical trial, mesothelin-targeting CAR T cells, prepared by pb, exhibited a rapid and robust killing effect against pancreatic cancer cells; in the xenograft mice model, they significantly suppressed tumor growth, causing minimal lesions in major organs (10). In a phase I trial treating nine patients with advanced non-small cell lung cancer using EGFR-specific CAR T cells generated by pb, Zhang et al. only reported grades 1 to 3 fever as observed after CAR T cell infusion, without any other symptoms of serious cytokine release syndrome (CRS) (11).
In the Zuma-1 clinical trial, the reported CRS was 92%, in which grade 3 or worse was 11%, and the ICANS was 67%, with grade 3 or worse being 32% (12). Patients with effusions usually had a higher rate of severe CRS and non-relapse mortality rate (13) and were not eligible for Zuma-1 trial (12). Based on our studies of CAR T cells with Piggy Bac in mesothelin and EGFR (10, 11), we generated an anti-CD19 pbCAR T. After evaluation of CD19 CAR T in terms of antitumor activity and safety, we initiated a clinical POC study that was approved by the Board of Ethics of the Shanghai Mengchao Cancer Hospital. We report here a case of relapsed follicular lymphoma with a high tumor burden, including bulky lymphadenopathies and a large amount of chylous ascites, which did not respond to chemotherapy; an anti-CD19 pbCAR T cell therapy was given. The patient rapidly reached nearly complete metabolic remission (CMR) on day 28 positron emission tomography–computed tomography (PET-CT) evaluation. Only grade 1 CRS occurred, and no neurotoxicity was observed.
Case presentationMedical historyA female patient in her mid-40s was initially diagnosed with follicular lymphoma by laparoscopic biopsy in 2015. At her diagnosis, she had multiple retroperitoneal lymphadenopathies, pleural effusion, and ascites. She was given chemotherapy for a total of 12 cycles and achieved remission. She felt well until October 2021, when she palpated an abdominal soft tissue mass on the right lower quadrant. The enhanced CT scan displayed multiple masses in the liver and retroperitoneal lymphadenopathies in the abdominal–pelvic cavity. A laparoscopic biopsy again confirmed a pathological diagnosis with relapsed follicular lymphoma (grade 1, 60%; grade 2, 40%). She received “R-COPP” regimen at a local hospital; however, her ascites progressed. The PET-CT scan showed multiple loci infiltration, including groups of deep and superficial lymphadenopathies, in the liver, bilateral lungs, abdominal–pelvic omentum, and mesentery, right adnexa with 5-cm mass, multiple loci of bone lesions, and a large amount of ascites with medium volume of left pleural effusion. She received two cycles of “R-Gemox” chemotherapy without any response. A pretreatment evaluation confirmed the patient’s high tumor burden with stage IV disease and a follicular lymphoma international prognostic index (FLIPI) score of three points.
The patient met the inclusion criteria, including relapsed follicular lymphoma, no response after two lines of chemotherapy, multiple loci of infiltration, and positive immunohistochemical staining of CD19. She signed the informed consent to be enrolled in the CD19-directed CAR T cell clinical trial.
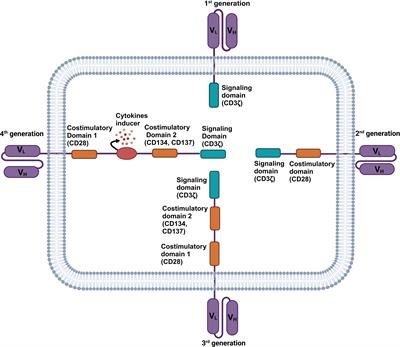
Preparation of CD19-directed pbCAR T cellsTo manufacture CD19-directed CAR T cells, the patient underwent leukapheresis to collect peripheral blood mononuclear cells (PBMCS). CAR-T cell electroporation, activation, and expansion were performed in the laboratory of the Cell Drug Unit, Shanghai Cell Therapy Group Corporation, as described previously (14). Briefly, autologous PBMCS were electroporated with Piggy Bac transposon and transposase plasmids encoding CD19-directed CAR with a 4-1BB costimulatory and a CD3ζ signaling domain.
Clinical resultsResponse to CD19-directed pbCAR T therapyThis study was an investigator-initiated trial sponsored by Shanghai Cell Therapy Group Corporation and approved by the Institutional Review Board of Shanghai Mengchao Cancer Hospital. The patient received a lymphodepleting regimen, cyclophosphamide—400 mg (300mg/m2) and fludarabine—40 mg (30mg/m2), daily on days -5 to -3. Two days later, the patient received a dose of 6 × 106/kg CD19-directed pbCAR T cells infused intravenously.
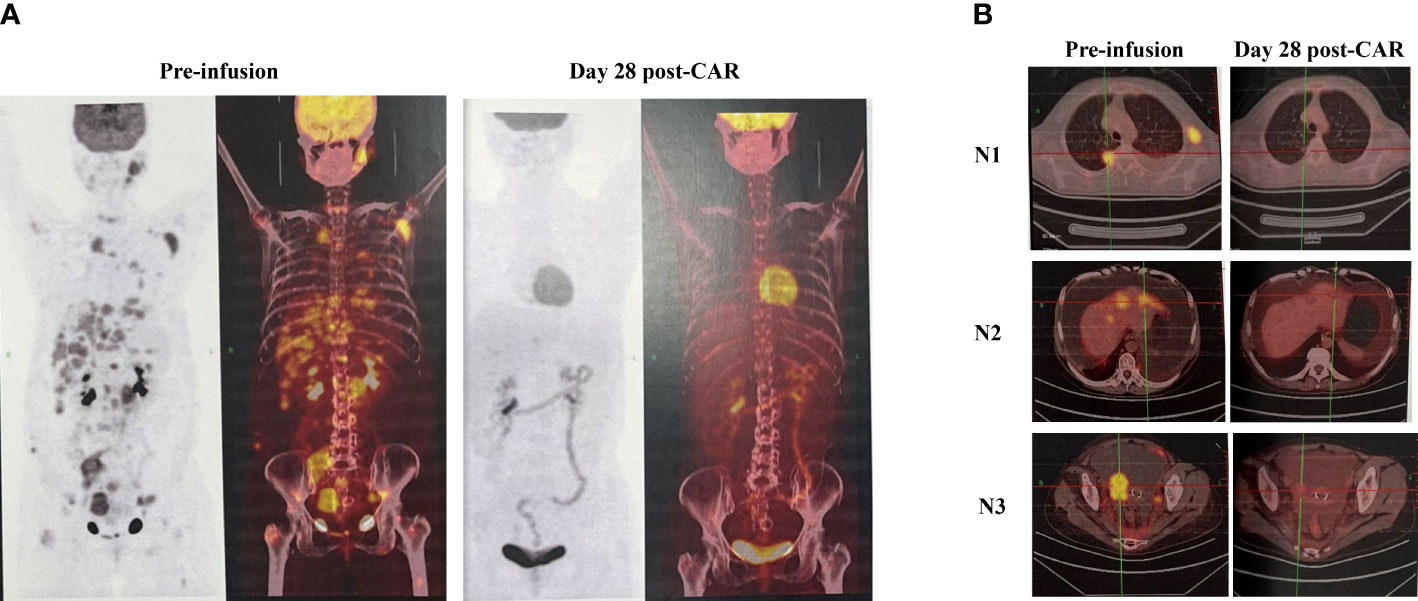
She had a rapid shrinkage of her left cervical, axillary lymph nodes, and soft tissue mass located on the right lower quadrant of the abdomen. Her left cervical lymph nodes (30 × 18 mm before infusion) were unpalpated within 1 week and undetected on day 14 by ultrasonography. She had a repeated low-grade fever in the first week after infusion, with the highest temperature of 38.2°C on day 1. She also complained of pain in the waist and bilateral inguinal regions, which was tolerable. She had grade 1 CRS, and there was no evidence of neurotoxicity. On day 28, the PET-CT image showed nearly CMR with a few loci in the liver left with a standard uptake value (SUVmax) of 4.12. However, the adnexa infiltration still existed, and the size decreased from 5 to 2.6 cm, with an SUV of 2.90, similar to that of the liver blood pool (SUVmax = 2.65) (Figures 1A, B). At her 3-month re-evaluation by PET-CT, the sizes of the adnexa mass and the liver lesions further decreased, with no uptake of adnexa mass and with one liver lesion left with a little higher SUV. The chylous ascites also gradually decreased, and the drainage catheter was removed on day 43. As of July 24, 2022, the patient was still at follow-up. The main clinical events are outlined in Table 1.
Figure 1 Clinical evaluation by PET-CT imaging. (A) Compared with the image before CAR T, PET-CT evaluation on day 28 showed nearly CMR with a few loci in the liver left. (B) The lymphoma activities were inhibited after CAR T cell infusion, as seen by PET-CT images for nodules at the lung, liver, and right adnexa. CMR, complete metabolic remission; N, nodule.
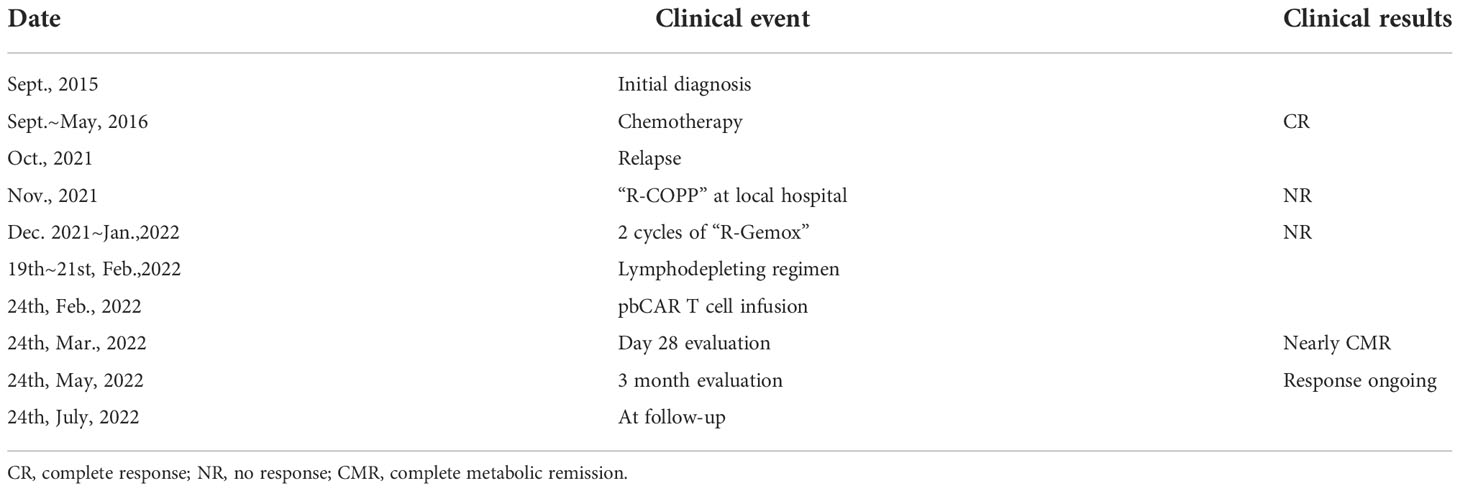
Table 1 The whole treatment process of the case with relapsed follicular lymphoma.
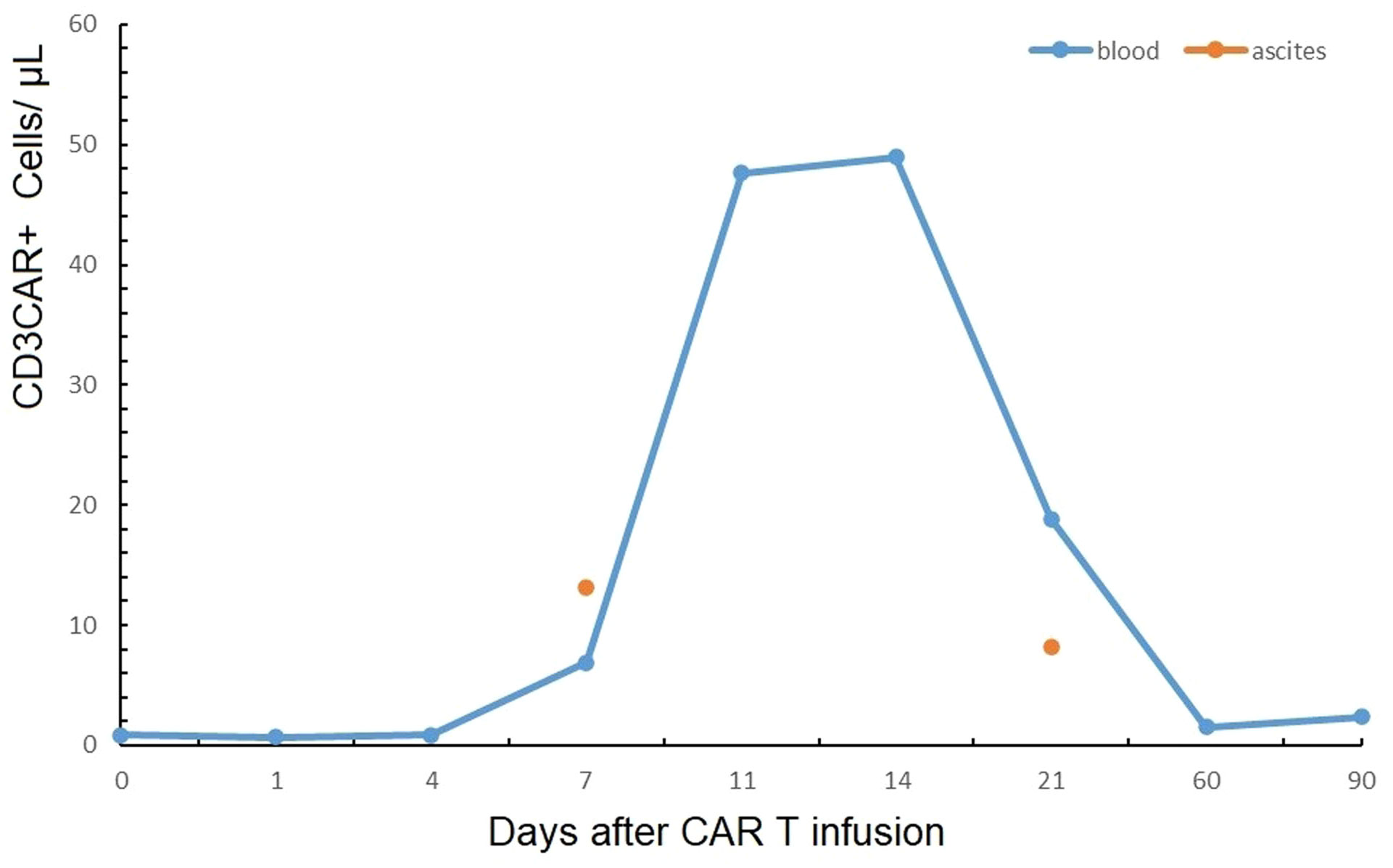
PharmacokineticsCD19-directed CAR T cells were detected both in the blood and the chylous ascites by flow cytometry. Circulating CAR T cells were first detected on day 7, and the absolute value was 6.86 μl-1. They peaked on day 14, with an absolute value of 48.97 μl-1, which accounted for 14.73% of all lymphocytes. Then, the value reduced to 18.85 μl-1 on day 21 but maintained detected as 2.38 μl-1 at 3 months. The CAR T cells could be detected in the ascites on day 7, with an absolute value of 13.15 μl-1, which was higher than that in the blood on the same day. On day 21, the CAR T cells were still detected in the ascites, with a value of 8.13 μl-1 (Figure 2). The expanded CAR T cells consisted of a certain percentage of immunotypic memory cells, with the CD3+CD45RA-CCR7+CAR+cells of 46.68 μl-1 on day 11, accounting for most of the CAR+ cells, and decreased to 2.88 μl-1 on day 21; however, these were still detected at 3 months (Supplementary Figure S1).
Figure 2 Circulating CAR T cells were detected both in the blood and the chylous ascites by flow cytometry, which peaked on day 14 in the blood.
B-cell aplasia, cytokine change, and laboratory testingThe patient had B-cell aplasia before CAR T infusion, which was likely due to a previous Rituximab treatment. The B cell counts remained depleted until day 72, when it recovered to 25 μl-1. Repeated intravenous IG was administered when the serum IgG level decreased to lower than 4 to 5 g/L. The level of cytokines detected by flow fluorometry generally showed a fluctuation within the normal range of IL-4, IL-6, IL-10, TNFα, and IFNγ, with a moderate rise of IL-6 on the first day after CAR T cell infusion, which was in accordance with the mild CRS (Supplementary Figure S2). The WBCs and neutrophils were reduced sharply after preconditioning and reached the lowest level within the first week after infusion. Granulocyte colony-stimulating factor (G-CSF) was used intermittently. At nearly 2 months, the WBCs recovered to over 3.0 × 109/L. The platelet counts decreased to the lowest level of 91 × 109/L; however, it recovered quickly. The liver enzymes were detected to have slightly increased at 1-month evaluation, probably reflecting the infiltrating CAR T cells that fought against liver lesions.
DiscussionThe three CD19-directed CAR T therapies approved by FDA, Axi-cel, Tisa-cel, and Liso-cel, are all prepared by viral vectors and complex manufacturing processes. The emerging non-viral gene-transferred CD19 CAR T products have not been approved for relapsed/refractory B cell lymphoma. This new approach could potentially reduce the costs and complexity associated with recombinant viral vector-based immunotherapy. There are also other clinical benefits as shown in our case.
In our case, the peak value of pbCAR T cell expansion was 48.97 μl-1 on day 14, accounting for 14.73% of all lymphocytes, which was similar to that prepared by viral vectors (15). Interestingly, no severe CRS or neurotoxicity was observed during the pbCAR T treatment, probably because the activated CD19pbCAR-T cells showed relatively low levels of IL-6. Kebriaei P et al. safely conducted a clinical trial using “sleeping beauty (SB)” to generate CD19-specific CAR T cells as adjuvant therapy to treat 26 patients with advanced B cell lymphoma or acute lymphoblastic leukemia following hematopoietic stem cell transplantation (16, 17). Li et al. reported a case of triple-hit relapsed/refractory diffuse LBCL with TP53 mutation, treated with Piggy Bac-generated CAR19-T cells, who obtained a CR in the second month with grade 2 CRS (18). In our case, despite B-cell recovery on day 72 after infusion, the response was still ongoing at 3 months post-infusion, which may be attributed to the pbCAR T cell’s inclination to memory type that kept CAR T cell persistence and the disease under control.
This patient had severe chylous ascites and a medium volume of left pleural effusion before CAR T cell therapy. The patient with pre-CAR T effusions generally had malignant effusions. The fluid accumulations may develop or worsen during the CRS process, leading to significant toxicities and death. In the Zuma-1 trial, patients with pre-existing symptomatic pleural effusions were excluded from the trial. Mirza AS et al. retrospectively analyzed 148 patients receiving CD19 CAR T for LBCL, including 19 patients with a pre-CAR T effusion, and 17 patients without a pre-existing effusion developed a new effusion after CAR T. Compared with patients with no effusions, patients with pre-CAR T effusions had a higher frequency of high-risk baseline characteristics, such as bulky disease and high IPI. Similarly, patients with pre-CAR T effusions had a higher rate of grade 3 or worse CRS (32% vs. 5%). Moreover, on multivariate analysis, pre-CAR T effusions were associated with reduced OS and higher non-relapse mortality (13).
The patient in this study had bulky disease with a large volume of ascites before CAR T therapy. She needed drainage every day during lymphodepleting and the first week after CAR T infusion. However, 2 weeks later, we observed a decrease in peritoneal effusions, and the patient needed drainage every 3 or 4 days. The CAR T cells could be detected on day 7 in the ascites, and the absolute value was higher than that in the blood, showing good penetration and infiltration of CAR T cells from peripheral blood to the peritoneum. Lin et al. observed a higher level of distribution of anti-CD19 pbCAR T cells in mesenteric lymph nodes, bone marrow of the femur, spleen, kidneys, and lungs, specifically accumulating at CD19-rich sites and CD19-positive Raji cell-induced tumors (19). During the whole CAR T process, the patient did not feel any pain or discomfort in the abdominal cavity. In the PET-CT on day 28, the left pleural effusion was invisible, and the ascites was remarkably reduced.
The long-term follow-up of Zuma-1 has shown excellent results of Axi-cel for relapsed/refractory LBCL. The overall objective response rate (ORR) was 83%, with a CR rate of 58%, and the 5-year OS was 42.6%. In the trial for relapsed/refractory follicular lymphoma and marginal zone lymphoma, Zuma-5 has reached extraordinary results, which are better than those for aggressive lymphoma. The ORR was 92%, with a CR rate of 76%. With a median follow-up of 17.5 months, the median progression-free survival was not reached. Cappell KM et al. also reported on a long-term follow-up of anti-CD19 CAR T cells for 28 cases with LBCL, eight cases with low-grade B-cell lymphoma, and seven cases with chronic lymphocytic leukemia. The percentage of more than 3-year duration of response was higher for patients with low-grade lymphoma than that for patients with LBCL (63% vs. 48%). The median event-free survival (EFS) for all patients with LBCL was 15 months; however, the median EFS for patients with low-grade lymphoma was 55 months (20). So, CD19-directed CAR T cell therapy might be a very powerful therapeutic strategy for relapsed/refractory low-grade lymphoma, with a higher ORR rate and CR rate and good response durability.
Our case of relapsed follicular lymphoma was one with a high tumor burden, involving multiple groups of superficial and deep lymph nodes, liver, lungs, adnexa, omentum, and mesentery. The tumor mass responded rapidly after CD19 CAR T cell infusion, as seen by the unpalpated enlarged cervical lymph nodes within 1 week, and the day 28 PET-CT showed nearly CMR. At 3 months, the response was ongoing. Furthermore, the patient did not have any infection during the whole process, having been given G-CSF, prophylactic antibiotics, and an intermittent supply of immunoglobulin.
In conclusion, Piggy Bac-generated CD19-directed CAR T cells could be a powerful therapeutic choice for refractory or relapsed follicular lymphoma, which showed good efficacy and safety despite the high tumor burden. Long-term efficacy, quality-of-life follow-up, and more cases are warranted for further evaluation.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Ethics statementThe studies involving human participants were reviewed and approved by the institutional review board (IRB) for Shanghai Mengchao Cancer Hospital. The IRB approval number is SHMCCH-IEC/21-06/05. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the patient for the publication of any identifiable data/information.
Author contributionsYZ, ZLin, YS, and QQ designed the study. YZ and ZLin wrote the paper. ZLi revised the paper and gave good advice. YZ analyzed the data and made the figures. FZ and XC were physicians in charge of the patient. Acquisition of data was done by YY and XF. All authors contributed to the article and approved the submitted version.
FundingThe study received funding from Shanghai Cell Therapy Group Corporation (BZ019). All authors declare no other competing interests.
AcknowledgmentsThe authors would like to thank the patient and his family for their participation in and support of the study. We would also like to express our appreciation to all the doctors, nurses, and researchers at the hospital, the cell drug business unit, and Baize medical laboratory who assisted during the study. We thank Professor Dong Chen (Division of Hematopathology, Mayo Clinic, Rochester, MN) for his critical review of the paper and important advice both in Science and English.
Conflict of interestAuthors ZLin, YY, XF, ZLi, YS, and QQ were employed by Shanghai Cell Therapy Group Corporation.
The authors declare that this study received funding from Shanghai Cell Therapy Group Corporation. The funder had the following involvement in the study: the study design, collection of data and the writing of this article.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary materialThe Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2022.1007210/full#supplementary-material
Supplementary Figure 1 | Expansion of CD3+CD8+CAR+ and CD3+CD45RA-CCR7+CAR+ T cells. The latter of central memory-like cells could still be detected at 3 months.
Supplementary Figure 2 | Change of cytokines. The level of cytokines detected by flow fluorometry generally showed fluctuation within the normal range of IL-2, IL-4, IL-6, IL-10, TNFα, and IFNγ.
AbbreviationsCAR T, chimeric antigen receptor T; pb, Piggy Bac; CRS, cytokine release syndrome; CR, complete response; OS, overall survival; LBCL, large B-cell lymphoma; CMR, complete metabolic remission; PET-CT, positron emission tomography-computed tomography; FLIPI, follicular lymphoma international prognostic index; PBMCS, peripheral blood mononuclear cells; WBCs, white blood cell counts; SUV, standard uptake value; IG, immunoglobulin; G-CSF, granulocyte colony-stimulating factor; ALT, alanine transaminase; AST, aspartate aminotransferase; SB, sleeping beauty; HSCT, hematopoietic stem cell transplantation; ORR, objective response rate; PFS, progression-free survival; EFS, event-free survival.
References1. Schuster SJ, Tam CS, Borchmann P, Worel N, McGuirk JP, Holte H, et al. Long-term clinical outcomes of tisagenlecleucel in patients with relapsed or refractory aggressive b-cell lymphomas (JULIET): A multicentre, open-label, single-arm, phase 2 study. Lancet Oncol (2021) 22(10):1403–15. doi: 10.1016/S1470-2045(21)00375-2
PubMed Abstract | CrossRef Full Text | Google Scholar
2. Locke FL, Ghobadi A, Jacobson CA, Miklos DB, Lekakis LJ, Oluwole O, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large b-cell lymphoma (ZUMA-1): A single-arm, multicentre, phase 1–2 trial. Lancet Oncol (2019) 20(1):31–42. doi: 10.1016/S1470-2045(18)30864-7
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Abramson JS, Palomba ML, Gordon LI, Lunning MA, Wang M, Arnason J, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large b-cell lymphomas (TRANSCEND NHL 001): A multicentre seamless design study. Lancet (2020) 396(10254):839–52. doi: 10.1016/S0140-6736(20)31366-0
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Nastoupil LJ, Jain MD, Feng L, Spiegel JY, Ghobadi A, Lin Y, et al. Standard-of-Care axicabtagene ciloleucel for relapsed or refractory Large b-cell lymphoma: Results from the US lymphoma CAR T consortium. J Clin Oncol (2020) 38(27):3119–28. doi: 10.1200/JCO.19.02104
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Jacobson CA, Locke FL, Ghobadi A, Miklos DB, Lekakis LJ, Oluwole O, et al. Long-term (≥4 year and ≥5 year) overall survival (OS) by 12- and 24-month event-free survival (EFS): An updated analysis of ZUMA-1, the pivotal study of axicabtagene ciloleucel (Axi-cel) in patients (Pts) with refractory Large b-cell lymphoma (LBCL). Blood (2021) 138(Supplement 1):1764. doi: 10.1182/blood-2021-148078
CrossRef Full Text | Google Scholar
6. Jacobson CA, Chavez JC, Sehgal AR, William BM, Munoz J, Salles G, et al. Axicabtagene ciloleucel in relapsed or refractory indolent non-Hodgkin lymphoma (ZUMA-5): A single-arm, multicentre, phase 2 trial. Lancet Oncol (2022) 23(1):91–103. doi: 10.1016/S1470-2045(21)00591-X
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Westin JR, Kersten MJ, Salles G, Abramson JS, Schuster SJ, Locke FL, et al. Efficacy and safety of CD19-directed CAR-T cell therapies in patients with relapsed/refractory aggressive b-cell lymphomas: Observations from the JULIET, ZUMA-1, and TRANSCEND trials. Am J Hematol (2021) 96(10):1295–312. doi: 10.1002/ajh.26301
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Moretti A, Ponzo M, Nicolette CA, Tcherepanova IY, Biondi A, Magnani CF. The past, present and future of non-viral CAR T cells. Front Immunol (2022) 13:867013. doi: 10.3389/fimmu.2022.867013
PubMed Abstract | CrossRef Full Text | Google Scholar
10. He J, Zhang Z, Lv S, Xiangzhen Liu XZ, Cui LZ, Jiang DQ, et al. Engineered CAR T cells targeting mesothelin by piggyBac transposon system for the treatment of pancreatic cancer. Cell Immunol (2018) 329:31–40. doi: 10.1016/j.cellimm.2018.04.007
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Zhang YJ, Zhang ZW, Ding YM, Fang Y, Wang P, Chu WQ, et al. Phase I clinical trial of EGFR-specific CAR-T cells generated by the piggyBac transposon system in advanced relapsed/refractory non-small cell lung cancer patients. J Cancer Res Clin Oncol (2021) 147(12):3725–34. doi: 10.1007/s00432-021-03613-7
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Neelapu SS, Locke FL, Bartlett NL, Lekakis LJ, Miklos DB, Jacobson CA, et al. Axicabtagene ciloleucel CAR T-cell therapy in refractory large b-cell lymphoma. N Engl J Med (2017) 377(26):2531–44. doi: 10.1056/NEJMoa1707447
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Mirza AS, Kumar A, Hashmi H, Garcia F, Logothetis CN, Darwin A, et al. Incidence and management of effusions before and after CD19-directed chimeric antigen receptor (CAR)T cell therapy in large b cell lmphoma. Transplant Cell Ther (2021) 27(3):242.e1–6. doi: 10.1016/j.jtct.2020.12.025
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Fang JM, Ding N, Guo XL, Sun Y, Zhang ZW, Xie BL, et al. αPD-1-mesoCAR-T cells partially inhibit the growth of advanced/refractory ovarian cancer in a patient along with daily apatinib. J Immunother Cancer (2021) 9(2):e001162. doi: 10.1136/jitc-2020-001162
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Spiegel JY, Patel S, Muffly L, Hossain NM, Oak J, Baird JH, et al. CAR T cells with dual targeting of CD19 and CD22 in adult patients with recurrent or refractory b cell malignancies: A phase 1 trial. Nat Med (2021) 27(8):1419–31. doi: 10.1038/s41591-021-01436-0
PubMed Abstract | CrossRef Full Text | Google Scholar
16. Kebriaei P, Singh H, Huls MH, Figliola ML, Bassett R, Olivares S, et al. Phase I trials using sleeping beauty to generate CD19-specific CAR T cells. J Clin Invest (2016) 126(9):3363–76. doi: 10.1172/JCI86721
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Srour SA, Singh H, McCarty J, Groot ED, Huls H, Rondon G, et al. Long-term outcomes of sleeping beauty-generated CD19-specific CAR T-cell therapy for relapsed-refractory b-cell lymphomas. Blood (2020) 135(11):862–5. doi: 10.1182/blood.2019002920
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Li C, Sun Y, Wang J, Tang L, Jiang HW, Guo T, et al. PiggyBac-generated CAR19-T cells plus lenalidomide cause durable complete remission of triple-hit Refractory/Relapsed DLBCL: A case report. Front Immunol (2021) 12:599493. doi: 10.3389/fimmu.2021.599493
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Lin ZC, Liu XZ, Liu T, Gao HX, Wang ST, Zhu XL, et al. Evaluation of nonviral piggyBac and lentiviral vector in functions of CD19 chimeric antigen receptor T cells and their antitumor activity for CD19+ tumor cells. Front Immunol (2022) 12:802705. doi: 10.3389/fimmu.2021.802705
PubMed Abstract | CrossRef Full Text | Google Scholar
20. Cappell KM, Sherry RM, Yang JC, Goff SL, Vanasse DA, McIntyre L, et al. Long-term follow-up of anti-CD19 chimeric antigen receptor T-cell therapy. J Clin Oncol (2020) 38(32):3805–15. doi: 10.1200/JCO.20.01467
留言 (0)