
記住我







Parkinson’s disease (PD) is a neurodegenerative disorder that significantly affects motor function in these patients. The ability to walk is a primary concern in independent daily living for individuals with PD (Montero-Odasso et al., 2005). The situation of walking with a concurrent manual task (e.g., walking and carrying a plate filled with food) is common in daily life. For individuals with PD, especially those who can still walk without a walking aid, the ability to safely dual-task walk is essential for good quality of life. However, dual-task interference accentuates gait impairment (e.g., slower walking velocity, shortened stride length, and greater stride-to-stride variability), leading to a higher risk of falling (Kelly et al., 2012; van der Marck et al., 2014; Orcioli-Silva et al., 2020). In addition, the gait impairments in walking velocity, stride length, and stride-to-stride variability are worsened in the off-medication state (McNeely and Earhart, 2013; Orcioli-Silva et al., 2020; Stuart et al., 2020). For poor proprioceptive-motor integration, individuals with PD often have smaller stride lengths and swing amplitudes than they planned (Iansek et al., 2013), underlying a loss of neuronal response specificity in the cortico-basal ganglia-thalamo-cortical loop (Maschke et al., 2003; Vinding et al., 2019). The lack of kinesthetic awareness in PD can be alleviated by altering the cognitive state. For example, greater gait velocity and longer step length have been observed in individuals with PD when they use an awareness strategy (or attentional cuing) to focus on “taking big steps” (Canning, 2005; Baker et al., 2007; Lowry et al., 2010; Lohnes and Earhart, 2011). This awareness strategy has been shown to be effective for both single-task walking and dual-task walking (Canning, 2005; Baker et al., 2007; Lowry et al., 2010; Lohnes and Earhart, 2011).
Human walking is not a completely automatic process under subcortical control. Spatially distant cortical areas (e.g., frontal, parietal, temporal, and occipital areas) are activated and synchronized during human walking (Takakusaki, 2017; Wang and Choi, 2020). In heathy adults, cortical oscillatory activities in the alpha and beta bands are tuned to the attentional and sensorimotor processes (Engel and Fries, 2010; Başar, 2012), which are often modulated during single-task walking and various settings of dual-task walking (Beurskens et al., 2016; Protzak and Gramann, 2021). To compensate for basal ganglia dysfunction, individuals with PD often exhibit a broader range of activation and enhanced cortico-cortical connectivity during single-task walking and dual postural-motor tasks (Maidan et al., 2016a,b; Asher et al., 2021; Huang et al., 2022). The severity of gait impairment in individuals with PD is proportional to the synchronization strength in alpha and beta bands among frontal-motor-parietal areas (Asher et al., 2021). PD manifests with excessive phase synchronization in the alpha band during locomotion (Miron-Shahar et al., 2019). The use of an external cuing strategy for goal-directed control of PD gait results in a compensatory decrease in parieto-occipital alpha band activity, underlying the increased visual attention being paid to relevant information from the environment (Stuart et al., 2021; Tosserams et al., 2022). Compared to single-task walking, individuals with PD increased beta activity in response to dual-task walking that reflects the taxing of additional cognitive resources in more challenging tasks (Possti et al., 2021). There is also evidence of a strong frequency-correlation, showing a mechanistic linkage between abnormal beta oscillation and pathological motor processes in PD (Little and Brown, 2014). Individuals with PD who have bradykinesia, rigidity, or tremulous movement also demonstrate excessively high beta activity in the sensorimotor cortex and basal ganglia (Engel and Fries, 2010). The enhanced beta oscillations of regional and inter-regional activities are harmful to the coding of kinesthetic information prior to initiating a new movement, as greater beta oscillations in the motor loop favor persistence of the status quo (Engel and Fries, 2010).
Although the awareness strategy relies internally on cognitive mechanisms to improve gait control in PD (Iansek et al., 2013), the underlying neural mechanism of internal cueing, such as focusing on movement amplitude, remains unknown. However, it is expected to involve complex integrative functions with adaptive changes in large-scale cortical assemblages. Within the context of brain connectivity, this study aimed to investigate the effect of stride awareness in taking big steps in dual-task walking for individuals with PD. We focused on the awareness-related modulation of brain functional connectivity in the alpha and beta bands. In addition, this study aimed to assess the functional linkages between awareness-related changes in electroencephalography (EEG) functional connectivity and gait variables for dual-task walking. The study was designed to provide insight into the neurological mechanisms of stride awareness to improve dual-task walking in PD. Due to potential variations in sensorimotor processing, we hypothesized that individuals with PD would have less functional connectivity strength in alpha and beta subnetworks with better walking performance when they walked with an awareness strategy than when they walked without an awareness strategy. We also hypothesized that awareness-related changes in walking performance would be associated with awareness-related changes in functional connectivity, especially in the beta band.
Materials and methods ParticipantsEighteen individuals with PD (mean age: 63.1 ± 7.7 years) participated in this study. The inclusion criteria were: a diagnosis of idiopathic PD according to the United Kingdom PD Society Brain Bank clinical diagnostic criteria (Hughes et al., 1992), PD onset ≥40 years of age, and had a symptoms of mild gait impairment (no moderate or severe gait impairment). In the present study, mild gait impairment was defined as scores of 1 or 2 on item 2.12 (walking and balance) and item 3.10 (gait) of the MDS-sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS). Item 2.12 and item 3.10 of the MDS-UPDRS are scored from 0 to 4 (Goetz et al., 2008). For item 2.12, the participants were asked about their walking and balance ability over the past week. A score of 1 on item 2.12 indicates the person had a symptom of slightly slow walking or leg drag, and never use a walking aid. A score of 2 on item 2.12 indicates the person occasionally used a walking aid, and did not need any help from other person. For item 3.10, the participants were asked to walk at least 10 meters, then turn around and return to the examiner. The measured items include stride amplitude, stride speed, height of foot lift, heel stride during walking, turning, and arm swing. A score of 1 or 2 on item 3.10 indicates the person can walk independently with minor or substantial gait impairment, and do not require an assistance device. Patients were excluded if they had a Mini-Mental State Examination (MMSE) score < 26, a history of brain surgery or other diseases and conditions that could influence balance ability, or a score > 2 on item 3.15 (postural tremor) and item 3.16 (kinetic tremor) of the MDS-UPDRS. A score > 2 on item 3.15 and item 3.16 indicates moderate or severe postural tremor or kinetic tremor in the hands, which may affect the accuracy of a manual task. Table 1 presents the demographic data and clinical characteristics of the participants. All procedures in this study were approved by the National Taiwan University Hospital Research Ethics Committee (Clinical Trial Registration No. NCT03298503), and all participants provided written informed consent.
Table 1. Patient demographics and characteristics.
The sample size was calculated based on data from a previous study (Lohnes and Earhart, 2011), which indicated that 17 participants would be sufficient to detect the effect of stride awareness on dual-task walking (Cohen’s d = 0.85, power = 0.9, α = 0.05).
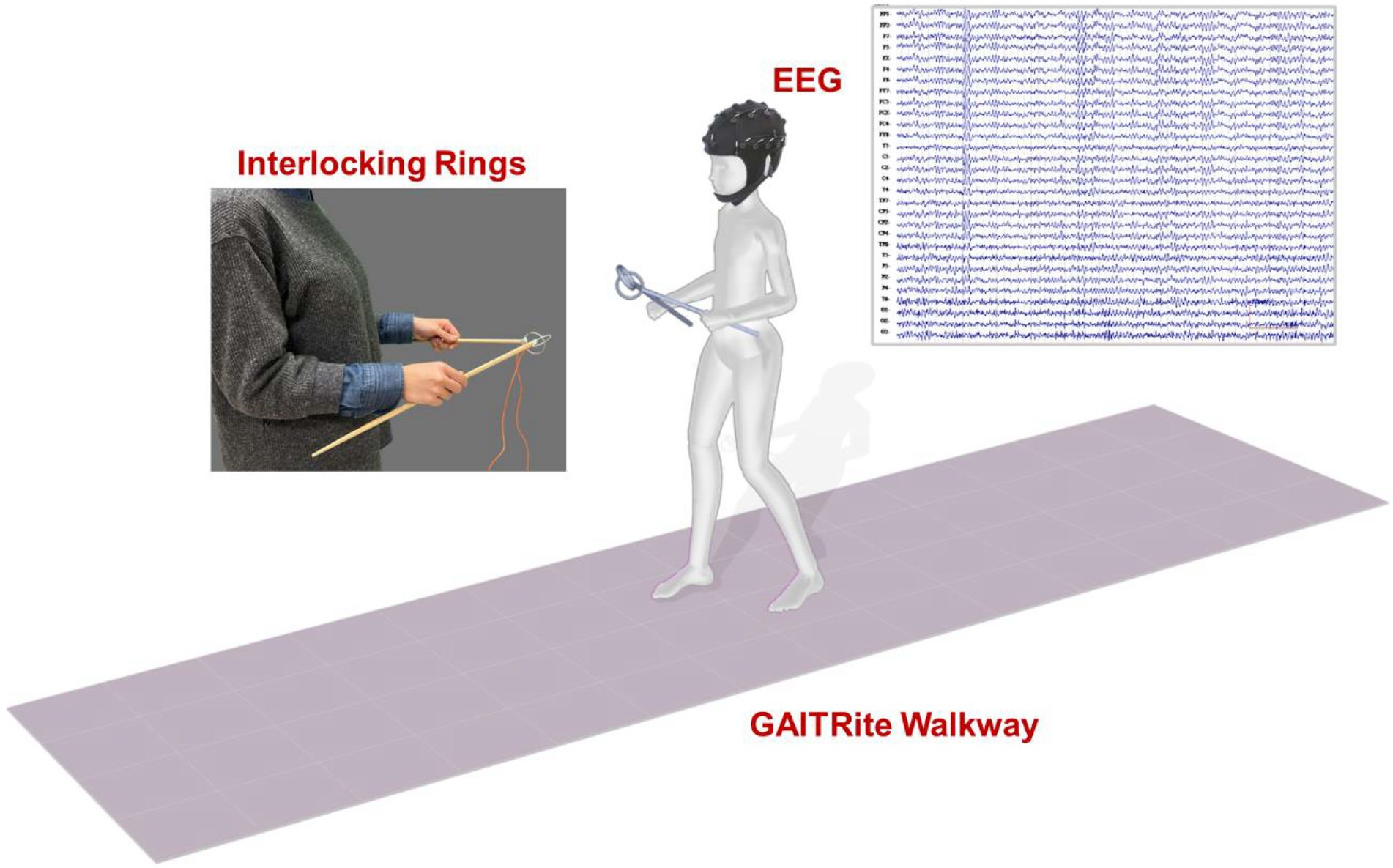
Experimental apparatus and data recordingThe participants were instructed to walk on an electronic walkway (GAITRite, CIR Systems Inc., United States; sampling rate: 100 Hz) while controlling a pair of interlocking rings (Figure 1). The length of the GAITRite walkway was 5.20 m, with an active area of 4.27 m. To stabilize gait measures with the GAITRite walkway, the participants walked 2 m before and after the walkway for acceleration and deceleration. For the ring task, participants held two sticks and kept their elbows in 90° flexion. Attached to the end of each stick was a metal ring (diameter: 4 cm), and the two rings were interlocked (Beurskens et al., 2016; Huang et al., 2022). The participants were asked to prevent the two rings from touching each other. When the two rings touched, the computer recorded the event with an A/D card (USB-6221, National Instruments, United States; sampling rate: 1 kHz).
Figure 1. Diagram of the experimental setup.
Cortical activities were recorded using a NuAmps 32-channel amplifier (NeuroScan Inc., United States). The EEG amplifier (height: 198 mm, width: 151 mm, depth: 40 mm, weight: 630 grams) was carried by participants in a backpack after proper fixation during locomotion like a mobile EEG system. The length of EEG wires outside the backpack was adjusted and fixed on participants’ upper back by several adhesive tapes to avoid movement artifacts caused by the movement of EEG wires. The cable connecting the EEG amplifier and recording computer was suspended to avoid interfering with walking. The similar method was used in a previous study for investigating gait initiation and stepping control (do Nascimento et al., 2005). The EEG electrodes (Fp1/2, Fz, F3/4, F7/8, FT7/8, FCz, FC3/4, Cz, C3/4, CPz, CP3/4, Pz, P3/4, T3/4, T5/6, TP7/8, Oz, and O1/2) were placed based on the 10–20 electrode system of the International Federation. The ground electrode was placed along the midline, ahead of Fz. To monitor vertical and horizontal eye movements and blinks, electrodes were placed above the left eyebrow, below the left eye, and horizontally on the outer canthi of both eyes. The impedances of all electrodes were ≤5 kΩ, and all electrodes were referenced to linked mastoids of both sides. EEG data were band-pass filtered at 0.1–100 Hz with a 1 kHz sampling rate. All behavioral data and EEG data were synchronized.
Experimental conditionsAll clinical assessments and dual-task walking examinations were performed in the morning on the same day, at least 12 h after the most recent administration of anti-parkinsonian medications (off-medication test) (Langston et al., 1992). There were two test conditions in this study: the non-awareness strategy (NAS) and the awareness strategy (AS). In the NAS condition, the participants were instructed to walk at their preferred speed and prevent the interlocking rings from touching. In the AS condition, the participants were instructed to pay attention to “taking big steps” while walking and prevent the interlocking rings from touching. The instruction was provided at the beginning of each test trial to emphasize the strategy application of non-awareness and awareness. The NAS condition was administered first to avoid carryover effects of walking awareness (Baker et al., 2007; Lowry et al., 2010). Two practice trials were conducted before eight testing trials in each experimental condition. Each test trial contained 7–9 walking steps (3–4 gait cycles per trial: 24–32 gait cycles per condition). Participants were asked to look straight ahead to avoid different postures or visual attention (e.g., looking at the rings or feet) during the test. The resting time was 30 s between two testing-trails and was 1 min between the NAS and AS conditions. Immediately following each test trial, participants were asked to rate the percentage of their attention that they felt had been directed towards walking in the NAS condition, or towards taking big steps in the AS condition, using an analogue scale (0–100%) to confirm the attentional allocation in each test trial (Canning, 2005).
Data analysisFor the walking task, velocity, cadence, step length, and the coefficient of variation (CV) of step length were calculated. For the ring task, ring-touch time, which is the percentage of time in which the rings were touching in a walking trial, was calculated for each trial.
Using the NeuroScan software program (NeuroScan Inc., El Paso, TX, United States), the blinks and eye movements were corrected through the creation of bipolar vertical electrooculogram (EOG) channels by subtracting the activity in the infraorbitally placed electrode from the activity in the supraorbitally placed electrode, and the creation of bipolar horizontal EOG channels by subtracting the activity of the two electrodes placed on the outer canthi of both eyes. The conditioned EEG data were segmented with respect to gait cycles between two successive heel strikes by the same leg. The pre-processed EEG data were further conditioned with a phase-invariant impulse response (FIR) filter in the two frequency sub-bands: alpha (8–12 Hz) and beta (13–35 Hz). We did not analyze EEG data under 6 Hz (i.e., delta and theta bands) for potential contamination of movement artifacts during locomotion (Gwin et al., 2011). To characterize the strength of the inter-regional connectivity for the alpha and beta bands, a phase-lag index (PLI) was applied to EEG epochs of each gait cycle for all 30 electrode pairs in the alpha band and beta band, respectively (Figure 2). PLI was selected because this connectivity index is insensitive to common sources, such as volume conduction (Stam et al., 2007). Based on the Hilbert transformation (Stam et al., 2007), the PLI features the distribution asymmetry of phase differences in the instantaneous phases between a given pair of EEG epochs. If φ(t) is the phase difference, the PLI is defined as:PLI=E
留言 (0)