1. IntroductionLumbar degenerative disease is a common disease in spinal surgery that mostly occurs in the elderly, with main clinical manifestations such as sciatica, low back pain, and cauda equina syndrome. Recently, transforaminal lumbar interbody fusion (TLIF) has become a common surgical approach for the clinical treatment of lumbar degenerative disease [
1]. The advantage of TLIF is that the nerve is exposed laterally by removing part of the facet joint, and the traction of the nerve root is reduced to avoid potential nerve injury. TLIF preserves the integrity of the posterior column by reducing the removal of the spinous process. OPEN-TLIF has been a safe and effective lumbar fusion procedure [
2]. A systematic review of 192 studies concluded that OPEN-TLIF has advantages over PLIF in complication rate, blood loss, and operation duration. The clinical outcome is similar, with a slightly lower postoperative ODI score for TLIF [
3]. However, extensive dissection of the paraspinal muscles is required in the MIS-TLIF procedure, and this may result in postoperative paravertebral muscle atrophy and low back pain [
4]With the progress of spinal surgery technology and the development of minimally invasive surgical techniques, Foley et al. [
5] proposed in 2002 to complete TLIF surgery under an expandable tube via the wistle approach, and named this minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF). The decompression and fusion procedure can be operated between the multifidus muscle and longissimus muscle to reduce the injury of paraspinal muscles and soft tissues [
6]. Previous studies concluded that there was no significant difference in postoperative quality of life score between Open-TLIF and MIS-TLIF [
7,
8], and some scholars believed that MIS-TLIF was superior to OPEN-TLIF in intraoperative blood loss and bedridden time [
9,
10]. However, almost all the conclusions were based on single-segment lumbar degenerative diseases [
9,
10,
11,
12,
13], and the merits of the two surgical methods in two-segment lumbar diseases are still controversial.With the aging of the population, patients with two segments lumbar degenerative diseases are not uncommon. According to a long-term follow-up study, about 20% of patients with lumbar degenerative diseases have two or more levels of lumbar disc herniation [
14]. For these patients, multilevel surgery may be necessary, and choosing a more appropriate surgical procedure will reduce surgical trauma. Whether MIS-TLIF still has advantages for two segments degenerative lumbar diseases is still debatable. To our knowledge, there has been no literature focused on the comparison of the two surgical methods for two segments disorders. In clinical practice, we found that the two surgical methods have similar efficacy. In order to verify this hypothesis, a total of 112 patients with lumbar degenerative diseases of two segments treated in our institution from January 2015 to September 2021 were included in this study. MIS-TLIF and Open-TLIF were used for surgical treatment, and we compared the clinical and radiological outcomes of the two methods. 2. Materials and Methods 2.1. Inclusion and Exclusion Criteria
Inclusion criteria: (1) patients with typical clinical manifestations of lumbar spinal stenosis, lower extremity neurological symptoms, low back and leg pain and failed to respond to standard conservative treatment for 3 months; (2) lumbar imaging examination showed spinal stenosis with or without lumbar spondylolisthesis; (3) CT and MRI confirmed two-level disc degeneration, the abnormal changes in imaging was consistent with clinical symptoms.
Exclusion criteria: (1) deformity or combined with grade III or above lumbar spondylolisthesis; (2) lumbar infection, tumor, severe osteoporosis or motor neuron disease; (3) patients who had undergone lumbar surgery or local block therapy; (4) incomplete imaging data and loss of follow-up.
2.2. General Information of PatientsA total of 112 patients with lumbar degenerative diseases of two segments were included according to the inclusion and exclusion criteria. There were 60 patients in the OPEN-TLIF group, which was also treated as the control, including 34 males and 26 females. There were 52 patients in MIS-TLIF group, including 28 males and 24 females. There was no significant difference in preoperative general information between the two groups (
Table 1). All patients were treated by experienced physicians using the Quadrant minimally invasive operating system (Beijing Fule Technology Development Co., Ltd., Beijing, China). This study was reviewed and approved by the Ethics Committee of Henan Provincial People’s Hospital(IRB approval number 2021–173). All patients signed informed consent. 2.3. Surgical Method of OPEN-TLIF
After general anesthesia, patients in the Open-TLIF group were placed in a prone position, and the operation area was routinely disinfected. The paravertebral muscle was separated from the spinous process, lamina, and facet capsule. The facet joints were exposed, three pedicle screws were inserted. The facet joint was bitten, the lamina was removed, the hyperplastic ligamentum flavum was removed, the dural sac and nerve roots were exposed, the protruding nucleus pulposus was removed, the intervertebral disc tissue was cleaned, the upper and lower cartilaginous endplates were scraped, the trimmed bone particles were implanted in the intervertebral space, and the cage was implanted in an oblique way. Whether to perform contralateral decompression was determined according to the preoperative symptoms and imaging manifestations. A paravertebral drainage tube was implanted, and the incision was sutured layer by layer.
2.4. Surgical Method of MIS-TLIF
The anesthesia mode and intraoperative position of patients in MIS-TLIF group were consistent with those in the OPEN-TLIF group. A posterior median incision was made, the subcutaneous skin was separated, and the skin was separated to the fascia layer on both sides. The fascia was cut 2 cm beside the midline at the intermuscular space between the longissimus muscle and multifidus muscle. A guide wire was implanted in the muscle space by blunt separation. After confirming the correct location, the quadrant channel was inserted. The remaining surgical procedures were the same as OPEN-TLIF surgery.
2.5. Postoperative Management
Prophylactic antibiotics were applied for 72 h after operation, and tower limb activity and symptom relief of patients were observed regularly. Braces were worn regularly for 3 months. Follow-up was performed at 1 week, 6 and 12 months after operation. X-ray and CT examinations were performed.
2.6. Observational Index
We used VAS score and ODI index to evaluate the clinical efficacy after the surgery. VAS score for low back pain and VAS score for leg pain and ODI index were recorded before operation, 1 week, 3 months and 12 months after operation.
Muscle injury during the perioperative period was evaluated according to the changes of blood creatine kinase (CK), and the CK content of the two groups was measured at preoperative, 3 days and 1 week after operation.
Postoperative intervertebral fusion was evaluated by the grading of lumbar fusion proposed by Bridwell et al. [
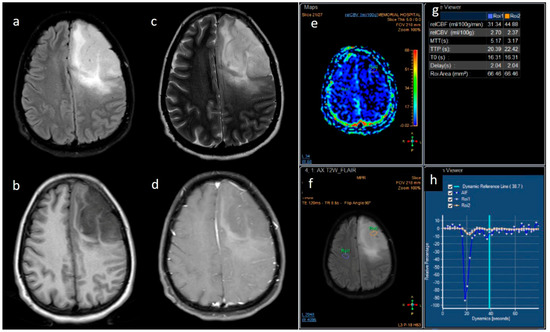
15]. Grade 1 showed complete fusion of the intervertebral space with trabecular reconstruction, and the grade 2 showed incomplete fusion of the intervertebral space with trabecular reconstruction.The screw position was evaluated by the classification proposed by Rao et al. [
16]. Type A0 means that the screw did not penetrate the medial wall of the pedicle. Type A1 means that the screw penetrated the medial wall of the pedicle less than 2 mm. Type A2 means that the screw penetration of the medial wall of the pedicle was greater than 2 mm and less than 4 mm. Type B0 means that the screw did not penetrate the lateral wall of the pedicle. Type B1 means that the screw penetrated the lateral wall of the pedicle less than 2 mm. Type B2 means that the screw penetrated the lateral wall of the pedicle more than 2 mm and less than 4 mm.(
Figure 1). 2.7. Statistical Analysis
SPSS 22.0(SPSS Inc., Chicago, IL, USA) was used for comparison and analysis of all data. Counting data were expressed as (X ± s). Normality of the data distribution was confirmed by Shapiro–Wilk testing. An independent sample T-test was used for comparison of the operation time, fluoroscopy, the amount of bleeding, the volume of drainage and the bed rest time between the two groups. An independent sample T-test was also used to compare the quality-of-life scores at each follow-up point between the two groups. Measurement data are expressed as (n%) and the Chi-square test was used for comparison of the general information of the patients, the complications after surgery and the distribution of screw types. Effect size (Cohen d) was calculated to examine the effect of statistical differences, and was classified as weak (≤0.49), moderate (0.5–0.79), or large (≥0.8). p < 0.05 was considered significant.
4. DiscussionThe clinical efficacy of OPEN-TLIF were verified [
17,
18]. Kunder et al. [
17] compared the advantages and disadvantages of PLIF and OPEN-TLIF in a meta-analysis, and the results showed that OPEN-TLIF was superior to PLIF in terms of operation time, intraoperative blood loss, and incidence of complications. MIS-TLIF adopts the paravertebral space approach to complete decompression and intervertebral bone fusion through an expandable channel, which can preserve the integrity of paravertebral muscles and posterior structures of the vertebral body [
19,
20]. However, the channel limits the operation space, experienced surgical techniques and necessary surgical tools are required, and the learning curve is steep [
21]. In this study, we found that the postoperative quality of life score and radiological outcomes of the two methods was similar but the operation time and intraoperative radiation exposure were higher in the MIS-TLIF group. A typical case is shown in
Figure 3.During follow-up we found that the VAS score of low back pain in the MIS-TLIF group was lower than that in the OPEN-TLIF group 1 week after operation (p
22,
23].We found that the MIS-TLIF group had higher operation time and fluoroscopy times. The increase of fluoroscopy prolonged the operation time and increased radiation exposure to doctors and patients. A number of studies have also confirmed this conclusion [
24,
25]. Arif et al. [
26] found that the operation time of MIS-TLIF was increased by 126.3 min and fluoroscopy time was increased by 22.9 s compared with the traditional method. By monitoring the exposure dose, related research found that the radiation dose of MIS-TLIF surgery was 30 µSV higher than conventional surgery.
CK levels measured at 3 and 7 days after surgery were similar in the two groups. Muscle injury results in an increase in cell membrane passage, which leads to the release of CK into the bloodstream. Continuous monitoring of CK after surgery showed that there was no significant difference in muscle injury between the two groups. MIS-TLIF surgery is designed to minimize muscle irritation, but our study found that when MIS-TLIF was extended to 2-level surgery, the results of muscle injury did not improve compared with OPEN-TLIF.
According to Bridwell classification, there was no significant difference in the postoperative interbody fusion rate between the two groups (p
18] found that there was no significant difference in interbody fusion rate between MIS-TLIF (RR = 2.13, 95%CI: 1.39–3.27) and OPEN-TLIF (RR = 2.13, 95%CI: 1.39–3.27). This is consistent with the results of our study. Kim et al. [
13] conducted a 5-year follow-up study on the fusion results of MIS-TLIF, and the authors found that the fusion rate was 97.7%. All these studies showed that the postoperative fusion rate could achieve satisfactory results whether open or minimally invasive.In this study, we found no significant difference in the incidence of complications between the two groups. However, concerning dural tear, we found the incidence of dural tear was higher in the MIS-TLIF group. Dural tears occurred in six cases in the MIS-TLIF group and only two cases in the OPEN-TLIF group. The reason may be that the learning curve of MIS-TLIF is steep, and the operation space is narrow due to the limitation of the channel. Lee et al. [
21] conducted a large sample size study to evaluate the learning curve of MIS-TLIF. The authors found that only after at least 44 cases of surgery could surgeons truly master the skill, shorten the operation time and reduce the amount of fluoroscopy, and patients could obtain satisfactory clinical efficacy. It is also worth noting that serious complications have occurred due to the surgeon’s familiarity with MIS operations: duodenal rupture occurred in one case and cage loosening occurred in two cases. A study by Kang et al. [
27] counted dural tears in the MIS-TLIF surgery, which occurred in one out of four patients undergoing primary surgery, and in four out of nineteen patients undergoing revision surgery. Goertz et al. [
28] found that the incidence of dural tears was higher in obese patients after MIS-TLF surgery. The results of the above studies indicate that the indications for MIS-TLIF surgery should be strictly controlled, and appropriate cases should be selected to improve the safety of surgery.In this study, there were no complications due to pedicle screw misplacement in either group. However, when the study focused on the accuracy of screw placement, and the position of the screw was evaluated according to Rao classification, the number of B-type screws in the MIS-TLIF group was higher than that in the OPEN-TLIF group (p
29] analyzed the use of CT navigation to guide pedicle screw placement in MIS-TLIF, and the results showed that the screw placement accuracy was 95.3%, and 19 screws (4.7%) deviated into the spinal canal. The authors believed that the narrow space under the channel limited the accuracy of screw placement. The study of Zhao et al. [
30] found that the injury rate of the upper facet during MIS-TLIF was 34.07% (62/182). After logistics regression analysis, the author found that a body mass index over 30 kg/m2 and L5 pedicle screw placement were independent risk factors for facet joint injury.
This study has limitations. First, the number of cases was limited. The incidence of lumbar degenerative diseases of two segments was lower, and the lack of follow-up data for some patients further limited the sample size. Second, the follow-up time was limited. Although all the patients achieved fusion in the follow-up time of this study, the difference in long-term efficacy between the two surgical methods still needs to be observed, and the difference in long-term complications between the two surgical methods still needs to be followed up. Third, this study was a single center retrospective study. The advantages and disadvantages of the two methods should be further compared in future studies with larger sample sizes, longer follow-ups and in multiple centers.



留言 (0)