1. IntroductionSevere acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes Coronavirus Disease 2019 (COVID-19) [
1]. As of 2 September 2022, over 604 million cases of COVID-19 have been documented, with death toll surpassing 6.5 million globally (WHO report). The health and economic toll of COVID-19 will increase over time. Further, the emergence and spread of SARS-CoV-2 variant of concern (VOC) have raised questions about the efficacy of current vaccines and monoclonal antibody therapies [
2].Early manifestations of SARS-CoV-2 infection are protean, but ageusia and anosmia are common [
3]. Other common symptoms include fever, cough, dyspnea, myalgias and/or fatigue [
4]. In severe cases, there may be acute respiratory distress syndrome (ARDS) or even multi-organ failure [
5]. There are increasing reports of some survivors suffering Long COVID [
6], a chronic illness with ongoing multidimensional symptomatology and disability that may last for weeks to years after the initial infection [
7]. The most common symptom associated with Long COVID is asthenia [
8,
9]. The other general symptoms that may be associated with Long COVID are fever, chills, anorexia, and general malaise [
10]. Long COVID may affect multiple organs in the cardiovascular [
11], respiratory [
12], nervous [
13], digestive [
14], urinary [
15], and the reproductive systems [
16]; and thus may result in a varied tissue-specific clinical manifestations.MicroRNAs (miRNAs) are small non-coding RNAs (ncRNA), 19–25 nucleotides in length, derived from hairpin shaped precursor molecules encoded by the genomes of animals, plants, and viruses [
17]. miRNAs control gene expression and regulate a wide array of biological processes by targeting messenger RNAs (mRNA) and inducing translational repression or accelerated RNA degradation [
18]. The miRNA expression profiles are tissue-/cell-specific [
19]. In recent years, miRNAs have been studied as likely candidates involved in most biologic processes; they have been implicated in many human diseases, including COVID-19 [
20]. The circulatory miRNAs present in blood are enclosed in vesicles (exosomes), which protect them from degradation [
21]. The stability of miRNAs in blood, their tissue specificity, and the ease with which they can be quantified make them a viable alternate to serve as a clinical biomarker for a wide range of diseases. We hypothesized that the dynamic changes in the circulatory miRNAs could reflect the severity of COVID-19 and thereby better predict length of hospital stay (LOS) and mortality risk. Our study demonstrates that miR-6741-5p plasma levels could predict LOS of hospital admitted patients by 48 h with high confidence and mortality risk. The study further describes the significance of miR-6741-5p in the biology of COVID-19.Treating COVID-19 and associated respiratory illness can be a major strain on the healthcare and economic systems. Pandemics may result in a sudden increase in demand for inpatient facilities with a corresponding increase in the number of infected cases [
22]. Liquid biomarkers such as miR-6741-5p have the advantage of real-time, non-invasive longitudinal monitoring of a disease condition and heterogeneity over tissue markers [
23]. This is the first study that describes a miRNA with potential to serve as a prognostic biomarker for predicting LOS and mortality risk. Predicting factors (such as circulating miR-6741-5p) associated with the LOS can not only aid in triaging patients in a timely manner but also assist in efficiently treating patients and managing hospitals. 4. DiscussionWe hypothesized circulatory miRNAs to provide predictive significance for the prognosis of COVID-19 patients. There are over 5000 publications that describe circulating miRNAs as biomarkers and 977 publications that describe circulating miRNAs as prognostic biomarkers. Interestingly, there are about 26 publications that describe the role of circulating miRNAs in COVID-19 and only one manuscript describes the cardiovascular signatures of severe COVID-19 that could predict mortality [
31]. The study determined a combination of circulatory miRNAs, inflammatory and endothelial cell biomarkers to serve as predictors of mortality in COVID-19 patients with severe illness.The goal of this study was to determine the minor differences observed in the circulatory miRNA profiles of moderate to severe COVID-19 patients on the day of hospitalization (I) when they received remdesivir plus dexamethasone (with or without baricitinib) treatment and at 48 h post treatment (T). The difference in changes to miRNA profile within 48 h post treatment was assumed to be the net effect of antiviral plus dexamethasone with or without baricitinib treatment. PCA is used to identify strong patterns in large, complex data sets [
32]. It is considered as the initial step in an exploratory analysis on expression data such as miRNA profiles [
33]. This is widely used effectively to reduce a large set of variables into smaller, easier-to-analyze sets while retaining meaningful information [
34]. We found PCA of plasma miRNA profiles could distinguish COVID-19 patients (group I) from healthy volunteers (group C). PCA analysis showed distinct clusters for group C and I (
Figure 1A,C); whereas COVID-19 patients (group I) clustered relatively closer to COVID-19 patients treated for 48 h (group T) (
Figure 1B). Such a cluster pattern between groups I and T is partly because of the shorter time interval post treatment and the inherent variations in the host responses to the treatment. It is evident that the discriminating miRNAs, such as miR-6741-5p, that result from such an analysis may prove to be robust biomarkers.Only nine circulatory miRNAs were differentially expressed between groups I and T compared to groups I and C, and groups T and C (
Figure 1D–F). Of these, only miR-6741-5p was upregulated in COVID-19 patients that were treated (T) (
Figure 2A). We were interested in the expression of miR-6741-5p for two reasons: (i) the significant difference in the expression levels of miR-6741-5p between the three groups of participants (
Figure 2A); and (ii) the putative targets of miR-6741-5p and their possible relevance to COVID-19 biology (
Figure 3).There was a unique pattern of expression in COVID-19 patients who received treatment. SARS-CoV-2 infection as such lowers the expression of miR-6741-5p (
Figure 2A). Upon treatment, in a subset of COVID-19 patients we observed a sudden spike in the miR-6741-5p expression (
Figure 2B) and that was a sign of poor prognosis, or longer LOS (
Table 1). The COVID-19 patients who survived post treatment generally had only a slight or no change in the expression of miR-6741-5p (
Figure 2B). An estimated marginal mean of 12.42 for Log2 CPM (shown as dotted line in
Figure 2B) may serve as a “clinical threshold” that may allow clinicians to determine who may survive (good prognosis) or die (poor prognosis) among COVID-19 patients. More specifically, all patients with below 12.42 Log2 CPM survived, had a short LOS, or a good prognosis (n = 7); whereas all patients with over 12.42 Log2 CPM died, had a long LOS, or a poor prognosis (n = 11). The LOS for all patients are shown in
Table 1. Inflammatory biomarkers such as C-reactive protein (CRP), D-dimer, and ferritin are often elevated in COVID-19 patients [
35]. We did not observe a significant correlation between the levels of inflammatory biomarkers during early times of treatment and the treatment outcome as suggested in earlier studies [
24,
36]. However, medical interventions such as mechanical ventilation and oxygenation seem to have a correlation with the prognosis of the disease. All the individuals who were on ventilation and/or received oxygen for an extended period of time had poor prognosis or died (
Supplemental Table S2). The miR-6741-5p expression in plasma obtained from patients treated with remdesivir plus dexamethasone (with baricitinib) at 48 h post treatment was slightly higher than those treated without baricitinib (12.82 vs. 10.3 log2 CPM). This can be explained by the fact that there are still concerns that JAK inhibitors such as baricitinib may increase the incidence of COVID-19-associated pulmonary aspergillosis (CAPA) when used with corticosteroids [
37].In our recently concluded study [
24], we did not mention miR-6741-5p as the discussion was only on the select miRNAs that were altered ≥10 folds due to SARS-CoV-2 infection. The effects of miR-6741-5p on COVID-19 biology could be multiple based on the potential target genes (
Figure S3). The overall pleiotropic effects of a sudden increase in miR-6741-5p expression in COVID-19 patients seem to lower adaptive immunity, pro-inflammatory response, healing process, cell proliferation and survivability while increasing viral replication; all of which may result in a poor prognosis (
Figure S5) [
38,
39,
40,
41,
42,
43,
44,
45,
46]. It is important to note that the miR-6741-5p expression levels in those with poor prognosis are at comparable levels to what is observed in healthy individuals (
Figure S6). This is a scientific paradox. Herein, we will attempt to solve the paradox using our working hypothetical model as follows: the biological effect of a miRNA is going to be different in a healthy individual compared to an individual who is responding to a viral infection; the biotic milieu is different (
Figure 4). In a healthy naïve individual, an innate immune response is only triggered following an exposure to a pathogen and so there is not going to be an adaptive immune response [
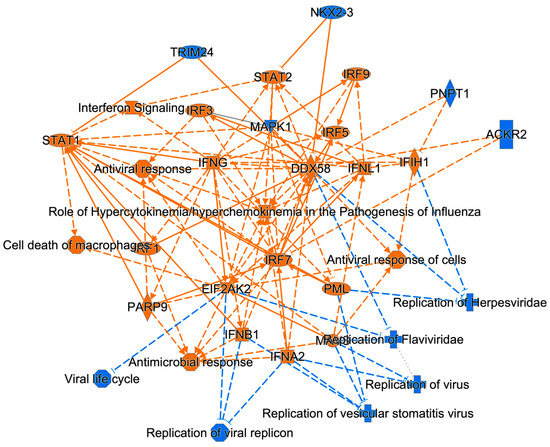
47]. The inflammatory responses and cell proliferation in a healthy individual are at adequate levels. When SARS-CoV-2 infects a person with a good prognosis, there is a decrease in the miR-6741-5p levels that promote an innate immune response followed by a robust specific adaptive immune response to fight the viral pathogen. There is an increase in pro-inflammatory response to combat virus-induced pathology and inflammation, followed by healing process (cell proliferation and survivability). In a subset of few patients where there is a sudden surge in the miR-6741-5p levels (comparable to healthy individuals), the net effect is different as they are affected with an ensuing virus-induced pathology. Such a sudden surge in miR-6741-5p leads to a decrease in adaptive viral specific immunity, pro-inflammatory response, antiviral response, cell proliferation and survivability; and thus a poor prognosis. In this study, we were also able to establish miR-6741-5p to physically bind, interact, and regulate expression of APOBEC3H gene (
Figure 3). Human APOBEC3H has two major functions: DNA cytosine deaminase [
48] and DNA editing enzymatic activity [
49]. The gene ontology (GO) annotations for APOBEC3H are provided in
Table S3. The DNA editing enzyme function of APOBEC3H plays a crucial role in innate and adaptive immune responses to viruses like herpesviruses, retroviruses, and potentially RNA viruses such as SARS-CoV-2 [
39,
42,
50]. The APOBEC3H is regulated by interferons (another key mediator of innate immunity) [
51] and thus may not have a direct bearing in healthy individuals when compared to infected patients. An integrated network and dynamical reasoning assembler (INDRA)-interactive pathway map (INDRA-IPM) [
52] representing the ability APOBEC3H to negatively regulate viral genome is presented in
Figure S7. In a recently concluded study, it was determined that the levels of APOBEC3H were higher in older individuals [
53]. Controneo et al. [
53] concluded the necessity to understand if APOBEC3H isoforms affect prognosis in older COVID-19 patients.




留言 (0)