Study design and participants
A retrospective cohort study was performed at the University Medical Center Utrecht (UMCU), a level-1 trauma center in the Netherlands. The medical ethical committee of the UMCU approved this study and waived the need for consent (protocol number 20-599/C).
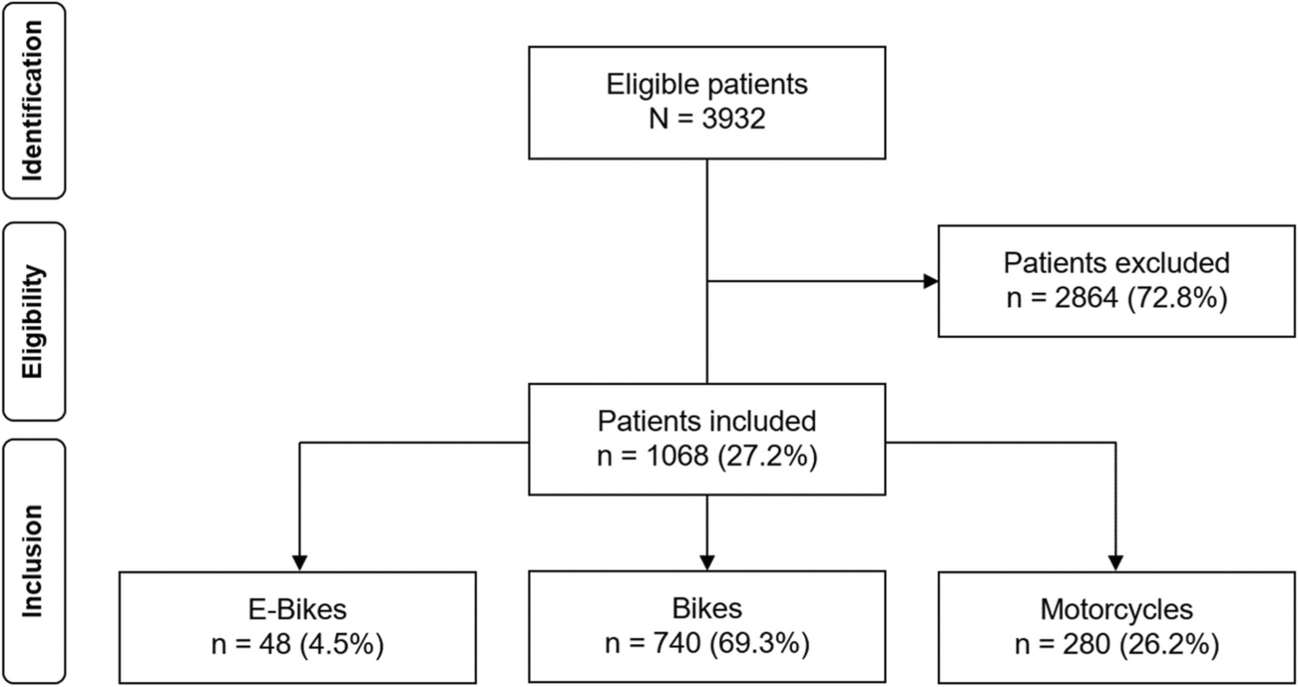
Trauma patients aged 16 years or older and hospitalized between January 1st, 2017, and December 31st, 2017, were identified through the local trauma registry. All consecutive patients who underwent CT imaging of the thorax, abdomen, aorta, thoracic spine, or lumbar spine within seven days of admission were included. At least one of the predefined radiologic parameters had to be assessed on these CT images. Exclusion criteria were an active infection upon admission, active outpatient antibiotic treatment or prophylaxis upon admission, transfer to another hospital during hospital admission, or treatment for more than 24 h in another hospital before transportation to the UMCU. Patients who suffered from severe brain injury—defined as an Abbreviated Injury Scale (AIS) score of the head of 3 or higher—were excluded as well since these injuries almost exclusively determine these patients' prognosis [22, 23].
Radiologic imaging and technique
All CT imaging was routinely performed using either 64- or 256-detector row scanners from Philips Medical Systems (Cleveland, OH, USA). All CT images were viewed using PACS IDS7 21.1.2 (SECTRA), and 0.9 and 5.0-mm slices were available. An intravenous contrast agent was administered in abdominal or thoracic CT imaging during trauma screening or angiographic scans of the aorta. In case an intravenous contrast agent was administered (89.6%, n = 388), the split bolus technique was used to simultaneously assess the portal and the arterial phase.
Radiologic parameter definitions and assessment
Thoracic CT images were analyzed for the presence of coronary artery calcifications and pulmonary emphysema, and abdominal CT images for the presence of calcification in the abdominal aorta and its degree of severity when present.
The coronary arteries and abdominal aorta were assessed on CT images in the bone and soft tissue settings; only calcified plaques were identified. The presence of coronary calcifications was assessed for the left main coronary artery (LM), left anterior descending (LAD) artery, left circumflex (LCx) artery, and right coronary artery (RCA) separately. The extent of calcification of the abdominal aorta was determined based on its circularity and divided per 90 degrees of circularity (i.e., possible scoring of 0 up to 4) as previously described by Hendriks et al. [24]. Pulmonary emphysema was determined using the pulmonary setting and considered present in case centrilobular emphysema was observed. Only centrilobular emphysema was considered in this study, as this specific entity has been associated with smoking, in contrast to other entities that might have more genetic or uncertain etiologies [25].
Two medical doctors (TK, AS) performed the radiologic assessment and discussed borderline cases with a senior staff radiologist with over 13 years of experience in thoracic and abdominal CT imaging evaluation (PdJ). The investigators were blinded to the outcomes during the radiologic analysis. Both investigators and the senior staff radiologist assessed sixty randomly selected cases to evaluate interobserver variability. The results of the interobserver variability analysis were very good, with Cohen's kappas of 0.77 or higher (Supplemental Table 1).
The inclusion criterion was any relevant CT imaging of the chest or abdomen. Therefore, it was unfeasible to assess all radiologic parameters in every patient. For example, when only abdominal imaging was performed, assessment of the coronary arteries was automatically excluded. If one or more radiologic parameters were unavailable, only these parameters were excluded from the analysis, while the available parameters were included. The number of incomplete examinations was stated in the tables as ‘missing’. No imputation methods were performed since we aimed to assess routine CT imaging. The results may be applied easily in patients with routine imaging; imputation methods would not increase the implementation of this opportunistic screening.
Outcomes
The medical health records were screened for outcomes. The primary outcome was the development of one or more complications, cumulated from all separately scored complications: infectious complications treated with antibiotics (i.e., pneumonia, urinary tract infection, wound infection, other infectious complications) and pharmacologically managed delirium (e.g., antipsychotics or benzodiazepines). Diagnosis and treatment of complications were part of regular care; no additional clinical criteria were used.
Secondary outcomes were intensive care unit (ICU) admission, hospital length of stay (HLOS) and ICU length of stay, days on mechanical ventilation, and the discharge condition measured using the Glasgow Outcome Scale (GOS) score. The local trauma registry provided secondary outcomes.
Follow-up lasted until hospital discharge or in-hospital death. No censoring for competing risks was performed; patients that died during hospital stay (1.8%, n = 8) were included in the analyses.
Variables
The local trauma registry provided age, gender, pre-trauma American Society of Anesthesiologists (ASA) classification, Injury Severity Score (ISS), Glasgow Coma Scale (GCS) score, AIS codes, and mechanism of injury. Radiologic images were obtained from the medical records manually.
Statistical analysis
All statistical analyses were performed using RStudio 1.4.1717 for Mac (© The R Foundation for Statistical Computing, 2019) with additional packages. The GOS score was separated into a favorable (i.e., good recovery or light disability) or an adverse discharge condition (i.e., severe disability, persistent vegetative state, or mortality) for further analysis. Coronary calcifications of the LAD, LCx, and RCA were made ordinal into one-, two-, or three-vessel coronary artery calcifications—as inspired by coronary artery disease; the LM was separately considered since it is considered a more severe condition associated with multivessel coronary artery disease [26, 27]. ASA classification was dichotomized into severe (ASA 3–4) or no severe comorbidities (ASA 1–2).
Normally distributed variables were described using the mean and standard deviation (SD), non-normally distributed or ordinal variables using the median and interquartile range (IQR), and categorical variables using the proportions.
The association between radiologic abnormalities and several outcomes—complications, infectious complications, pneumonia, delirium, an adverse discharge condition, and HLOS—was assessed. HLOS was log-transformed before analyses. Results were back-transformed before being presented.
Logistic regression analysis was used for the dichotomous and ordinal outcomes; results were presented with the odds ratio (OR) and 95% confidence interval (95% CI). Linear regression analysis was used for HLOS; results were presented with the beta-coefficient and 95% CI. Regression analyses were performed crude and adjusted for covariates. Age, sex, ASA classification, and ISS were chosen as covariates for each separate radiologic abnormality parameter based on clinical experience and previous literature [10,11,12,13,14,15]. Furthermore, age is a risk factor for the radiologic parameters [16,17,18, 28].
The p for trend was calculated for the number of coronary arteries and the degree of abdominal aorta calcification. In crude analysis, the Cochran-Armitage test was used for dichotomous or ordinal variables; linear regression was used for HLOS. In multivariable analysis, the additional value of the ordinal value to the model was assessed using the likelihood ratio test for all outcomes.
Outcomes were considered statistically significant with a p value < 0.05 despite the number of evaluated associations. No correction for multiple testing was made because of the study's explorative nature.


留言 (0)