
記住我






A 66-year-old Caucasian woman presented with a two-week history of bilateral sequential subacute progressive visual field loss and photopsias initially affecting the left eye and rapidly progressing to the right eye within several days. The patient denied prodromal symptoms and there were no recent infections, no recent travel history or sick contacts. The past medical history was significant for hypothyroidism, migraines, hearing loss and psoriasis. The past surgical history included a bilateral mammoplasty, tubal ligation, and a cone biopsy of the cervix done 40 years ago that revealed pre-cancerous changes. A recent Pap smear was suspicious for malignancy. Attempted repeat biopsy 1 week prior to presentation failed due to scarring of the cervix. Medications included levothyroxine, zopiclone, and an estradiol vaginal ring. The patient had no known drug allergies. The family history was positive for breast cancer. There was no significant past ocular history except for myopia.
On initial ophthalmic examination by the referring physician, best-corrected visual acuity (BCVA) was 20/30 in the right eye and 20/70 in the left eye. Pupils were equal and reactive with no afferent pupillary defect. Confrontation visual fields revealed bilateral enlargement of the blind spots. Color vision was 7/9 in the right eye and 0/9 in the left eye. There were rare anterior chamber cells in both eyes. Intraocular pressures were 17 mmHg bilaterally. Fundus exam revealed normal optic nerve heads with no swelling or vascular engorgement. There was no significant vitritis. Surrounding each disc was a contiguous area of retinal atrophy and retinal pigment epithelium (RPE) disruption bordered by a continuous leading edge of elevated white retina. This bisected the fovea in the left eye and was bordering the fovea in the right eye. An infectious disease workup was initiated. However, due to the proximity of the leading edge to the fovea in the right eye, oral prednisone 100 mg daily was started immediately.
The patient was examined two days later. Despite the large doses of prednisone, BCVA had dropped to 20/400 in the right eye and 20/400 in the left eye. There was again no significant intraocular inflammation. The white line of elevated retina and corresponding area of retinal atrophy had enlarged in both eyes, and had now crossed the fovea in the right eye. Due to the unusual location and pattern, an autoimmune process was suspected. Considering the possible history of gynecological malignancy, arrangements were made for hospital admission and workup.
On initial examination at our institution, the BCVA was 20/500 in the right eye and count-fingers at 1 foot in the left eye. The intraocular pressures were normal. Pupils were 5 mm bilaterally and reactive to light, both direct and consensual. There was no afferent pupillary defect. Color vision was reduced with Ishihara plate testing 1/16 in the right eye and 2/16 in the left eye. Confrontation visual fields were unremarkable. Extraocular movements were normal. Ductions, versions and smooth pursuit were normal. No nystagmus was noted. The anterior segment was normal in both eyes. A grade 2 + nuclear sclerotic cataract was noted in both eyes. The vitreous had no cells and no haze. Fundus examination of the left and right eye showed a classic pattern of symmetrical bilateral retinal atrophy surrounding each optic nerve (Fig. 1). The outer limit of the retinal atrophy showed a distinctive and slightly irregular white border. The area within the atrophic retina showed scattered zones of RPE clumping/migration. The peripheral retinal examination showed no retinal or choroidal lesions, and no vascular changes. The optic nerves appeared normal with no swelling, atrophy or cupping.
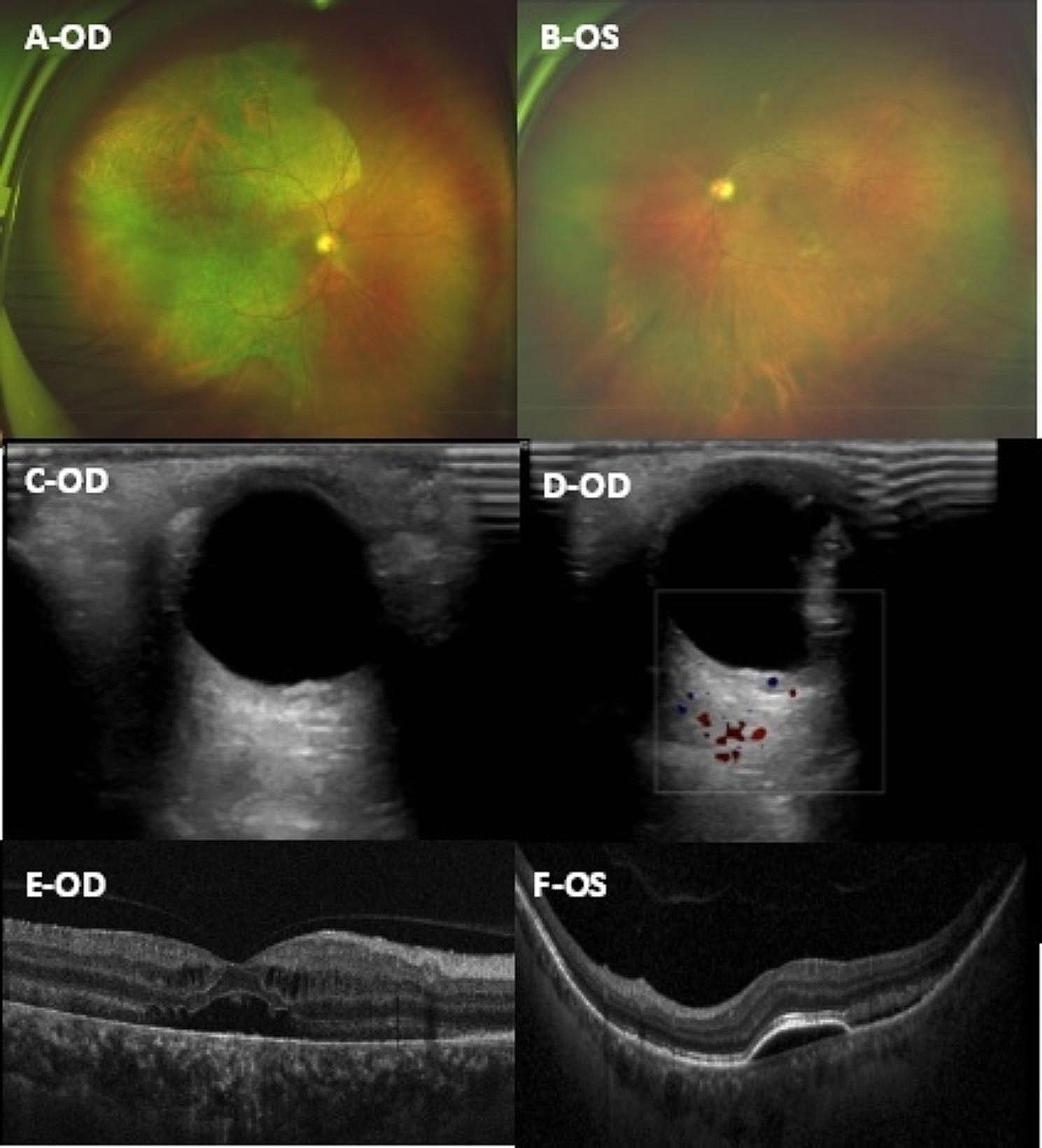
Fig. 1
Fundus examination of the right eye (A) and the left eye (B) showing a classic pattern of symmetrical bilateral retinal atrophy surrounding each optic nerve. The outer limit of the retinal atrophy showed a distinctive and slightly irregular white border
Humphrey visual field testing central 30–2 white stimulus SITA-standard protocol demonstrated symmetrical enlargement of the blind spots with inferior visual field loss corroborating the retinal changes (Fig. 2). Spectral-domain optical coherence tomography (SD-OCT) showed a normal retinal architecture outside the zone of peripapillary atrophy. There was an abrupt and elevated nodular disruption of the RPE at the margin of the annulus, located just beyond the temporal edge of the fovea. Patchy RPE loss and destruction of the ellipsoid layer were seen within the peripapillary atrophied zone extending to the margin of the optic disc (Fig. 3). The structural abnormalities seen on SD-OCT correlated with findings on fundus autofluorescence which showed a classic annular hyperautofluorescent border with presumed active hyperautofluorescent zones with patchy hypoautofluorescent zones of atrophy (Fig. 4).
Fig. 2
Humphrey visual field testing central 30–2 white stimulus SITA-standard protocol demonstrating symmetrical enlargement of the blind spots with inferior visual field loss in the right eye (A) and the left eye (R)
Fig. 3
Spectral-domain OCT of the macular (A) and the optic nerve head (B) of the right eye showing a normal retinal architecture outside the zone of peripapillary atrophy. An abrupt and elevated nodular disruption of the RPE at the margin of the annulus can be seen, located just beyond the temporal edge of the fovea. Patchy RPE loss and destruction of the ellipsoid layer are seen within the peripapillary atrophied zone extending to the margin of the optic disc
Fig. 4
Fundus autofluorescence images of the right and left eye using Topcon 3D OCT-2000 (A and B, respectively) and using Heidelberg Spectralis OCT (C and D, respectively) showing both presumed active hyperautofluorescent zones with patchy hypoautofluorescent zones of atrophy and a classic annular hyperautofluorescent border
Laboratory analyses including erythrocyte sedimentation rate, C-reactive protein, complete blood count with differential, antinuclear antibody, anti-neutrophil cytoplasmic antibodies, rheumatoid factor and angiotensin-converting enzyme revealed normal findings. Human Immunodeficiency Virus (HIV), Herpes Simplex Virus (HSV), Lyme disease (Borrelia burgdorferi), and Bartonella (Cat Scratch Disease) serologies were negative. Varicella Zoster Virus (VZV) immunoglobulin G (IgG) was positive. Toxoplasmosis immunoglobulin G (IgG) and immunoglobulin M (IgM) were nonreactive. An MRI with contrast of the orbits showed no optic nerve pathology.
The patient was started on 1 g IV methylprednisolone for three days followed by oral prednisone 100 mg daily. Two days after presentation, visual acuity was CF at 1 foot in both the right and left eye. There were no changes to the white annular band. Two weeks after presentation, visual acuity declined to HM in the right eye and CF at 1 foot in the left eye. Retinal pigment epithelial atrophy persisted in both eyes and there was no detectable progression of the annular band in both eyes. Three months after presentation, the best-corrected visual acuity was 20/200 in the right eye and CF at 1 foot in the left eye. The annular band remained unchanged in both eyes.
An extensive workup was performed to assess for an occult neoplasm, including Magnetic Resonance Imaging (MRI) scans of the brain, pelvis, spine and breast, and Computed Tomography (CT) scans of the chest, abdomen, pelvis and head. The investigations detected an invasive ductal carcinoma of the left breast that was subsequently confirmed to be of Histological Grade/Nottingham Score of 2/3 following an ultrasound-guided core needle biopsy of the breast.
留言 (0)