
記住我




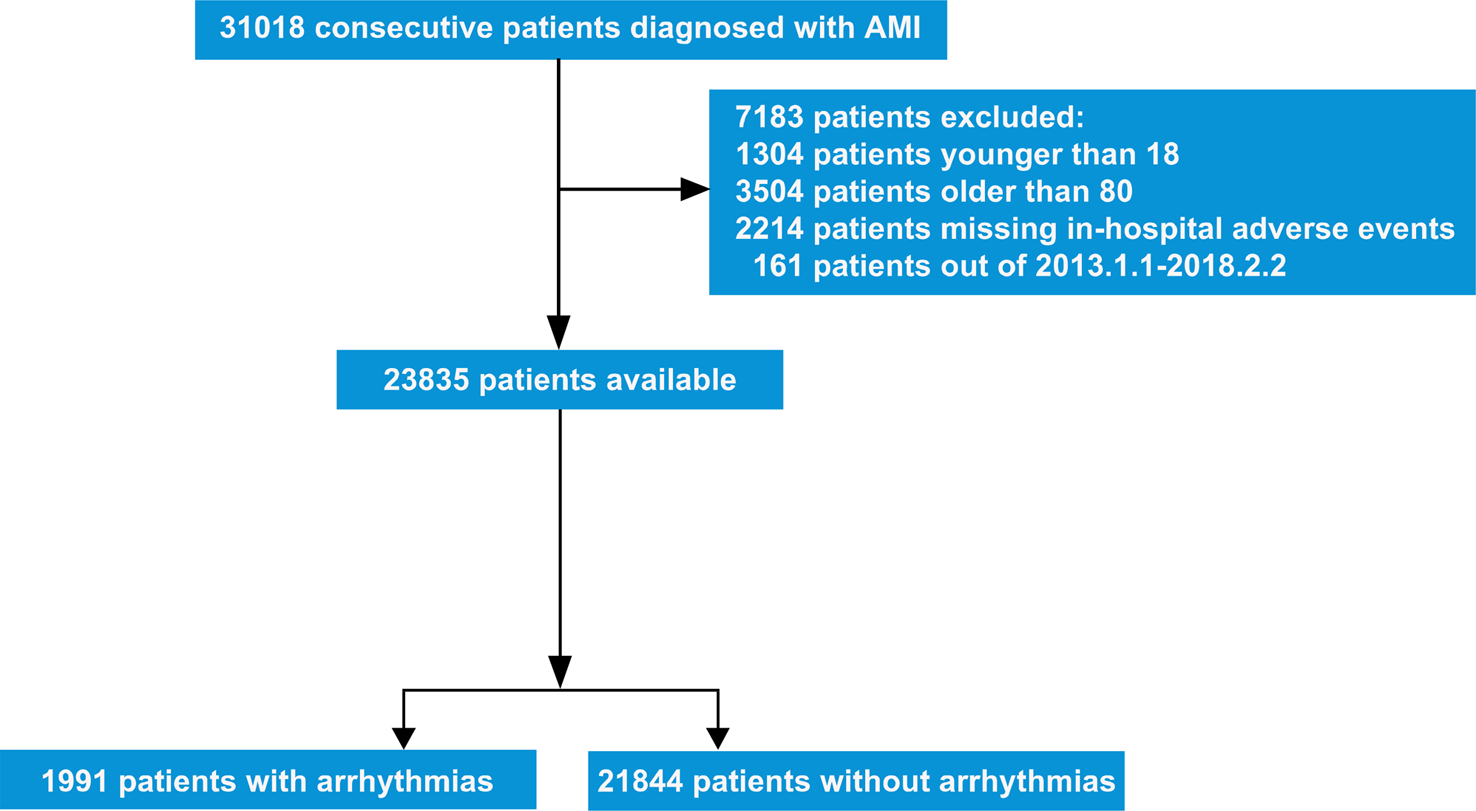




This retrospective cohort study involved patients undergoing CABG from Jiangsu Province Hospital (JSPH) and Shanghai Chest Hospital (SHCH). From the initial 15,600 patients undergoing cardiac surgeries, 5248 patients receiving isolated CABG from the two hospitals were enrolled, including 2241 from JSPH and 3007 from SHCH. Among them, some patients were excluded for the following reasons: 1) age < 75 years old, 2) redo CABG, and 3) severe absence of medical records. Finally, 684 qualified patients were included. The detailed patients’ enrollment was presented in Fig. 1. According to the Chinese Society of Health Management and allied professional organizations recommended criteria with body mass index (BMI), BMI < 18, 18–23.9, 24–27.9 and ≥ 28 indicate lean, normal weight, overweight and obesity, respectively [8] (Fig. 2). Thus, 354 patients were classified into an overweight and obesity group, and the remaining 330 patients were involved into a normal weight and lean group.
Fig. 1
Patients’ enrollment flowchart. CABG coronary artery bypass grafting, JSPH Jiangsu Province Hospital, SHCH Shanghai Chest Hospital
Fig. 2
Different BMI distributions of the whole cohort before and after propensity score matching
This study did not involve patient treatment and ensured patients’ privacy, so individual consent was waived. The procedures conducted here were approved by the ethics committees of Jiangsu Province Hospital (2022SR209) and the ethics committees of the Shanghai Chest Hospital (IS22036). The clinical trial registration number was ChiCTR2200061869 (05/07/2022).
Baseline characteristicsDemographic variables including sex, age, BMI, body surface area, types of coronary artery diseases (CADs), and comorbidities (DM, hypertension, cerebrovascular diseases (CVDs), peripheral vascular disease, preoperative atrial fibrillation, chronic pulmonary disease (COPD), pulmonary hypertension) were collected before operation. Types of CADs included stable angina pectoris, unstable angina pectoris and acute myocardial infarction. CVDs included stroke and lacunar infarction. Scores of the European System for Cardiac Operative Risk Evaluation II (EuroSCORE II) were calculated. Renal failure was defined as Ccr < 30 mL/min/1.73 m2. New York Heart Association (NYHA) grades were used to classify the cardiac function. The short-term postoperative mortality referred to the all-cause death within 30 days after surgery.
Follow-upPatients who survived after the operation were followed up according to the treatment routine. They were followed up at the first month, the third month, and every six months after discharge. If a patient had any change in his/her condition, he/she needed to seek nearby medical treatment in time. During the follow-up, if a patient died, the time and cause of death were recorded timely through family members. The last follow-up results were updated on March 25, 2022. The cardio-cerebrovascular (CCV) mortality included deaths from ischemic heart disease, chronic heart failure, hypertensive disease and cerebrovascular disease. Cerebrovascular disease included ischemic cerebrovascular disease, hemorrhagic cerebrovascular disease and certain complications following cerebrovascular disease. Ischemic heart disease included angina pectoris, myocardial infarction and subsequent complications following myocardial infarction. Hypertensive disease included hypertension and certain complications following hypertension.
Statistical analysisKolmogorov–Smirnov (K–S) test was performed to assess the normal distribution of each variable. Continuous variables in normal distribution were expressed as mean ± standard deviation (SD), and categorical variables were presented as counts with percentages. Non-normally distributed variables were reported as medians and interquartile ranges. Wilcoxon rank-sum test was used for the comparison of continuous variables between 2 groups. Categorical variables were analyzed with Fisher’s exact or Chi-square test.
Clinical variables including age, gender, overweight and obesity, DM, hypertension, types of CADs, serum creatinine (Scr), renal failure, left ventricular ejection fraction (LVEF), COPD, and NYHA grade were estimated by univariate analysis to investigate the relationships with 30-day postoperative mortality. Then variables with P < 0.05 were analyzed by multivariate logistic regression to study the independent risk factors associated with 30-day postoperative mortality. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to present binary outcomes. The Kaplan–Meier method was used to present patients’ survival, with the log-rank test to compare whether there was a significant difference in survival between the two groups. Variables like age, BMI, DM, hypertension, peripheral vascular disease, pulmonary hypertension, CVDs, previous PCI, CABG, male sex, types of CADs, preoperative CCR, COPD, preoperative atrial fibrillation and NYHA grade were taken into multivariate Cox regression to identify significantly different variables for long-term mortality. Hazard ratios (HR) were displayed with 95% CIs. The proportionality of hazards (PH) was assessed for each variable and Schoenfeld residuals were visually inspected for potential time-variant biases.
To minimize the bias of a retrospective observational study, we used 1:1 propensity score matching (PSM) to adjust preoperative variables between the two groups. Each patient with BMI ≥ 24 was matched to a patient with BMI < 24 by using variables: age, CADs classification, hypertension, LVEF, CVDs, pulmonary hypertension, intra-aortic balloon pump (IABP), and Euroscore II score. The optimal nearest neighbor matching algorithm without replacements was applied with the caliper width of 0.02. Cases lack of matched controls were excluded. The validity of PSM was evaluated by standard mean difference (SMD), and the covariate balance was presented with love plot (Additional file 2: Fig. S1). The absolute standardized difference < 0.2 was regarded as balanced matching. Totally 276 pairs of elderly patients were included in this propensity-matched cohort study. Univariate and multivariate logistic regression were applied to analyze the relationships of variates to 30-day postoperative mortality. Kaplan–Meier method and multivariate Cox regression were conducted to present patients’ survival and estimate significantly different variables for long-term mortality. Data processing for PSM and statistical analysis were performed with SPSS 22.0 (IBM, Chicago, IL, USA). P < 0.05 was considered to be significant.
Multi-collinearity diagnosis was performed with SPSS 22.0 (IBM, Chicago, IL, USA). The variance inflation factor (VIF) cutoff point < 10, tolerance > 0.1 and the Condition Index (CI) between 0 and 15 were considered as no collinearity. After collinearity analyzed of DM and overweight and obesity, we found no collinearity existed in these variables before and after PSM.
留言 (0)