
記住我
COVID-19 is a multisystem disease caused by severe acute respiratory syndrome coronavirus 2 and increased demand for ICU (1). Although the number of cases from COVID-19 has stabilized worldwide, it might cause permanent pathology with physical sequelae (2,3). ICU survivors may develop prolonged functional impairment persisting for months or years. Patients with acute respiratory distress syndrome continue to have reduced muscle strength and physical capacity, affecting their full recovery after critical illness (4).
The expectation is that these long-term sequelae will be similar to or worse than those observed in ICU survivors. Since individuals with COVID-19 remain in the ICU for longer, and many COVID-19 pneumonia patient typically require longer durations of mechanical ventilation (MV), high doses of sedatives, vasopressors, and neuromuscular blockers when compared with usual pneumonia (1,5). In addition, corticosteroids are the mainstay of COVID-19 therapy, and the increased rates of secondary infections due to other immunosuppressive therapies, factors that could lead to impaired recovery (5–7). Furthermore, health professionals remain hesitant to mobilize in very critically ill patients’ mobilization in very serious patients, as are most patients with COVID-19 who need intensive care (8). Recent studies have drawn attention to new disabilities and persistent deficits in patients with COVID-19 (9,10). Among the physical alterations, fatigue, muscle weakness, and decreased physical capacity are reported (10,11). Although studies have identified decreased physical capacity at different follow-up times after hospital discharge (9), the acute impact of COVID-19 on the physical function of ICU admittees of different subgroups of recovery still need to be investigated.
Further understanding of the course of physical impairments, the recovery of functionality during hospitalization and its associated factors may help to identify strategies to improve the process of care, disease prevention and rehabilitation of patients affected by COVID-19 during hospitalization and improve their postdischarge outcomes. Therefore, this study aimed to analyze functional recovery subgroups of critically ill COVID-19 survivors during their hospital stay and to identify their associated factors. The secondary aims were to develop predictive models of functional loss at ICU and hospital discharge, identify the factors associated with functional status outcomes for the specific group undergoing MV and observe their ability to perform functional activities.
MATERIALS AND METHODS Design and SettingThis was a prospective multicenter cohort study. Patients were recruited from July 2020 to July 2021. This study was conducted at four hospitals in São Paulo, Brazil: two public and two private. The patients were recruited from the COVID-19 ICUs of those hospitals, and they were followed up until hospital discharge. The procedures were followed in accordance with the ethical standards of the responsible committee on human experimentation (Ethics Committee for Research Project Analysis of the Clinical Hospital USP number 34395020.6.1001.0068) and with the Helsinki Declaration of 1975. All subjects’ informed consent for participation in the study, and all patients or their proxies gave written informed consent.
ParticipantsAll consecutive adult patients (≥ 18 yr old) with COVID-19 diagnosed by reverse transcriptase-quantitative polymerase chain reaction who were admitted to the enrolled ICUs and previously reported their ability to independently perform activities of daily living (defined as a Barthel index [BI] score ≥ 85 2 wk before hospital admission) were included. The exclusion criteria were death during hospitalization, ICU length of stay (LOS) shorter than 4 days, functional decline due to other complications (stroke, amputees) and patients who could not understand simple commands such as opening and closing their eyes, opening their mouth and showing their tongue, and understand the tests to be performed during the evaluation (12).
Assessments Demographic and Clinical Information.Data were collected on demographic and clinical characteristics, including patient age, sex, number of comorbidities, severity of illness (using Simplified Acute Physiology Score [SAPS] 3 (13), use of vasopressors, sedation, corticosteroids and neuromuscular blockers, MV, prone position, dialysis, blood glucose, muscle strength, and ICU LOS. Variables were collected from the patient chart and registered on the Research Electronic Data Capture system.
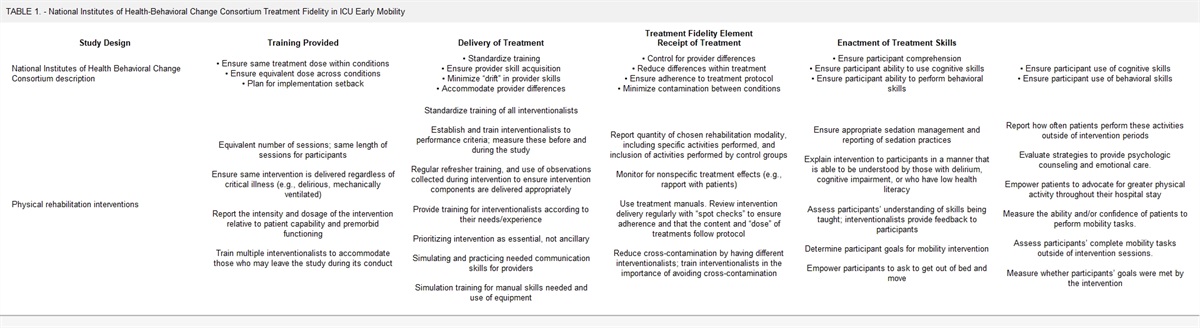
Physical Status.Respiratory muscle strength (12), handgrip dynamometer (13), muscle strength via Medical Research Council (MRC) (14), and step test (15) were performed for physical status evaluation as recommended in the literature. All the tests were always performed in the same order and by trained physical therapists. Patients were monitored and supervised during all tests, and if necessary, oxygen support and rest periods were given before resumption. Respiratory muscle strength evaluation was performed via maximal inspiratory and expiratory pressure tests using a manovacuometer (14). Peripheral muscle strength was evaluated via a handgrip dynamometer (16) and MRC test (15). ICU weakness was considered an MRC score less than 48 points (15). The level of mobility was assessed by the ICU Mobility Scale (17). Physical capacity was assessed by a step test using the number of steps as the performance variable (18). The number of calendar days was counted until out-of-bed patient mobilization (time to out-of-bed patient mobilization) with a high posture. High posture meant sitting on the edge of the bed, standing, and walking (counted from the 2nd day in the ICU for spontaneously breathing patients or after sedatives were withdrawn for patients on invasive MV). Whether the patient walked while in the ICU was also recorded. Patients underwent usual physiotherapy care, including posture changes, active assists and active mobilization, as well as bed positioning, bedside and armchair transfers, orthostatism, and walking, without a preestablished routine. Only one center had a mobility protocol with an established prescription and progression (Supplemental Fig. 1, https://links.lww.com/CCM/H209).
Functional Status.Functional status was evaluated using the BI score (19) assessed by professionals trained to collect research data. The BI evaluates activities of daily living, including mobility items. The BI was analyzed in two ways: as a continuous variable (total score and change between post and pre [delta]) and as a categorical variable (≥ 85 points = functional independence; < 85 points = functional dependence). For the analysis of the BI as a continuous variable, the change in the score from before hospitalization to ICU discharge (delta) was calculated. For the analysis of BI as a categorical variable, patients were classified according to their functional capacity (dependent or independent) (20). The pattern of evolution of each specific BI activity was also separately analyzed during the hospital stay.
Description of Functional Recovery Groups.We analyzed the functional recovery of individuals during all hospitalizations at three points in time: before hospitalization, at ICU discharge, and at hospital discharge. Three functional recovery groups were defined a priori, and then patients were classified as follows: 1) independent individuals who maintained their functional independence (preserved group [PG]) in the ICU and at hospital discharge, 2) individuals who became dependent at ICU discharge but recovered their independence by hospital discharge (recovered group [RG]), and 3) individuals who were dependent at ICU discharge and at the time of hospital discharge (dependent group [DG]). At each time, functional dependence and independence were defined as above (20).
Outcome Measures.The primary outcome was the BI class at ICU discharge and hospital discharge: independent or dependent.
Statistical AnalysisThe data were analyzed for normality using the Kolmogorov-Smirnov test. Continuous variables are presented as the mean and sd or median and interquartile range (25–75th percentile), depending on the data distribution. Categorical data are presented as absolute number and percentage. Missing data were replaced by previously collected data on each patient to maintain the statistical power of the study and decrease the chance of bias. One-way analysis of variance was used to compare the functional recovery groups for continuous variables, the chi-square test for categorical variables. The analyses were performed with SigmaStat 12.0 (Statistical Analysis Software, San Jose, CA).
For Study’s Main Objective.Functional recovery subgroups were classified by the BI score at ICU discharge and hospital discharge. Therefore, if the patient at ICU discharge presented a BI greater than or equal to 85 points, he was classified as maintaining independence (PG). If the patient presented BI less than 85 points, he was classified as dependent. At hospital discharge, if the patient previously classified as dependent in the ICU presented BI greater than or equal to 85 points, he was reclassified as having recovered functionality at hospital discharge (RG). However, if the patient presented BI less than 85 points, he was still classified as dependent (DG).
Multiple linear regressions were used to identify factors associated with decreased BI scores (functionality) on ICU discharge and on hospital discharge. Initially, a univariate analysis was performed using Pearson correlation test between the dependent variable (delta = post–pre BI score) and the independent variables (age, sex, SAPS score, number of comorbidities, presence of hyperglycemia, use of [yes/no]: dialysis and nasoenteral probe and sedation and neuromuscular blocker and corticoid, days under MV, days in the ICU, MRC score in the ICU, time to get out of bed in the ICU) to detect independent variables correlated with the dependent variable. The only exceptions were MRC score and days of hospitalization, which were only tested in the hospital discharge model. The independent variables that correlated with the dependent variable at p value of less than 0.05 were tested in the regression model. Multicollinearity analysis was performed between the independent variables. In the final analysis, the independent variables that showed a true association (p < 0.05) with the dependent variable were kept in the regression model. As the main objective was to analyze the factors associated with functional dependence or independence, the BI score was also treated as a categorical variable to provide information on the functional evolution of the patient.
Multiple binary logistic regression was used to identify factors associated with the presence of functional independence at ICU discharge and functional recovery at hospital discharge. The steps for building the regression models were similar to those for multiple linear regression. However, the univariate analysis was performed via binary logistic regression between the dependent variable (with vs without functional independence) and the independent variables already mentioned in the construction of the multiple linear regression model. The model was adjusted for severity using SAPS score. In the final multiple logistic regression model, the odds ratio (OR) and its 95% CI were established for each variable.
For Study’s Secondary Objectives.All steps of the regression models were repeated only for patients undergoing invasive MV, considering the same dependent and independent variables. To discriminate specific activity changes in the BI during the hospital stay, the percentage of patients who reached the maximum possible score in each of the BI-specific activities at ICU discharge and hospital discharge was determined.
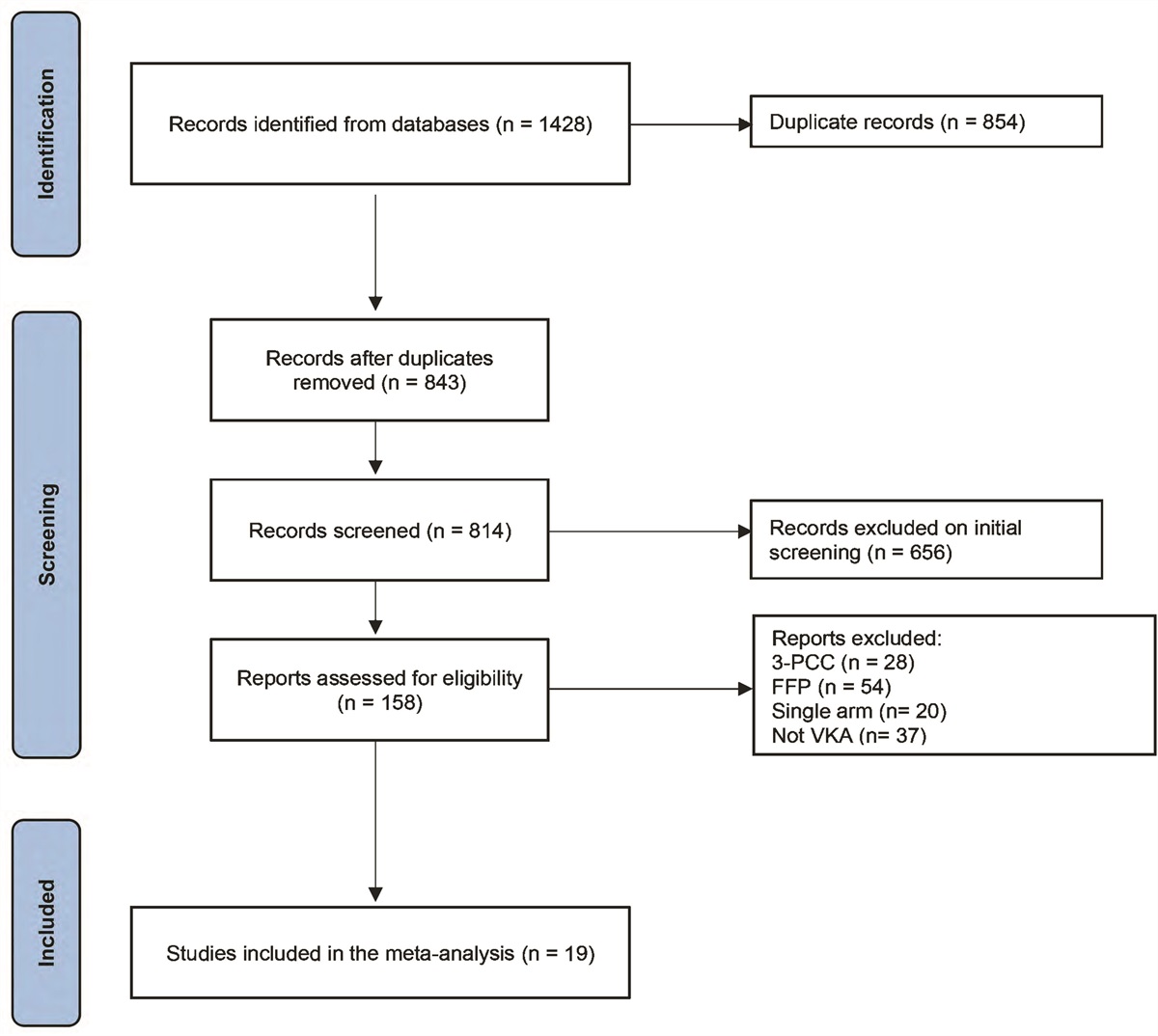
RESULTSFrom the 400 eligible individuals, 339 were included in the study. The reasons for exclusion are shown in Figure 1. The average age was 55 ± 14 years, and 53% of the patients underwent MV for an average of 9 days. Regarding drugs, 93% received corticoids, and 35% received neuromuscular blockers. About the pre-hospital functional status, all patients were independent with BI = 100 points. All demographic, clinical, and therapeutic data for the population are shown in Table 1. The physical and functional characteristics of the general population at ICU discharge and hospital discharge are shown in Supplemental Table 1 (https://links.lww.com/CCM/H209). On the level of physical therapy during the first day of hospitalization, 66% of patients walked during their stay in the ICU. The active exit from bed took, on average, 5 ± 3 days to happen. The highest level of functional mobility of patients at ICU discharge was measured by the 10-point ICU Mobility Scale 7 ± 2 scale.
TABLE 1. - Baseline and Comparison of Demographic, Clinical, Therapeutic, Physical Function, and Functionality Data Among Critically Ill COVID-19 Patients and From the Three Functional Recovery Subgroups Variables n = 339 Preserved Group (n = 144) Recovery Group (n = 109) Dependent Group (n = 75) p Age 55.3 ± 14.7 56 (42–67) 60 (46–67) 59 (48–68) 0.48 Simplified Acute Physiology Score 3 51.2 ± 16.5 52 ± 16 45 ± 17 53 ± 15 0.003 Comorbidities (score) 1.6 ± 0.8 1.64 1.63 1.57 0.8 Use of MV 179 (52.8%) 84 (56%) 35 (48%) 59 (52%) 0.5 MV duration, d 9.3 ± 8.2 5 (3–7.5) 9 (6–15) 6 (4.5–10) < 0.05 Sedation drugs use 189 (55.8%) 59 (39) 47 (63) 83 (72) < 0.001 Sedation duration, d 7.4 ± 6.0 4 (2–6) 7 (5–12) 6 (4–9) < 0.05 Corticosteroids use, n (%) 318 (93.8%) 144 (95) 69 (93) 105 (92) 0.5 Prone position 114 (33%) 49 (33) 28 (39) 35 (31) 0.49 Neuromuscular blocker agent duration, d 120 (35.4%) 2 (1–4) 3 (2–6) 3 (2–4) 0.05 Dialysis, n (%) 38 (11.2%) 10 (7) 7 (6) 18 (24) < 0.001 Nasoenteral probe, n (%) 172 (50%) 52 (36) 59 (54) 57 (76) < 0.001 Hyperglycemia (glucose ≥ 180), n (%) 191 (56.3%) 63 (43) 81 (74) 42 (56) < 0.001 ICU LOS, d 13.9 ± 11.2 11 (7–16) 10 (7–15) 10 (7–17) 0.97 Hospital LOS, d 25.6 ± 23.0 20 (14–30) 19 (13–26) 20 (12–30) 0.66 BI at ICU discharge — 85 (85–100) 65 (55–100) 50 (60–70) 0.02 Handgrip ICU discharge — 22 (18–30) 20 (14–28) 12 (4–18) < 0.05 ICU-acquired weakness — 10 (9.5) 22 (21) 73 (69) < 0.001 MRC at ICU discharge — 52 (46–60) 48 (46–60) 48 (44–60) 0.32 Walking at ICU, n (%) — 131 (86) 47 (63) 44 (38) < 0.001 MIP at ICU discharge — 70 (60–100) 50 (40–70) 55 (49–77) < 0.05 MEP at ICU discharge — 80 (60–100) 60 (40–80) 60 (50–80) < 0.05 BI at hospital discharge — 100 (100–100) 90 (90–100) 60 (55–75) < 0.001 Handgrip at HD — 25 (18–32) 25 (16–32) 18 (15–17) < 0.05 MRC score at HD — 60 (52–60) 58 (48–60) 50 (40–51) 0.002 MIP at hospital discharge — 80 (66–100) 70 (50–100) 70 (61–83) < 0.05 MEP at hospital discharge — 90 (70–100) 80 (50–100) 80 (60–90) < 0.05BI = Barthel index, HD = hospital discharge, LOS = length of stay, MEP = maximal expiratory pressure (cm H2O), MIP = maximal inspiratory pressure (cm H2O), MRC = Medical Research Council, MV = invasive mechanical ventilation, n = absolute number.
Data are mean ± sd, n, and median (interquartile range). Dashes indicate data not applicable.
 Figure 1.:
Figure 1.: Flowchart of study participants. BI = Barthel index, DC = discharge, LOS = length of stay.
Functional Recovery SubgroupsFrom the 339 patients assessed at ICU discharge, 151 (45%) were independent and 188 were dependent (55%). At hospital discharge, a total of 328 individuals were assessed. Of these, 253 (76.9%) were independent and 75 (22.8%) were dependent. These patients completed the assessments at all three timepoints and were analyzed for functional recovery.
The 328 individuals were classified into three categories according to their BI scores at ICU discharge and hospital discharge. Group PG consisted of 144 patients (44%) who had no functional status loss during hospitalization. The RG group was the 109 (33.2%) individuals who showed dependence at ICU discharge but recovered their independence by hospital discharge. Finally, 75 individuals were dependent at ICU discharge and had not recovered their functional status at hospital discharge (DG) (22.8%). The functional recovery of the patients during hospitalization is shown in Figure 2.
 Figure 2.:
Figure 2.: Functional recovery subgroups based on the Barthel index over the hospital stay of critically ill COVID-19 survivors. DC = discharge, DG = dependent group, IQR = interquartile range, MG = maintenance group, NRG = no recovery group, PG = preserved group, RG = recovery group.
The differences in the physical variables between groups are shown in Table 1. The comparison of demographic, clinical, and therapeutic data between the three functional recovery subgroups is presented in Table 1. Differences were found between the groups in functional severity scored via SAPS 3, MV duration, use and days of sedation, dialysis, nasoenteral probe (yes/no), and hyperglycemia.
Factors Associated With Functional Loss and Recovery Groups During HospitalizationThe primary analyses showed the factors associated with losing some degree of functionality (delta of BI) and the categorization depending on functionality. In the multiple linear regression, age, corticoid use, time to out-of-bed patient mobilization, and hyperglycemia were factors independently associated with some degree of functionality (delta BI score) at ICU discharge. The following equation was built with the associated factors (R2 = 0.26): delta BI = –7.255–(0.262 × age) + (14.692 × corticoid use)–(9.602 × hyperglycemia)–(0.631 × time to out-of-bed mobilization).
The factors associated with becoming functionally dependent at ICU discharge were the time until the first day to out-of-bed patient mobilization (OR, 1.20; 95% CI, 1.11–1.29), age (OR, 1.02; 95% CI, 1.01–1.04), hyperglycemia (OR, 2.52; 95% CI, 1.56–4.07), and SAPS (OR, 1.022; 95% CI, 1.006–1.037). Recovery to baseline independence during the ward stay was associated with ICU LOS (OR, 0.966; 95% CI, 0.939–0.994) and muscle strength (MRC test) at ICU discharge (OR, 1.128; 95% CI, 1.075–1.183). All data are shown in Table 2. In the subgroup analysis of MV patients, the factors associated with becoming functionally dependent at ICU discharge were the time to out-of-bed patient mobilization (OR, 1.11; 95% CI, 1.06–1.24) and days of sedation use (OR, 1.14; 95% CI, 1.03–1.27).
TABLE 2. - Analysis of Variables Associated With Functional Status at Different Points of Physical Function Recovery Variable OR (95% CI) For dependence functional at ICU discharge Time to out-of-bed patient mobilization 1.20 (1.11–1.29) Hyperglycemia 2.52 (1.56–4.07) Simplified Acute Physiology Score 1.022 (1.006–1.037) Age 1.02 (1.01–1.04) Recovered baseline independence at hospital discharge ICU length of stay 0.996 (0.939–0.994) Muscle strength (Medical Research Council score) at ICU discharge 1.128 (1.075–1.183)Supplemental Figure 2 (https://links.lww.com/CCM/H209) shows the percentages of patients who reached the maximum possible score in each of the BI-specific activities at ICU discharge and at hospital discharge. The activities that require the highest mobility levels were the ones with the fewest patients who reached the maximum score at each time point. Approximately 60% of patients were completely able to perform postural transfers, climb stairs, and walk at hospital discharge, while almost all patients achieved the maximum scores on bowel control.
DISCUSSIONThis study aimed to characterize and analyze the data from the functional recovery of critically ill COVID-19 patients throughout their hospital stay and identify the associated factors. We analyzed the factors associated with patients who lost function during the ICU stay but recovered it by the time of hospital discharge and patients who lost physical function in the ICU and had not recovered it by the time of hospital discharge. The associated factors for functional loss and dependent status at ICU discharge were age, hyperglycemia, severity, and time to out-of-bed mobilization. The variables associated with physical function recovery on the ward before hospital discharge were ICU LOS and muscle strength at ICU discharge.
A study of the functional trajectory of older adult patients during hospitalization showed that 18% lost function and failed to recover before hospital discharge (21). Herridge et al (22) found that different patterns of the trajectory of functional recovery after ICU discharge were predicted by age and ICU LOS. Patients who failed to recover functionally consisted of older patients with longer sedation and longer hospital stays (23). Several studies have shown physical changes after infection by COVID-19 and have called attention to its greater impact on those patients who need to be hospitalized (9,11,24,25). Our data showed the percentage of patients with COVID-19 who did not recover their previous functional state and who may need post-hospital interventions. We found age, hyperglycemia, severity, corticoid use, and sedation to be independent factors for functional loss in this specific population. Muscle strength at ICU discharge was associated with functional recovery at hospital discharge. Clinical variables such as age and muscle strength have been associated with functional loss in hospitalized patients (26,27), and recent studies have added data of patients with COVID-19. de Andrade-Junior et al (28) showed muscle alterations in patients with COVID-19. A previous study showed a relationship between loss of strength in the ICU and worse functional outcomes after discharge in patients with COVID-19 (25). In our study, muscle strength was also related to the functional recovery group at discharge from the ward. In the study by McWilliams et al (29), all COVID-19 patients developed muscle weakness in the ICU, and older patients were more likely to require further rehabilitation after discharge. Age was also associated with physical function in COVID-19 patients in the study by Paneroni et al (30), as was the use of MV. Hyperglycemia and corticosteroids are known factors for worse physical outcomes due to their negative impact on muscles. Blood glucose control and rational use of corticosteroids have been suggested for the prevention of the physical components of post-intensive care syndrome and better recovery after discharge from the ICU (15,31). However, even we know that steroids can cause ICU-related myopathy, they are an evidence-based treatment regime for COVID-19 and hence cannot be avoided (7). Therefore, the modifiable factors showed in our study and other studies associated with functional loss would be hyperglycemia and muscle strength. In the subanalysis of patients who used MV, days of sedation were associated with lost physical function, although it did not necessarily lead to functional dependence. Sedation has been widely recognized as a modifiable factor to minimize negative outcomes (32).
As several studies have shown benefits from early rehabilitation in the ICU (33,34), we chose to analyze the impact of adding motor milestones at independence status to the clinical variables. This is particularly important because rehabilitation is a modifiable variable that can help improve outcomes. In patients with COVID-19, we found that a longer time to getting out of bed was associated with independence loss. Most likely, this is because a longer time spent in bed has adverse consequences (35). When analyzing the specific activities of the BI, we noted that the activities that imply mobility were more severely impaired at hospital discharge. This may be an opportunity to focus on physical therapy rehabilitation in hospital follow-up to improve the functionality of these patients (36).
This study has some strengths and limitations. This was a multicentric study with longitudinal follow-up of patients during their hospital stay. This allowed us to analyze the functional recovery and associated factors at different times. To the best of our knowledge, this is the first study to classify functional recoveries during hospitalization in patients with COVID-19. Despite being multicentric, it was carried out in a single state in Brazil, São Paulo though it should be noted, São Paulo is the most populous Brazilian state, and it was the epicenter of COVID-19 for several months. Since this was a longitudinal study, practices of ventilatory support, medications, and disease severity were altered during the time of the pandemic. These changes may have affected the rehabilitation of these patients over the study time. Additionally, we did not separately analyze data from the private and public hospitals, the impact of established mobility protocols in the hospitals, the physiotherapist/patient ratio or the number or duration of physical therapy sessions in the ICU or ward, which would have bolstered our results. Symptoms of distress could occur during ICU stay, especially during the pandemic. This can impact patients’ mobility level due to factors such as demotivation, fear, and adherence to the rehabilitation process. And the subsequent impact on functional recovery. This was not evaluated in our study. Finally, the present study does not present control groups. The assessments were carried out at the pandemic’s peak when all ICUs were directed toward caring for patients with COVID-19.
Analyzing the variables associated with functional recovery may help to refine the rehabilitation throughout the care of COVID-19 patients and potentially reduce the number of patients with physical function impairment. Second, attention should be paid to patients who lose their function in the ICU and recover it before going home (36). For the management of hospitals, more data are needed to help create protocols for intervention against modifiable factors and the rehabilitation of patients. Our data can help health systems implement public policies for critically ill COVID-19 patients’ rehabilitation. Further examination of these groups may assist in the design of clinical trials to tailor interventions to specific subgroups of COVID-19 individuals who fall critically ill.
CONCLUSIONSMore than half of critically ill patients with COVID-19 became physically dependent after their ICU stay, and age, hyperglycemia, and time to out-of-bed patient mobilization were independent factors associated. About the patients that recovered their physical function by hospital discharge, the variables associated with recovery were muscle strength at ICU discharge and ICU LOS.
REFERENCES 1. Wiersinga WJ, Rhodes A, Cheng AC, et al.: Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA. 2020; 324:782–793 2. Falvey JR, Ferrante LE: Flattening the disability curve: Rehabilitation and recovery after COVID-19 infection. Heart Lung. 2020; 49:440–441 3. Grabowski DC, Joynt Maddox KE: Postacute care preparedness for COVID-19: Thinking ahead. JAMA. 2020; 323:2007–2008 4. Herridge MS, Tansey CM, Matté A, et al.; Canadian Critical Care Trials Group: Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011; 364:1293–1304 5. Grasselli G, Zangrillo A, Zanella A, et al.; COVID-19 Lombardy ICU Network: Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUS of the Lombardy region, Italy. JAMA. 2020; 323:1574–1581 6. Oliveira E, Parikh A, Lopez-Ruiz A, et al.: ICU outcomes and survival in patients with severe COVID-19 in the largest health care system in central Florida. PLoS One. 2021; 16:e0249038 7. Sterne JAC, Murthy S, Diaz JV, et al.: Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: A meta-analysis. JAMA. 2020; 324:1330–1341 8. Liu K, Nakamura K, Kudchadkar SR, et al.: Mobilization and rehabilitation practice in ICUS during the Covid-19 pandemic. J Intensive Care Med. 2022; 37:1256–1264 9. Hodgson CL, Higgins AM, Bailey MJ, et al.; COVID-Recovery Study Investigators and the ANZICS Clinical Trials Group: The impact of COVID-19 critical illness on new disability, functional outcomes and return to work at 6 months: A prospective cohort study. Crit Care. 2021; 25:382 10. Gamberini L, Mazzoli CA, Sintonen H, et al.; ICU-RER COVID-19 Collaboration: Quality of life of COVID-19 critically ill survivors after ICU discharge: 90 days follow-up. Qual Life Res. 2021; 30:2805–2817 11. Nalbandian A, Sehgal K, Gupta A, et al.: Post-acute COVID-19 syndrome. Nat Med. 2021; 27:601–615 12. De Jonghe B, Sharshar T, Lefaucheur JP, et al.; Groupe de Réflexion et d’Etude des Neuromyopathies en Réanimation: Paresis acquired in the intensive care unit: A prospective multicenter study. JAMA. 2002; 288:2859–2867 13. Moreno RP, Metnitz PG, Almeida E, et al.; SAPS 3 Investigators: SAPS 3–From evaluation of the patient to evaluation of the intensive care unit. Part 2: Development of a prognostic model for hospital mortality at ICU admission. Intensive Care Med. 2005; 31:1345–1355 14. McConnell AK, Copestake AJ: Maximum static respiratory pressures in healthy elderly men and women: Issues of reproducibility and interpretation. Respiration. 1999; 66:251–258 15. Vanhorebeek I, Latronico N, Van den Berghe G: ICU-acquired weakness. Intensive Care Med. 2020; 46:637–653 16. Luna-Heredia E, Martín-Peña G, Ruiz-Galiana J: Handgrip dynamometry in healthy adults. Clin Nutr. 2005; 24:250–258 17. Kawaguchi YM, Nawa RK, Figueiredo TB, et al.: Perme intensive care unit mobility score and ICU mobility scale: Translation into Portuguese and cross-cultural adaptation for use in Brazil. J Bras Pneumol. 2016; 42:429–434 18. Andrade CH, Cianci RG, Malaguti C, et al.: The use of step tests for the assessment of exercise capacity in healthy subjects and in patients with chronic lung disease. J Bras Pneumol. 2012; 38:116–124 19. Mahoney FI, Barthel DW: Functional evaluation: The Barthel index. Md State Med J. 1965; 14:61–65 20. Sulter G, Steen C, De Keyser J: Use of the Barthel index and modified Rankin scale in acute stroke trials. Stroke. 1999; 30:1538–1541 21. Covinsky KE, Palmer RM, Fortinsky RH, et al.: Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: Increased vulnerability with age. J Am Geriatr Soc. 2003; 51:451–458 22. Herridge MS, Chu LM, Matte A, et al.; RECOVER Program Investigators (Phase 1: towards RECOVER); Canadian Critical Care Trials Group: The RECOVER program: Disability risk groups and 1-year outcome after 7 or more days of mechanical ventilation. Am J Respir Crit Care Med. 2016; 194:831–844 23. Gandotra S, Lovato J, Case D, et al.: Physical function trajectories in survivors of acute respiratory failure. Ann Am Thorac Soc. 2019; 16:471–477 24. Stam HJ, Stucki G, Bickenbach J; European Academy of Rehabilitation Medicine: COVID-19 and post intensive care syndrome: A call for action. J Rehabil Med. 2020; 52:jrm00044 25. Medrinal C, Prieur G, Bonnevie T, et al.: Muscle weakness, functional capacities and recovery for Covid-19 ICU survivors. BMC Anesthesiol. 2021; 21:64 26. Aarden JJ, van der Schaaf M, van der Esch M, et al.; Hospital-ADL study group: Muscle strength is longitudinally associated with mobility among older adults after acute hospitalization: The Hospital-ADL study. PLoS One. 2019; 14:e0219041 27. Dettling-Ihnenfeldt DS, Wieske L, Horn J, et al.: Functional recovery in patients with and without intensive care unit-acquired weakness. Am J Phys Med Rehabil. 2017; 96:236–242 28. de Andrade-Junior MC, de Salles ICD, de Brito CMM, et al.: Skeletal muscle wasting and function impairment in intensive care patients with severe Covid-19. Front Physiol. 2021; 12:640973 29. McWilliams D, Weblin J, Hodson J, et al.: Rehabilitation levels in patients with Covid-19 admitted to intensive care requiring invasive ventilation. An observational study. Ann Am Thorac Soc. 2021; 18:122–129 30. Paneroni M, Vogiatzis I, Bertacchini L, et al.: Predictors of low physical function in patients with Covid-19 with acute respiratory failure admitted to a subacute unit. Arch Phys Med Rehabil. 2021; 102:1228–1231 31. Bryant SE, McNabb K: Postintensive care syndrome. Crit Care Nurs Clin North Am. 2019; 31:507–516 32. Pun BT, Balas MC, Barnes-Daly MA, et al.: Caring for critically ill patients with the ABCDEF bundle: Results of the ICU liberation collaborative in over 15,000 adults. Crit Care Med. 2019; 47:3–14 33. Schujmann DS, Teixeira Gomes T, Lunardi AC, et al.: Impact of a progressive mobility program on the functional status, respiratory, and muscular systems of ICU patients: A randomized and controlled trial. Crit Care Med. 2020; 48:491–497 34. Schweickert WD, Pohlman MC, Pohlman AS, et al.: Early physical and occupational therapy in mechanically ventilated, critically ill patients: A randomised controlled trial. Lancet. 2009; 373:1874–1882 35. Winkelman C: Bed rest in health and critical illness: A body systems approach. AACN Adv Crit Care. 2009; 20:254–266 36. Pandullo SM, Spilman SK, Smith JA, et al.: Time for critically ill patients to regain mobility after early mobilization in the intensive care unit and transition to a general inpatient floor. J Crit Care. 2015; 30:1238–1242
留言 (0)