
記住我
KEY POINTS
Question: We assessed the efficacy and safety of avdoralimab (complement blockade with an anti-C5aR1 mAb) in patients with severe COVID-19. Findings: In this double-blind, placebo-controlled study, C5aR1 blockade in severe COVID-19 did not improve clinical status at days 14 and 28. Meaning: These results do not support further evaluations of complement blockade for severe COVID-19 treatment in the context of actual standard-of-care.Since its emergence in China in 2019, the original strain of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and its variants have infected ~260 million people globally, and over 5 million people worldwide had died from COVID-19 by the end of 2021 (1). With the progression of the pandemic, very few treatment options have proved effective, and COVID-19 continues to be a major public health problem. In 10–20% of hospitalized patients, transfer to an ICU is required, due to acute respiratory distress syndrome, requiring high-flow oxygen (HFO), noninvasive ventilation (NIV), or invasive mechanical ventilation (IMV) (2,3). Severe COVID-19 is characterized by overt inflammation of the lungs in response to the viral infection (4–6). No antiviral treatment has yet displayed strong clinical efficacy (7). Immunomodulatory drugs known to delay hyperinflammation—principally dexamethasone (8), but also, to a lesser extent, tocilizumab (9,10), anakinra (11), and Janus Kinase (JAK) inhibitors (12,13)—have been shown to be effective, to some extent. However, despite substantial changes to the treatments prescribed, no significant improvements in ICU mortality rates between the first wave and the next two waves have been reported (14).
A link between exaggerated activation of the complement cascade and the initiation, maintenance, and amplification of inflammation has been reported in severe COVID-19 (15–17). Furthermore, systemic activation of the complement cascade may, indeed, lead, via C5a, to the recruitment of neutrophils to the pulmonary endothelium and their activation, resulting in endothelial cell damage and subsequent lung injury (18,19). Consistent with these results, we reported an association of higher levels of soluble C5a with more severe COVID-19 in a longitudinal study assessing the immune responses of 82 individuals (20). We also found that C5b9 accumulated in the lung sections of patients with COVID-19. Accordingly, small proof-of-concept studies have suggested that inhibiting the C5a-C5aR axis might improve survival and reduce hypoxia in patients with severe COVID-19 (21,22).
Avdoralimab is a monoclonal antibody against C5aR1 that inhibits the signaling of C5a via its receptor. In FOR COVID Elimination (FORCE), a double-blind, randomized, placebo-controlled study, we evaluated the safety and efficacy of avdoralimab in patients with severe COVID-19 pneumonia defined as a requirement for oxygen therapy greater than or equal to 5 L/min to maintain blood oxygen saturation levels (Spo2) greater than 93%.
MATERIALS AND METHODS Trial OversightFORCE was a double-blind, placebo-controlled phase II clinical trial conducted at 12 clinical sites in France (full list in the Supplementary Appendix, https://links.lww.com/CCM/H213), and coordinated by Assistance Publique des Hôpitaux de Marseille. The trial protocol was approved by the French National Agency for the Safety of Medicines and Health Products (MEDAECNAT-2020-04-00043_2020-001686-36), and the competent ethics committee (Comité de Protection des Personnes Ouest II CPP #2020/34/Covid-19, EudraCT2020-001686-36) and was overseen by an independent data and safety monitoring board. Procedures were performed in accordance with ethical standards (institutional and national) for human experimentation and the 1975 Helsinki Declaration. Data were analyzed by independent statisticians at the International Drug Development Institute. Written informed consent was obtained from all patients or their legal representatives (if the patient was unable to provide consent). The trial was registered on ClinicalTrials.gov (NCT04371367).
Trial PopulationWe enrolled adults between 18 and 80 years old in this trial. Hospitalized patients were eligible for inclusion if they had severe COVID-19 pneumonia requiring oxygen therapy greater than or equal to 5 L/min to maintain blood Spo2 greater than 93% (World Health Organization [WHO] ordinal scale ≥ 5; Table S1, https://links.lww.com/CCM/H213). COVID-19 diagnosis was confirmed by a positive reverse transcription-polymerase chain reaction (PCR) assay for SARS-CoV-2, or, for cohort 2, on the basis of CT imaging findings typical of COVID-19 (peripheral ground glass opacities).
Cohort 1 consisted of patients requiring conventional oxygen therapy via masks or nasal prongs at greater than or equal to 5 L/min (WHO score 5) and patients on HFO (WHO score 6). Cohort 2 contained patients in the ICU requiring HFO, NIV, or IMV (WHO scores, 6–9). Cohort 3 contained patients on IMV for less than 72 hours, with a ratio of the Po2 to the Fio2 (Pao2/Fio2 [P/F]) of 60 to 200 mm Hg (WHO scores, 7–9).
Initially, the trial was designed to include two cohorts. Cohort 1 consisted of patients admitted to a general hospital and requiring conventional oxygen therapy via masks or nasal prongs at greater than or equal to 5 L/min (WHO score, 5), and cohort 2 contained patients admitted to the ICU requiring HFO, NIV, or IMV (WHO scores, 6–9). In the face of difficulties enrolling patients in cohort 1 (due to patients requiring rapid transfer to the ICU for HFO treatment), the trial was amended without breaking blinding in August 2020. In this new design, once cohort 2 was closed for enrollment, patients receiving HFO were enrolled in cohort 1 (WHO scores, 5–6). Patients on IMV for less than 72 hours with a Pao2/Fio2 ratio of 60 to 200 mm Hg were enrolled in cohort 3 (WHO scores, 7–9).
For all cohorts, the exclusion criteria included being pregnant or breastfeeding, being enrolled in another clinical trial, having active bacterial or fungal sepsis at the time of enrollment, or having contraindications preventing ICU admission. After trial amendment, for cohorts 1 and 3, the exclusion criteria included receiving extracorporeal membrane oxygenation, having chronic pulmonary disease, or requiring immediate renal support therapy. Patients were allowed to receive glucocorticoids, including dexamethasone (12). However, concomitant therapy with immunomodulatory or antiviral agents (such as tocilizumab, anakinra, or hydroxychloroquine) was prohibited. The use of antibiotic prophylaxis was not specifically recommended.
Randomization and TreatmentEligible patients were randomly assigned, in a 1:1 ratio, to the avdoralimab or placebo arms, via a web-based case-report form system. Randomization was performed in blocks of four, with stratification by trial site and type of admission (ICU or general hospital). Patients received avdoralimab (500-mg loading dose followed by a 200-mg maintenance dose) or placebo (normal saline) administered intravenously every 48 hours until oxygen therapy was no longer needed, and for a maximum of 14 days (eight injections). Treatment could be discontinued if an adverse event potentially linked to the treatment occurred. Only trial-site pharmacists were aware of the treatment assigned to the patient. All other trial-site personnel and patients were blind to treatment assignment during the study.
Outcome MeasuresFor cohorts 1 and 3, the primary outcome was clinical status improvement on days 14 and 28, assessed with the WHO ordinal scale. For patients in cohort 2, the primary outcome was the number of ventilator-free days at day 28 (VFD28). VFD28 was assessed 28 days after enrollment and was defined as the number of days on which the patients were alive and had been completely weaned off IMV for at least 48 hours. Patients who had died by day 28 were considered to have had zero ventilator-free days (23).
The secondary outcome measures were clinical status improvement on days 14 and 28 according to the WHO ordinal scale (cohort 2), ventilator-free days at day 14 (VFD14) and VFD28 for ICU patients, Sequential Organ Failure Assessment (SOFA) score at day 14 in ICU patients, the occurrence of adverse events, the occurrence of secondary bacterial or fungal sepsis (24), the rate of patient discharge alive from the hospital or from the ICU before day 14 (WHO score < 4 or < 6, respectively), and mortality at day 28.
Statistical AnalysisThe statistical analysis was based on Gaussian tests comparing the mean clinical improvement assessed with the WHO score ordinal scale (cohorts 1 and 3) and mean VFD28 (cohort 2). For cohort 1, we calculated that a sample size of 90 patients would provide a power of more than 76% for detecting a 1.0-point difference on day 14 and a power of more than 88% for detecting a 1.2-point difference between treatment arms on day 28. For cohort 2, a sample size of 48 patients would provide a power of more than 96% for detecting a clinically significant improvement of at least 2 days in the primary outcome (VFD28) with a 5% type I error (one-tailed test). For cohort 3, a sample of 60 patients would provide the trial with a power of more than 80% for detecting a 1.3-point difference at day 14 and a power of more than 89% for detecting a 1.5-point difference between treatment arms at day 28. A fallback procedure was used to control for familywise type I error after multiple testing (25).
The intention-to-treat population (ITT) included all patients randomized and assigned to a treatment arm. In cohort 1, the modified-ITT (m-ITT) population included only the patients enrolled after protocol amendment. The per-protocol (PP) population was based on the treatment effectively received; patients not meeting the inclusion criteria were excluded. The population for the safety analysis included all patients receiving at least one dose of avdoralimab or placebo.
Post hoc exploratory analyses were performed for factors believed to influence COVID-19 outcomes. Logistic regression models with odds ratios were used to evaluate the impact of known prognostic factors for COVID-19 on WHO ordinal scale score at day 14 (≤ 4 vs ≥ 5) and mortality at day 28. In both models, treatment arm was forced into the model, to evaluate the impact of treatment on outcome.
The statistical analyses were performed with the SAS software Version 9.4 and the RStudio software version 1.1.456. Sample size was calculated with the East 6 software (Cytel). Results are expressed as means (sd).
Supplementary methods (selection of avdoralimab dose, additional statistical analyses, and exploratory laboratory analysis) are detailed in Appendix 2 (https://links.lww.com/CCM/H213). The full protocol and statistical analysis plan detailing the statistical approach are available in Appendix 5 (https://links.lww.com/CCM/H213) (protocol details).
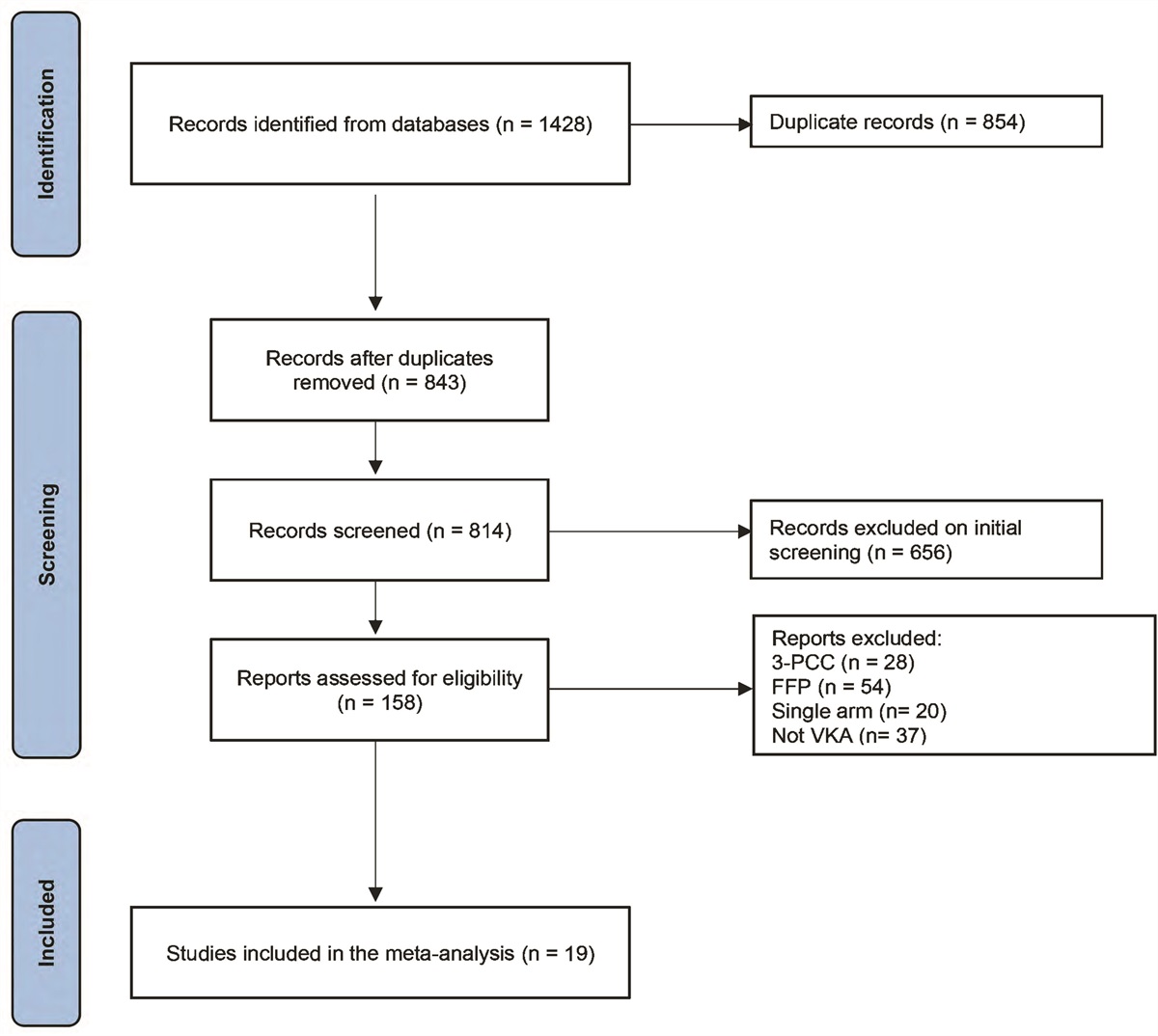
RESULTS Patient CharacteristicsBetween May 2020 and January 2021, 207 patients were randomized and included in the ITT population: 99 patients in cohort 1 (50 and 49 in the avdoralimab and placebo groups, respectively); 49 patients in cohort 2 (24 and 25, respectively); and 59 patients in cohort 3 (29 and 30, respectively). The ITT and PP populations are shown in Figure 1. Reasons for withdrawal from the study are described in Table S2 (https://links.lww.com/CCM/H213).
 Figure 1.:
Figure 1.: Flowchart. In cohort 1, 50 patients were assigned to receive avdoralimab (intention-to-treat [ITT] population), and 47 (94%) received the treatment as assigned (per-protocol [PP] population): three were on invasive mechanical ventilation (IMV) at first treatment administration. In cohort 1, 49 patients were assigned to receive placebo (ITT population), and 45 (92%) received placebo as assigned (PP population): one was assigned to placebo but switched treatment arms during the study, and three were on IMV at first treatment administration. In cohort 2, 24 patients were assigned to receive avdoralimab (ITT population), and 23 received the treatment as assigned. One patient was on conventional oxygen therapy at first treatment administration. In cohort 2, 25 patients were assigned to receive placebo (ITT population), and 24 (96%) received placebo as assigned: one was assigned to placebo but received avdoralimab. As this patient received only avdoralimab, he was switched to the avdoralimab group in the PP population. In cohort 3, 100% of patients received their assigned treatment in either arm; 29 patients received avdoralimab, and 30 patients received placebo (ITT and PP populations).
Baseline demographic data and medical history were largely similar between cohorts and treatment groups (Table 1). Mean patient age was higher for the avdoralimab-treated patients in cohort 3 (69.1 yr [7.5]), the mean age across cohorts being 63.7 years (10.4). Most of the patients enrolled were male (71%; n = 147/207) (Table S3, https://links.lww.com/CCM/H213—for the characteristics of the total population at baseline). Most patients had at least one risk factor at baseline, mostly hypertension (51%, n = 105/207), obesity (45%, n = 93/207), or type 2 diabetes (36%, n = 75/207). In cohort 2, obesity was more prevalent among the patients of the placebo group (64%, n = 16 vs 33%, n = 8). A larger number of patients in the avdoralimab group than those in the placebo group had comorbidities: cancer (21%, n = 5 vs 4%, n = 1) in cohort 2, cardiovascular disease in cohort 2 (33%, n = 8 vs 16%, n = 4) and cohort 3 (28%, n = 8 vs 17%, n = 5), and chronic obstructive pulmonary disease (21%, n = 6 vs 7%, n = 2) in cohort 3.
TABLE 1. - Patient Characteristics at Baseline (Intention-to-Treat Population Population)a,b Cohort 1 Cohort 2 Cohort 3 Demographic data Avdoralimab, n = 50 Placebo, n = 49 Avdoralimab, n = 24 Placebo, n = 25 Avdoralimab, n = 29 Placebo, n = 30 Age, yr 63.2 (10.4) 60.8 (12.5) 65.0 (7.8) 63.3 (9) 69.1 (7.5) 63.6 (10.6) Sex—M (n [%]) 36 (72) 30 (61) 18 (75) 19 (76) 21 (72) 23 (77) BMI (kg/m2) 29.8 (5.9) 30.3 (5.7) 28.9 (5.7) 31.2 (6.0) 31.1 (4.2) 30.3 (4.7) Risk factors Obesity (n [%]) 25 (50) 19 (39) 8 (33) 16 (64) 12 (41) 13 (43) Hypertension (n [%]) 25 (50) 26 (53) 9 (38) 13 (52) 19 (66) 13 (43) Diabetes (n [%]) 16 (32) 18 (37) 10 (42) 10 (40) 14 (48) 7 (23) Comorbidities (chronic diseases) Cardiovascular disease (n [%]) 13 (26) 12 (25) 8 (33) 4 (16) 8 (28) 5 (17) Chronic obstructive pulmonary disease (n [%]) 1 (2) 3 (6) 1 (4) 3 (12) 6 (21) 2 (7) Chronic kidney disease (n [%]) 1 (2) 3 (6) 2 (8) 2 (8) 2 (7) 1 (3) Cancer (n [%]) 7 (14) 5 (10) 5 (21) 1 (4) 2 (7) 2 (7) COVID-19 diagnosis Positive severe acute respiratory syndrome coronavirus-2 reverse transcription polymerase chain reaction (n [%])c 50 (100) 49 (100) 23 (96) 24 (96) 29 (100) 30 (100) Viral load at inclusion (Ct)d 27.9 (6.6) 23.8 (8.1) 23.3 (4.6) 24.4 (4.2) 27.1 (5.6) 26.6 (6) Time from first signs to inclusion (d) 9.2 (3.3) 9.8 (2.9) 10.1 (3.9) 10.2 (4.1) 10.6 (4.5) 10.7 (3.2) Time from hospitalization to inclusion (d) 2.1 (1.7) 2.4 (2.5) 2 (1.6) 1.4 (1.2) 2.3 (1.6) 2.8 (1.8) COVID-19 severity at inclusion World Health Organization Scale (n [%]) 5: Hospitalized, oxygen by mask or nasal prongs 8 (16) 10 (20) 1 (4) 0 (0) 0 (0) 0 (0) 6: Hospitalized, oxygen by NIV or HFO 40 (80)e 36 (74) 13 (54) 15 (60) 0 (0) 0 (0) 7: IMV and P/F ratio ≥ 150 0 (0) 1 (2) 5 (21) 2 (8) 3 (10) 4 (13) 8: IMV and P/F ratio < 150 or vasopressors 0 (0) 0 (0) 4 (17) 4 (16) 15 (52) 14 (47) 9: IMV and P/F ratio < 150 and vasopressors, RRT, or extracorporeal membrane oxygenation 2 (4) 2 (4) 1 (4) 4 (16) 11 (38) 12 (40) Sequential Organ Failure Assessment 3.8 (1.3) 4.0 (1.6) 5.2 (2.2) 5.7 (3.0) 7.1 (2.7) 6.7 (2.3) P/F ratio—ICU patients (HFO/NIV or IMV) 119 (52) 118 (64) 133 (62) 131 (57) 127 (56) 130 (48) Positive end-expiratory pressure (cm H2O)—IMV patients — — 12.6 (1.9) 12.4 (3.8) 12.8 (2.8) 12 (2.5) Tidal volume (mL)—IMV patients — — 422 (17) 417 (52) 410 (53) 418 (51) Lesions on CT-scans, n (%) Limited 3 (6) 3 (6) 3 (13) 1 (4) 1 (3) 0 (0) Moderate 20 (40) 18 (37) 2 (8) 4 (16) 5 (17) 8 (27) Severe 10 (20) 18 (37) 8 (33) 7 (28) 6 (21) 6 (20) CT scan not done 17 (34) 10 (20) 11 (46) 13 (52) 17 (59) 16 (53) Concomitant drugs, n (%) Antibiotics 15 (30) 14 (29) 6 (24) 7 (29) 15 (52) 18 (60) Dexamethasone 41 (82) 42 (86) 22 (88) 18 (75) 28 (97) 25 (83) Methylprednisolone 15 (30) 11 (23) 3 (13) 5 (20) 5 (17) 10 (33) Number of perfusions (avdoralimab or placebo) 5.7 (2.1) 5.3 (2.2) 6.1 (2.3) 6 (2.3) 6.1 (2.4) 6.8 (2)HFO = high-flow oxygen, IMV = invasive mechanical ventilation, NIV = noninvasive ventilation, P/F = Pao2/Fio2.
aPlus-minus values are means ± sd.
bBaseline was defined as the last known observation before the administration of avdoralimab or placebo on day 1.
cTwo patients in cohort 2 were not tested by polymerase chain reaction. For these patients, diagnosis was confirmed by lung CT-scan
dViral load was assessed in a total of 88 patients. In cohort 1: n = 15 (avdoralimab arm) and n = 14 (placebo arm). In cohort 2: n = 11 (avdoralimab arm) and n = 14 (placebo arm). In cohort 3: n = 17 (avdoralimab arm) and n = 17 (placebo arm).
eOne patient included in this category was on IMV at the time of first treatment administration but was listed as having a World Health Organization score of 6 at inclusion.
Most patients (95%, n = 196) received glucocorticoids (including dexamethasone and methylprednisolone) during the course of the trial (Table 1; and Table S3, https://links.lww.com/CCM/H213).
Disease characteristics at baseline were also well-balanced between the treatment arms (Table S4, https://links.lww.com/CCM/H213). All but two patients had SARS-CoV-2 infection confirmed by nasopharyngeal PCR test. The two remaining patients were enrolled in cohort 2, and their COVID-19 diagnosis was confirmed by lung CT scan. The mean (±sd) time from the onset of COVID-19 symptoms to enrollment was 9.8 days (±3.8 d) in the avdoralimab-treated groups and 10.1 (±3.3) in the placebo-treated groups. Disease severity, as assessed by SOFA, Simplified Acute Physiology Score 2 scores and P/F ratios (Table 1), and mean number of perfusions (Table 1; details in Table S11, https://links.lww.com/CCM/H213) were similar for all treatment arms in all three cohorts (Table 1).
Primary OutcomeIn cohorts 1 and 3, there was no significant difference in clinical improvement on the WHO ordinal scale between patients in the avdoralimab and placebo groups, on days 14 and 28 (Table 2). On day 28, the between-group difference in mean WHO scale improvement between the groups (avdoralimab vs placebo, so negative results mean favor placebo and positive results favor avdoralimab) was –0.3 (95% CI, –1.2 to 0.7; p = 0.7) in cohort 1; and –0.3 (95% CI, –1.8 to 1.2; p = 0.6) in cohort 3. The data for day 14 are shown in Table 2. Similar results were obtained for the m-ITT and PP populations in all cohorts (Tables S5 and S6, https://links.lww.com/CCM/H213).
TABLE 2. - Primary and Secondary Efficacy Outcomes (Intention-to-Treat Population Population) a Cohort 1 Cohort 2 Cohort 3 Outcomes Avdoralimab, n = 50 Placebo, n = 49 Avdoralimab, n = 24 Placebo, n = 25 Avdoralimab, n = 29 Placebo, n = 30 World Health Organization scale score improvement D14 1.2 (2.3) 1.4 (2.1) 0.7 (2.6) 1.4 (1.7) 1.2 (2.5) 1.4 (1.9) Difference of the means (avdoralimab vs placebo) (95% CI)b –0.3 (–1.1 to 0.6) –0.7 (–2.0 to 0.6) –0.2 (–1.3 to 1.0) p 0.71 0.86 0.61 D28 1.7 (2.8) 1.9 (2.1) 0.5 (3.1) 2.7 (2.1) 1.7 (3.0) 1.9 (2.6) Difference of the means (avdoralimab vs placebo) (95% CI)b –0.3 (–1.2 to 0.7) –2.2 (–3.7 to –0.6) –0.3 (–1.8 to 1.2) p c 0.70 0.99 0.65 VFD VFD14 NA NA 6.9 (6.7) 7.1 (6.4) 3.2 (4.4) 2.4 (4.2) Difference of the means (avdoralimab vs placebo) (95% CI)b — — –0.3 (–4.0 to 3.5) 0.8 (–1.4 to 3.1) p c — — 0.55 0.23 VFD28 NA NA 12.1 (13.6) 18.4 (10.4) 8.8 (11.1) 7.7 (10.3) Difference of the means (avdoralimab vs placebo) (95% CI)b — — –6.3 (–13.2 to 0.7) 1.0 (–4.5 to 6.6) p c — — 0.96 0.36 Mortality at D28, n (%) 6 (12) 3 (6) 4 (17) 2 (8) 10 (35) 7 (23) p c 0.32 0.36 0.35 AEs Sepsis 6 (12) 8 (16) 6 (24) 7 (29) 10 (35) 10 (33) Related AE 9 (18) 13 (27) 8 (32) 9 (38) 7 (24) 9 (30) Serious AE 18 (36) 13 (27) 13 (52) 11 (46) 19 (66) 20 (67)AE = adverse event, NA = not applicable, VFD = ventilator-free day.
aPlus-minus values are means ± sd.
bA negative result favors placebo. A positive result favors avdoralimab.
cIn a one-tailed Student t test (avdoralimab-placebo > 0).
For cohort 2, mean (±sd) VFD28 was 12.1 (13.6) for the avdoralimab group and 18.4 (10.4) for the placebo group, with a between-group difference of –6.3 days (95% CI, –13.2 to 0.7; p = 0.96) (Table 2).
Key Secondary and Safety OutcomesAvdoralimab was not effective for any of the secondary outcomes (Table 2; and Tables S5 and S6, https://links.lww.com/CCM/H213, for the m-ITT and PP populations, respectively). In cohort 2, no difference in clinical improvement on the WHO scale was observed between patients in the avdoralimab and placebo groups on days 14 and 28. On day 28, the between-group difference was –2.2 days (95% CI, –3.7 to –0.6; p = 0.99 in a one-tailed Student t test). In cohort 3, VFD14 and VFD28 were similar between the avdoralimab and placebo groups. Mean (sd) VFD28 was 8.8 (11.1) with avdoralimab and 7.7 (10.3) with placebo, with a between-group difference of 1 day (95% CI, –4.5 to 6.6; p = 0.36 in a one-tailed Student t test). Data for VFD14 are detailed in Table 2. Mortality rates at day 28 were higher, although not significantly, in the patients treated with avdoralimab than in those treated with placebo (19.4%, n = 20 vs 11.5%, n = 12, p = 0.12) (Table 2; and Tables S5 and S6 and Fig. S1, https://links.lww.com/CCM/H213).
SOFA score improvement at day 14 and the percentage of patients discharged from the hospital or from the ICU at days 7, 14, 21, and 28 were not improved by avdoralimab. In cohort 2, cumulative rates of discharge from hospital and the ICU were higher in the placebo group (Table S7, https://links.lww.com/CCM/H213).
Serious adverse events were reported in 48% (n = 50) and 43% (n = 44) of patients treated with avdoralimab and placebo, respectively. Sepsis was reported in 21% (n = 22) and 24% (n = 25) of patients treated with avdoralimab and placebo, respectively. Fatal events occurred in 27% (n = 28) of patients receiving avdoralimab and 16% (n = 16) of those receiving placebo, over all cohorts. Similar percentages of patients in each cohort had adverse events or serious adverse events (Table S8, https://links.lww.com/CCM/H213). The most commonly reported cause of death was COVID-19 pneumonia or COVID-19-related complications (Table S9, https://links.lww.com/CCM/H213).
Post Hoc Exploratory AnalysesWe accounted for factors believed to influence COV
留言 (0)