
記住我
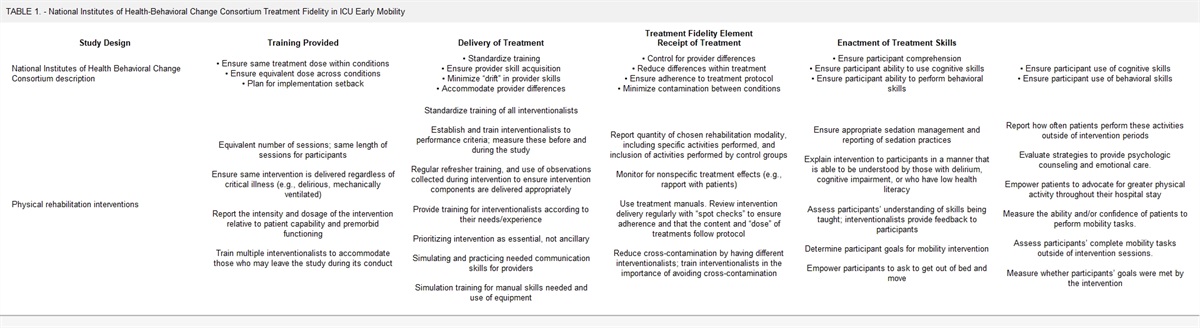
KEY POINTS
Question: This mixed-methods, guideline-based simulation study evaluated hypothetical (re-)allocation of ICU resources during the pandemic as performed by front-line intensivists. Findings: This simulation study found that the two-step prioritization approach, 1) assessment of each patient, 2) a prioritization visit across ICUs, is feasible and acceptable; while resource-intensive, it would be effective to prevent intuitive, non-reliable decisions. Triage would put tremendous burden on intensivists, but they would be willing to assume the responsibility if the approach was transparent, legal, and included interdisciplinary cooperation. Meaning: Combining clinical assessment by physicians plus a score-based protocol could be an alternative to other triage concepts.During the COVID-19 pandemic, the demand for intensive care has temporarily exceeded supply in some countries, so that rationing of resources (triage) became necessary (1–3). To date, no consensus has been reached on the criteria that should guide prioritization and triage (4–7).
When triage is looming, focus moves from exclusively patient-centred decision-making toward the inclusion of a perspective of population health (3,6,8). This shift is more than a simple exchange of protocols. Triage may require withdrawing or withholding life-sustaining measures for patients who otherwise would have been treated until leaving the ICU or until death. Rationing whose life support to terminate, or not to initiate, is ethically challenging, medically complex, and emotionally draining. The difficulties are not just conceptual; they also pertain to putting guidelines into practice.
Triage concepts across the world differ, for example, in defining exclusion criteria for treatment and/or implementing triage officers (9). Several studies have already proved feasibility and accuracy of allocation concepts, but there are still many unresolved questions about how to predict short-term survival best, how to mitigate risks of biases or limitations of scores, and how to implement the fairest (re-)allocation (10–12).
In line with broader international consensus, a German guideline developed and refined in 2020/2021 focuses on a multiprinciple approach including: 1) likelihood of survival to hospital discharge as guidance, 2) evaluating all patients eligible for ICU treatment including reallocation, 3) ensuring transparency, and 4) applying interdisciplinary decision-making to reduce the risks of biases, inequity, and discrimination (13). To respond to the lack of consensus about triage scoring systems and to prevent biases, an interdisciplinary triage team of at least two experienced treating intensivists, specialists, and optionally ethicists should collaborate and share allocation decisions (13–15).
The aim of this study is to evaluate, in hypothetical form, the feasibility, reliability, and acceptability of an institutional prioritization protocol that was developed in our university hospital based on the German guideline. This real-time simulation study allowed to analyze the prognostic assessment of front-line physicians, the hypothetical resource (re-)allocation, and the intensivists’ perspectives on this protocol. The findings are relevant not only for preparation in the current pandemic but also particularly critical for future public health crises, should clinicians need to ration scarce resources.
MATERIALS AND METHODS Study design, Setting, and ParticipantsThis study is a prospective observational monocentric hypothetical cohort study during the second wave of the COVID-19 pandemic in Germany from December 2020 to March 2021 at five ICUs: two from internal medicine and three from anesthesiology and intensive care medicine at a German university hospital. We applied a convergent parallel design of quantitative and qualitative methods and linked results for interpretation. The study was conducted in agreement with the principles of the Declaration of Helsinki, and the Ethics Committee of the Technical University of Munich approved the study protocol (approval number 675/20 S). All participating physicians were approached by e-mail and informed about the study background, methods, and data protection.
Simulation Intervention and Quantitative Data CollectionAll participating intensivists were trained on the background and protocol of triage in a 2-hour lecture and written materials. To prepare for the hypothetically upcoming triage, a patient survey form (Supplementary Material, https://links.lww.com/CCM/H211) had to be completed for inpatients in the five ICUs collecting information on the acute illness, preexisting general health, comorbidities, duration of ICU stay as well as on patients’ will and patient-centered treatment plan. During a 2-day preparation, intensivists had to assess their patients’ likelihood to survive the current treatment. They had to compare and categorize them into groups with “good,” “moderate,” and “unfavorable” prognoses on their ICU. No specifications were given for the scoring of individual items or diagnoses; intensivists were asked to decide according to their clinical judgment. Considering the underlying disease, the attending specialists (e.g., surgeons, neurologists) could have been consulted for patient-centered decision-making and prognostic assessment. The attendings of each ICU had to report two patients who were least likely to survive for the prioritization visit. The assessment of each ICU patient and the resulting choice of two patients per ICU presented a compromise between a manageable number of patients for the prioritization visit in the emergency situation and the need to assess as many patients as possible to make a fair and transparent allocation decision. For the simulation, five prioritizations teams were formed, each consisting of two attendings or senior physicians in intensive care, one from internal medicine, and one from anesthesiology. Three teams assessed in person, two teams reviewed only the survey forms and medical files. All teams were asked to rank the preselected patients according to their likelihood to survive the current treatment. Three intensivists were not available on the day of the prioritization visit due to various commitments. All patients included were followed up until hospital discharge or death.
In case of a pandemic crisis, this ordering by a prioritization team would have been the baseline for triage if no other resources were available at the hospital and beyond for additional critically ill patients.
Focus Group and Qualitative Data CollectionThe participating intensivists were selected by purposive sampling with the criteria: 1) senior ICU-attendings, 2) participation in study simulation, and 3) interest in the research question. The day after the simulation, they were assigned to one of two groups matched to their duty responsibilities. Each focus group (FG), one virtually and one face-to-face, took 90 minutes. Both were moderated by the first author (K.Kn.), who has a background in intensive care and clinical ethics. Field notes were made by another researcher (K.A.). There was no hierarchical relationship between the researchers and the participants. The semistructured interview guide developed according to Helfferich was discussed, piloted, and revised in research group meetings and within the local expert network for qualitative research (16). The full methods description employed the COnsolidated criteria for REporting Qualitative research (Supplemental Material, https://links.lww.com/CCM/H211) (17).
Outcome VariablesPrimary outcome with regard to the patients included was the survival of acute illness in terms of in-hospital mortality. Secondary outcomes were length of ICU stay, length of inpatient stay, and ICU mortality.
The qualitative analysis focused on how intensivists perceived the prioritization during a simulated situation of impending pandemic overload of intensive care resources and how they evaluated the applied protocol. Quantitative and qualitative data were analyzed separately and subsequently integrated for interpretation (18).
Statistical MethodsContinuous ICU patient data were described by median, 25th and 75th percentiles, and categorical data by absolute and relative frequencies. Relevant patients’ characteristics were compared by Mann-Whitney U test (continuous variables) and chi-square test or Fisher exact test (categorical variables), respectively. Using binary logistic regression analysis, significant predictors of hospital mortality were determined, and area under the receiver operating characteristic (ROC) curve was used to quantify the predictive ability for hospital mortality. All analyses were conducted two-sided using a 5% level of significance and 95% CIs and calculated for relevant effect sizes. Statistical analyses were performed using Microsoft Excel 2013 and IBM SPSS Statistics Version 26.0 (IBM Corp, Armonk, NY).
Qualitative AnalysisThe FG discussions were audio-recorded, transcribed verbatim with simple transcription rules, and anonymized. The transcripts were analyzed by author (K.Kn.), who is experienced in qualitative research, and by authors (K.A., E.S.), who were trained in qualitative methods. A content-structured qualitative analysis according to Kuckartz (19) was performed, using the software MAXQDA 12 (VERBI– Software GmbH, Berlin, Germany). We applied a data-driven strategy for a descriptive, content-based analysis using open coding. The codes were listed and systematized in a hierarchical coding frame. The category system was discussed, cross-validated, and revised by the research team. The coding frame was revised in a second application to the material. The resulting coding guide was applied to the whole material and is available on request. Illustrative quotes are listed with FG and participant number (P). Preliminary results were discussed with participants in a plenary session.
RESULTSOn the simulation day, 64 beds were in operation, 61 occupied in the five ICUs, and 53 patients could be included in the study (Fig. 1). Patients who were redirected to palliative comfort care or transferred for recovery were excluded. The median age was 69 years (Q25–Q75: 57–76 yr); 70% were male. Participating intensivists (n = 13) assessed the prognosis as “good” in 29, “moderate” in 17, and “unfavorable” in seven patients. When the forecasts were later compared with actual mortality rates at the hospital, there was good concordance: good equals to 13.8% mortality, moderate equals to 64.7%, and unfavorable equals to 71.4% (Table 1).
TABLE 1. - Characteristics and Outcome Variables of the Study Cohort Characteristics, Median (25–75th Percentiles) Unless Otherwise Indicated Total Cohort (N = 53) Predicted Outcome: Good (N = 29) Predicted Outcome: Intermediate (N = 17) Predicted Outcome: Unfavorable (N = 7) Not Nominated for Prioritization Simulation (N = 43) Nominated for Prioritization Simulation (N = 10) p a Age (yr) 69 (57–76) 67 (57–75) 74 (55–76) 73 (58–75) 68 (56–77) 73 (64–76) 0.707 Male sex, n (%) 37 (69.8) 19 (65.5) 13 (76.5) 5 (71.4) 30 (69.8) 7 (70) 1.0 Eastern cooperative oncology group performance status 1 (0–2) 0 (0–2) 1 (0–2) 1 (0–1.5) 1 (0–1.5) 2 (0.25–2.75) 0.19 Karnofsky index 80 (70–90) 80 (70–90) 80 (67.5–90) 74 (62.5–95) 80 (70–90) 75 (60–85) 0.509 Clinical Frailty Scale 3 (2–4.5) 3 (1.5–5) 3 (2–4) 3 (2–5) 3 (2–4) 3 (2.5–5.5) 0.402 Charlson Comorbidity Index 4 (2–6) 4 (2–5) 4 (3–7) 5 (3–7) 4 (2–5.5) 6 (3.5–6.75) 0.075 Duration of ICU stay (on day of prioritization) 11 (6–21) 9 (3–17) 13 (7–21) 35 (25–44) 9 (4–19) 28 (20–37) 0.001 Duration of hospital stay (on day of prioritization) 18 (8–29) 14 (6–21) 21 (11–19) 46 (34–52) 13 (7–21) 42 (27–55) < 0.001 Sequential Organ Failure Assessment score (on day of prioritization) 6 (3–10) 4 (2–6) 10 (7–12) 8 (6–11) 6 (3–9.5) 9 (7.25–11.5) 0.038 COVID-19 patients, n (%) 16 (30.2) 5 (17.3) 8 (47.1) 3 (42.8) 13 (30.2) 3 (30) 1.0 Duration of ICU stay (d) 32 (19–48) 26 (12–41) 34 (22–53) 55 (42–68) 27 (15–43.5) 50 (41–71) 0.008 Duration of hospital stayb (d) 62 (35–138) 85 (35–142) 43 (31–108) 88 (65.5–153) 55 (32–137) 79 (59–136) 0.251 Mortality (ICU), n (%) 16 (30.2) 4 (13.8) 9 (52.9) 3 (42.9) 10 (23.3) 6 (60) 0.05 Mortality (hospital), n (%) 20 (37.7) 4 (13.8) 11 (64.7) 5 (71.4) 12 (27.9) 8 (80) 0.004aMann-Whitney U test (continuous variables) and chi-square or Fisher exact test (categorical variables) comparing patients selected/respectively not selected for prioritization simulation.
bIncluding further treatment and/or rehabilitation hospitals until discharge (to home, nursing home, or death).
 Figure 1.:
Figure 1.: Flowchart of patients nominated for the simulated prioritization visit. The classification into “good,” “moderate,” and “unfavorable” prognoses was based on the ICU clinician’s judgment (without more specific group-defining information). *Including patients with a changed treatment goal toward palliative comfort care.
The patients nominated for a prioritization visit (n = 10)—the two with the worst forecasts per each ICU—had higher Sequential Organ Failure Assessment (SOFA) scores and a prolonged intensive care and hospital stay until that moment. The predicted poor outcome was confirmed by an in-hospital mortality rate of 80%; details are shown in Table 1. None of the prioritization teams considered the two survivors to have the worst or second-worst prognosis. Four of the five teams identified the same patient as having the most unfavorable prognosis, but in general the comparison within this group of patients with a very low probability of survival to hospital discharge was not concurrent (Fig. 2).
 Figure 2.:
Figure 2.: Grouping of patients nominated for the simulated prioritization visit. Illustrated are the 10 patients nominated for the prioritization visit, sorted by estimated prognosis by each prioritization team (1–5) from less unfavorable (left side of figure) to most unfavorable (right side of figure). Each symbol (star, pentagon, etc.) refers to a specific patient. The prioritization teams had access to patient data, records, and survey forms. Teams 1, 2, and 3 visited the patients, whereas teams 4 and 5 performed the assessment and grouping only after reviewing the available records.
In binary logistic regression analysis, age (p = 0.029) and SOFA score at the point of prioritization visit (p = 0.007) were significant predictors of in-hospital mortality leading to an area under the ROC curve of 0.87. The statistical model predicted the in-hospital mortality for all included patients. The 10 with calculated worst prognosis (ranging from 77.7% to 90.6%) had an observed in-hospital mortality of 60%. However, participating physicians were comparatively more accurate. Compared with the statistical model, the group of 10 patients nominated by the intensivists had a mortality of 80% (Table 1 and Fig. 2).
The thirteen participating intensivists, ranging in age from 37 to 56 years (median, 42 yr), had 3–21 years of ICU experience (median, 7 yr). All but one, who was prevented by duty, participated in the FGs. All emphasized that everything must be done to prevent rationing and triage. Qualitatively, we identified the following three themes that describe challenges of implementing an institutional pandemic rationing protocol. An overview is summarized in Table 2.
TABLE 2. - Core Statements and Illustrative Quotes From Intensivists About Challenges of Triage and Benefits of an Institutional Protocol After a Simulation of Rationing Decision-Making During a Pandemic Subthemes Challenges of Triage Decision-Making Benefits of Institutional Triage Protocol Likelihood to survive the current acute illness as the single criterion Implication to disregard the long-term outcome and the general aim at reasonable outcomes, not only at survival is challenging.Participants highlighted that focusing exclusively on the likelihood of survival to hospital discharge differs from general goals in intensive care, which also consider the long-term prognosis. The intensivists characterized the comparative analysis of their patients as completely different from nonpandemic decision-making. They worried that the time pressure may prevent the common step-by-step shared decision-making and would mean less time for surrogates for farewell.
“[in non-pandemic times] we communicate about limitation of treatment, and then it usually takes at least two days until the relatives have discussed it until they have gathered together, until they have said goodbye. So far, no one is prepared for an abrupt termination of treatment.” (FG1, PA)
The Human Factors Influencing Decision-MakingParticipants underlined the influence of qualifications, work experience, and the role of personal attitudes on decision-making. More professional years bring more experiential knowledge, but professional action was also seen to entail a risk of bias. Participants emphasized their physicians’ duties to care and to respect patients’ preferences even when being different from their own values. Knowing a patient’s disease trajectory was characterized not only as prerequisite for prognostic assessment but also considered a risk of bias. Still, all stressed, that if the worst-case scenario required triage, they would like to assess the patients selected for triage themselves, instead of relying only on assessments by others, so they would be more certain of their decisions. Reflecting critically on limits of their professional competencies, they suggested the involvement of colleagues and further specialists for the best qualified and most objective assessment of patients’ individual prognoses.
The Challenges of Triage and Benefits of the Institutional ProtocolDuring the simulation, the participants perceived high complexity of decision-making that goes beyond the individual patient’s interest. Key benefits of the practice model were the preparation period, the consensus-oriented team-based decision-making approach, and the focus on the prognosis of short-term survival that they estimated as being less influenced by personal values and therefore less prone to bias. Preexisting severe illness or advanced age were described as a potentially higher risk in influencing prognostic assessment than acute severe illness, for example, trauma with high prognostic uncertainty but also a high risk to die. Participants stressed what they found helpful in decreasing these risks of misjudgment: 1) making allocation decision not based on one particular moment in time but on serial information about the patient’s course of treatment, 2) engaging other treating specialists, and 3) considering time for interdisciplinary exchange. The stepwise approach was perceived as resource-extensive but effective to prevent spontaneous or/and intuitive decisions. The default of assessing solely the short-term survival without considering long-term outcome and quality of life was perceived as challenging by participants. They had to deliberately disregard reflection on individual attitudes toward a good life in light of severe neurologic impairment.
All participants were in favor of adding the face-to-face prioritization visit to the survey form. Scores about general health status and comorbidities were seen as only one part but as not decisive for their prognostic assessment. More information about the acute illness and sufficient time for interdisciplinary exchange was suggested. Further, participants requested absolute transparency for surrogates, family members, team members, clinic staff, and the general public about applying such a protocol. They stressed the need for societal consensus and legal permission.
All participants agreed that prioritization and triage would be a tremendous burden and enormously challenging for physicians. “It felt like handing someone over to death” (FG2 PL). The requested consensus-oriented team-based assessment with ICU colleagues and specialists was perceived as crucial. They were however not in favor of fully delegating the decision-making to other professions, to specialties, or to triage officers. For moderation and communication of allocation decisions, participants suggested that the prioritization team should involve clinical ethicists. Overall, the protocol was perceived as extremely helpful, reassuring, and a supporting tool to meet the emotional burden.
DISCUSSIONThe present study sought to hypothetically test the implementation of a prioritization protocol during a simulation of an impending ICU resource overload. Exploring intensivists’ experiences reveals challenges of the triage dilemma and the benefits of an institutional protocol.
For decades, experts have engaged in an ethical debate about fair allocation of scarce medical resources (9,20–22). During triage, the focus shifts from exclusively patient-centered decisions to an increasing consideration of obligations toward a collective of patients. The need arises to decide about the best use of scarce health resources (23,24). The values that guide prioritization differ between jurisdictions. Although some states—like the United Kingdom or South Africa—lean toward utilitarian principles, other countries place more emphasis on egalitarian values—for example, Austria or Spain (25-28). The criteria that are supposed to be applied in clinical practice require a balancing between these different accounts of distributive justice. Options are to decide according to the rule to save as many lives as possible, the rule “first come first served,” or a lottery. A subset of the debate asks whether certain groups of people, such as healthcare workers or children, should be given special status (29,30). Each criterion comes with different ethical and social benefits and problems, and a full ethical deliberation is beyond the scope of this article (4,5,7,31).
In Germany, key professional associations collaborated considering the ethical, social, and medical dimensions of ICU resource prioritization in a pandemic overload (13,32). The resulting guideline attempted to align individual and public health interests aiming at minimizing preventable deaths, ensuring adequate healthcare, and preventing discrimination. In contrast to other countries, such as Switzerland, that categorically set limits regarding age and frailty, the German guideline focuses on a comparative analysis and on allocation across all patients with ICU needs (13,33). Main criteria for triage decisions are acute chance of survival and collaborative decision-making.
When testing the German recommendations, we found that forecasting short-term survival is suitable, feasible, and to some extent reliable. Our study shows that SOFA score and length of ICU stay were the variables that—in hindsight—correlated most strongly with the worst prognosis. The SOFA score is a common criterion in triage protocols (8). However, it should be noted that there is a risk of disadvantaging marginalized patients through protocols that rely on it (34). In our study, SOFA score was one among several criteria and as such our findings support its usefulness. Our data did not answer the questions about limitations of SOFA score nor whether comorbidity or frailty scores applied according to the guideline are indicative at all of the individual outcome prediction. It is known that frail patients, for example, have a reduced functional status and a higher risk of developing persistent critical illness as well as of subsequently dying from their condition (35). But as previously shown, the functional trajectory during hospital stay is not necessarily worse than that of nonfrail patients, suggesting a relevant rehabilitation potential (36). Our qualitative findings confirm the shortcomings of score-based prediction and the benefit of assessing more than one point in time. Including serial information, the course of the current illness and the response to treatment could lead to more certainty in predicting the survival for an individual patient. Thus, it could potentially decrease risks of discrimination due to pre-existing illness, age, or prognostic uncertainty. Similar to Butler et al (10,37), who in contrast applied a triage officer approach, our data underline the role of procedural criteria such as interdisciplinary assessment and collaborative decision-making as most decisive for estimating short-term survival, decreasing the risk of biases and for alleviating the burden of triage decisions. That said, the remaining prediction discordance within the patient group with the highest risk to die in the ICU raises the question whether better predictions tools could yield better judgments or whether there will always remain limits to differentiate precisely between these very severely ill intensive care patients.
In a simulated situation of extreme scarcity, intensivists were able to add to their professional duties toward the individual patient the duty to fulfill their obligation to distribute scarce resources fairly between all critically ill patients at the hospital. With regard to the principle of nonmaleficence and their professional duty to care, intensivists stressed their burden caused by the dilemma to withdraw or to withhold a therapy that could otherwise have been beneficial. Physicians require societal consensus as to how rules of distributive justice and procedural criteria should be translated into clinical settings for frontline decision-making. Other prerequisites for implementing protocols are regular education and training to prevent misapplication, to counteract risks of misinterpretation, and to prepare clinicians for their role in allocating scare resources (37–39).
In summary, our study confirms that the operationalization of a national triage guideline into an institutional protocol is feasible, acceptable, and supportive.
Our study has limitations. The single-center design in one European country cannot account for the contribution to the contingencies in other regional, legal, and social contexts. Furthermore, the results cannot be transferred to other hospitals. We increased the validity of our findings through triangulation by using a mixed methods approach that allowed to obtain deeper insights into challenges of implementing a prioritization protocol. Using a simulation allowed gaining knowledge that increases the pandemic preparedness of a crucial healthcare institution. Future research should focus on verifying a combination of criteria and allocation procedures to become as certain as possible and to prevent misuse.
CONCLUSIONSBefore an impending pandemic overload materializes, hospitals should implement and train a consensus-oriented, structured, and transparent approach to ensure ethically legitimate distribution of scarce ICU resources. To mitigate potential bias and minimize emotional burden of intensivists, allocation decisions should be supported by interdisciplinary physicians and clinical ethicists. Ongoing information including on current response to treatment is useful. However, differentiating between patients with very low chances to survive remains challenging and requires further conceptual and empirical research. A prioritization and triage protocol, its assignment or categorical criteria and procedural measures, need to be publicly debated and analyzed by further research.
ACKNOWLEDGMENTSWe would like to thank the participating physicians of the departments of Internal Medicine and the department of Anesthesiology and Intensive Care at the University Hospital rechts der Isar, School of Medicine, Technical University of Munich for their interest and support during the challenging times of the COVID-19 pandemic. We also thank the Munich network of qualitative research in medicine and public health for the opportunity of discussing the study design and data analysis with qualitative researcher outside of the study group and Marie-Christine Fritzsche for her valuable contributions and feedback on the draft article.
REFERENCES 1. Faggioni MP, González-Melado FJ, Di Pietro ML: National health system cuts and triage decisions during the COVID-19 pandemic in Italy and Spain: Ethical implications. J Med Ethics. 2021; 47:300-307 2. Rosenbaum L: Facing COVID-19 in Italy — Ethics, logistics, and therapeutics on the epidemic’s front line. N Engl J Med. 2020; 382:1873–1875 3. Vergano M, Bertolini G, Giannini A, et al.: Clinical ethics recommendations for the allocation of intensive care treatments in exceptional, resource-limited circumstances: The Italian perspective during the COVID-19 epidemic. Crit Care. 2020; 24:165 4. Ehni HJ, Wiesing U, Ranisch R: Saving the most lives-A comparison of European triage guidelines in the context of the COVID-19 pandemic. Bioethics. 2021; 35:125–134 5. Jöbges S, Vinay R, Luyckx VA, et al.: Recommendations on COVID-19 triage: International comparison and ethical analysis. Bioethics. 2020; 34:948–959 6. Joebges S, Biller-Andorno N: Ethics guidelines on COVID-19 triage - An emerging international consensus. Crit Care. 2020; 24:201 7. Woesler M SH: Mechanical ventilation, triage and scoring - Notes on the state affairs in Europe at the beginning of the COVID-19 pandemic. 8. Antommaria AHM, Gibb TS, McGuire AL, et al.; Task Force of the Association of Bioethics Program Directors: Ventilator triage policies during the COVID-19 pandemic at U.S. hospitals associated with members of the association of bioethics program directors. Ann Intern Med. 2020; 173:188–194 9. Christian MD, Sprung CL, King MA, et al.; Task Force for Mass Critical Care; Task Force for Mass Critical Care: Triage: Care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest. 2014; 146:e61S–e74S 10. Butler CR, Webster LB, Sakata VL, et al.: Functionality of scarce healthcare resource triage teams during the covid-19 pandemic: A multi-institutional simulation study. Crit Care Explor. 2022; 4:e0627 11. Cheung WK, Myburgh J, Seppelt IM, et al.; Influenza Pandemic ICU Triage Study Investigators: A multicentre evaluation of two intensive care unit triage protocols for use in an influenza pandemic. Med J Aust. 2012; 197:178–181 12. Guest T, Tantam G, Donlin N, et al.: An observational cohort study of triage for critical care provision during pandemic influenza: ‘Clipboard physicians’ or ‘evidenced based medicine’? Anaesthesia. 2009; 64:1199–1206 13. Deutsche Interdisziplinäre Vereinigung Für Intensiv- Und Notfallmedizin (Divi): Entscheidungen über die Zuteilung intensivmedizinischer Ressourcen im Kontext der COVID-19-Pandemie (3. überarbeitete Fassung vom 14.12.2021). 2021. Available at: https://www.awmf.org/leitlinien/detail/ll/040-013.html. Accessed January 1, 2022 14. Raschke RA, Agarwal S, Rangan P, et al.: Discriminant accuracy of the SOFA score for determining the probable mortality of patients with COVID-19 pneumonia requiring mechanical ventilation. JAMA. 2021; 325:1469–1470 15. Nates JL, Nunnally M, Kleinpell R, et al.: ICU admission, discharge, and triage guidelines: A framework to enhance clinical operations, development of institutional policies, and further research. Crit Care Med. 2016; 44:1553–1602 16. Helfferich C: Die Qualität qualitativer Daten: Manual für die Durchführung Qualitativer Interviews. Fourth Edition. Heidelberg, Germany, Springer, 2011 17. Tong A, Sainsbury P, Craig J: Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007; 19:349–357 18. Creswell JW: Designing and Conducting Mixed Methods Research. Second Edition. New York, NY, SAGE, 2011 19. Kuckartz U: Qualitative Inhaltsanalyse. Methoden, Praxis, Computerunterstützung. Fourth Edition. Weinheim, Germany, Beltz Juventa, 2012 20. Sprung CL, Joynt GM, Christian MD, et al.: Adult ICU triage during the coronavirus disease 2019 pandemic: Who will live and who will die? Recommendations to improve survival. Crit Care Med. 2020; 48:1196–1202 21. Maves RC, Downar J, Dichter JR, et al.; ACCP Task Force for Mass Critical Care: Triage of scarce critical care resources in COVID-19 an implementation guide for regional allocation: An expert panel report of the task force for mass critical care and the American College of Chest Physicians. Chest. 2020; 158:212–225 22. Kain T, Fowler R: Preparing intensive care for the next pandemic influenza. Crit Care. 2019; 23:337 23. Jeffrey DI: Relational ethical approaches to the COVID-19 pandemic. J Med Ethics. 2020; 46:495–498 24. Pugh J, Wilkinson D, Palacios-Gonzalez C et al: Beyond individual triage: Regional allocation of life-saving resources such as ventilators in public health emergencies. Health Care Anal. 2021; 29:263–282 25. British Medical Association: COVID-19 – Ethical Issues and Decision-Making When Demand for Life-Saving Treatment Is at Capacity, 2022. Available at: https://www.bma.org.uk/media/4964/bma-covid-19-ethics-guidance-jan-2022.pdf. Accessed January 30, 2022 26. Gopalan PD, Joubert IA, Paruk F, et al.: The critical care society of Southern Africa guidelines on the allocation of scarce critical care resources during the COVID-19 public health emergency in South Africa. S Afr Med J. 2020; 110:700–703 27. Bioethikkommision - Bundeskanzleramt Österreich: Zum Umgang mit knappen Ressourcen in der Gesundheitsversorgung im Kontext der Covid-19-Pandemie, 2020. Available at: https://www.aem-online.de/fileadmin/user_upload/Stellungnahme_der_Bioethikkommission_zur_Covid19_Pandemie.pdf. Accessed December 14, 2021
留言 (0)