Description of the recruited sample
Forty-five adolescents agreed to participate, 29 (64%) of those in Heidelberg and 16 (36%) in Mainz. Thirty-four (76%) were diagnosed with CD, eleven (24%) with ODD. Thirty (67%) identified as male, 15 (33%) as female. Mean age was 14.4 (SD = 2.1; range: 11 – 18). Eleven adolescents (24%) went to lower secondary school (German: “Haupt-, Werkrealschule”), 13 (29%) to higher secondary school (German: Realschule), seven (16%) to high school, (four (9%) to special needs school, one (2%) to vocational school. For six adolescents (13%) differentiation was not possible (comprehensive school), and three (7%) did not go to school at intake.
Acceptability of intervention and scientific investigation in patient groupRecruitment and therapy adherence
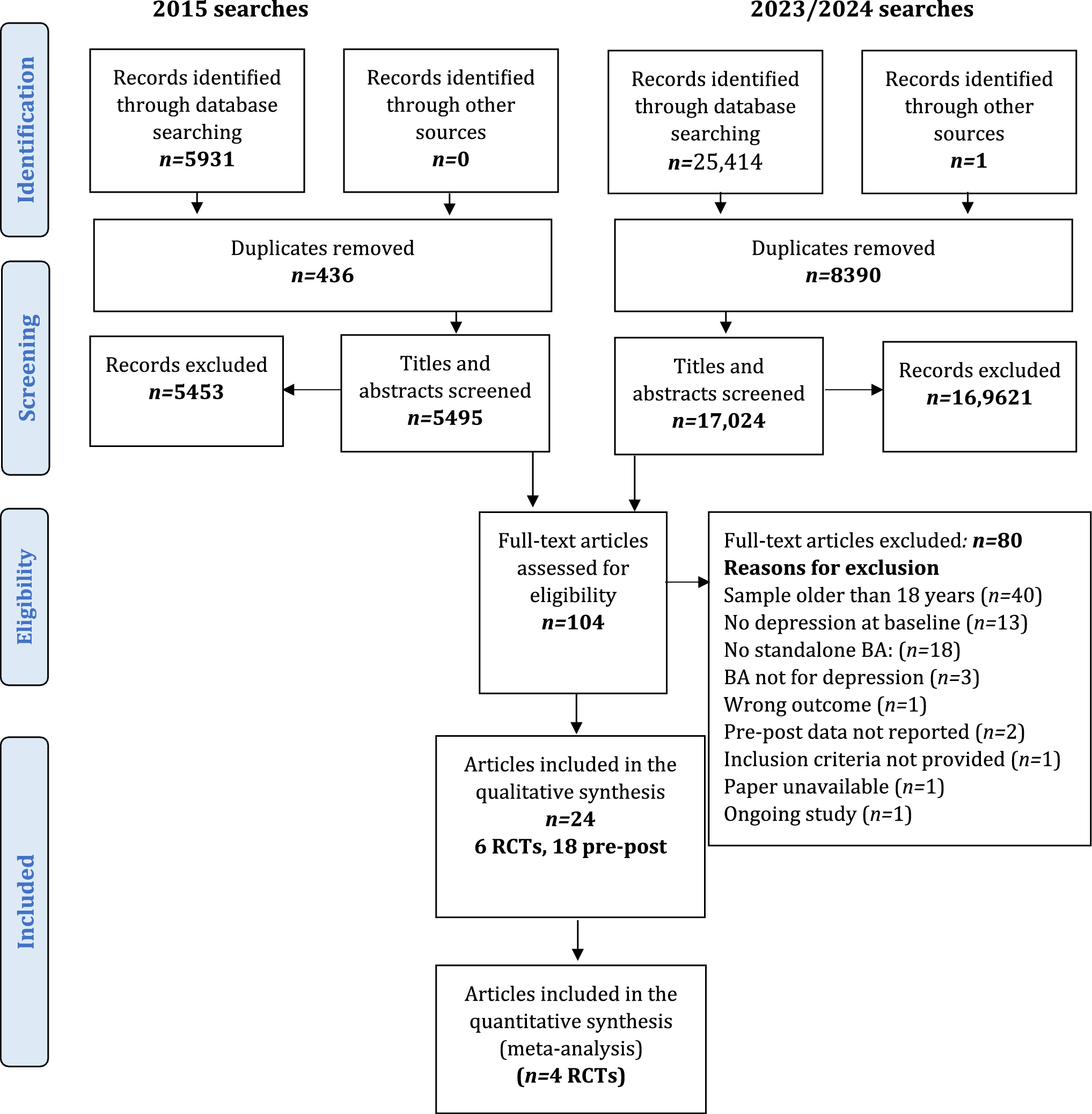
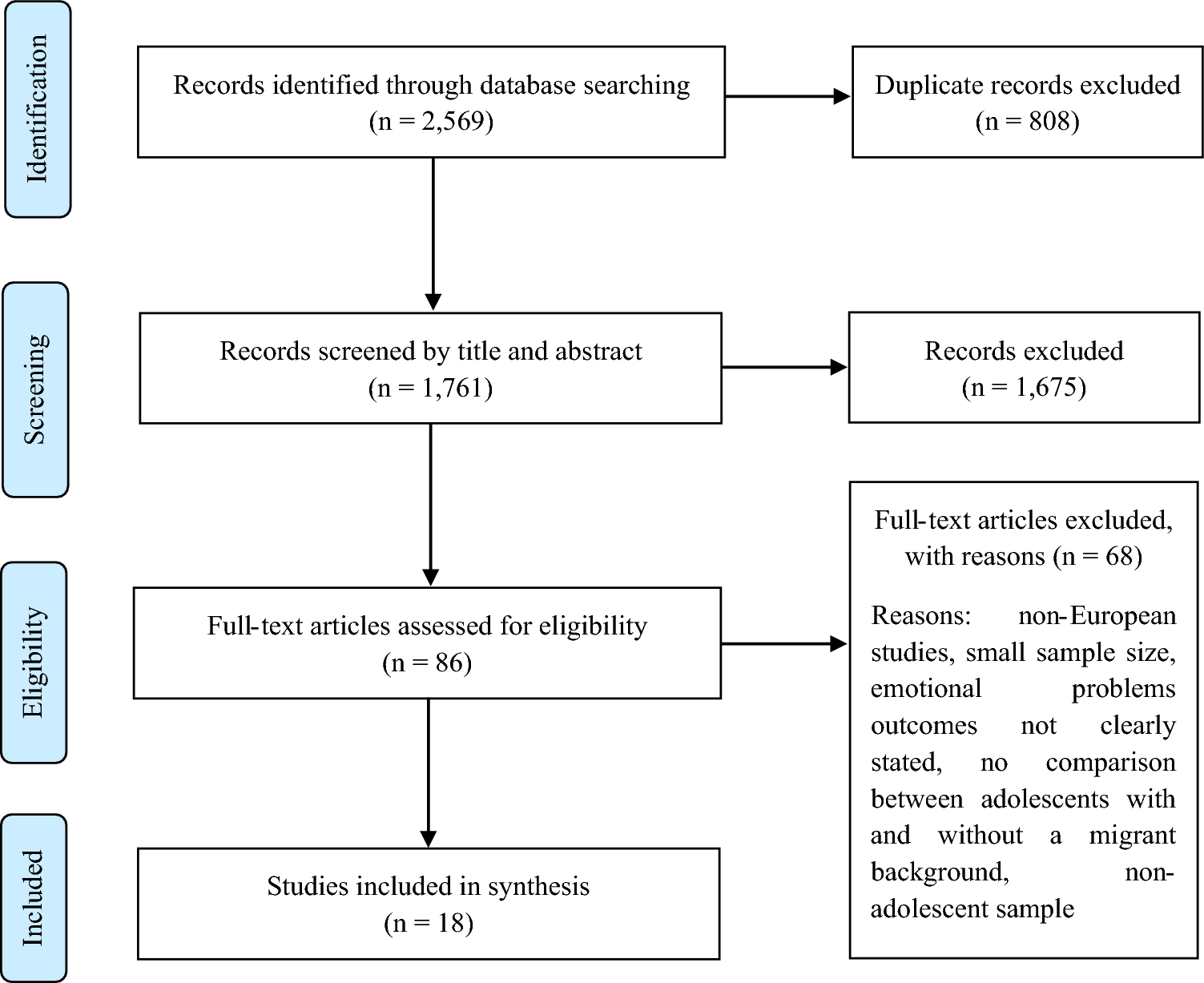
Overall, 86 adolescents were screened for eligibility across an overall study duration of five years and four months. Of these 86, 41 (48%) could not be included: 24 (28%) declined participation in the screening process, eleven (13%) were excluded in the screening process because there was no indication. Six (7%) were excluded due to other reasons (e.g., postponement of appointments by the adolescent until recruitment stop). Forty-five adolescents (52% of screened individuals) agreed to participate in the study. Three (3%) participants were randomized and referred to TAU before design change of the study; they were defined as study determined drop-out and are, thus, not considered for calculation of therapy adherence, acceptance of scientific assessments and pre–post analyses.
Of the remaining 42, four (10%) dropped out between diagnostic process and beginning of the intervention. Twenty-four (57%) completed the treatment. 14 (33%) dropped out during the intervention (for overview see flow diagram Fig. 1). Of these, eleven (79%), dropped out prior to or after the second individual session with their therapist.
Acceptance of scientific assessments
Acceptance of scientific assessments at a given timepoint was defined to be present when participants filled out at least one questionnaire at the respective timepoint. The number of adolescents and parents filling out at least one questionnaire is presented in ratio to the number of adolescents still participating in the study at the given timepoint: At T1 pre-treatment, questionnaires were filled out by 32 adolescents (84% of 38 treatment beginners) and 31 parents (82%). At T2 during treatment, questionnaires were filled out by 19 adolescents (76% of 25 still participating adolescents) and 13 parents (52%). At T3, questionnaires were filled out by 20 adolescents (83% of 24 completers) and 13 parents (54%). At T4, 6 adolescents (25% of the 24 completers) and 5 parents (21%) filled out the online questionnaires.
Treatment duration
Mean session number of completed treatments was 30.3 (SD = 15.2), with a range of eight to 69 individual sessions and zero to ten family sessions. Lowest numbers of individual sessions per treatment were eight (treatment duration: eight months), ten (treatment duration: seven months) and 12 (treatment duration: seven months). Highest numbers of individual sessions were 50 (treatment duration: 20 months), 56 (treatment duration: 23 months), and 69 (treatment duration: 26 months).
Qualitative treatment evaluations
Overall, 16 interview-based treatment evaluations were available for qualitative analysis (N = 10 in Heidelberg, N = 6 in Mainz). A detailed content analysis of treatment evaluations of the Heidelberg subsample published as a sub-analysis [22] revealed several positive aspects: adolescents liked, that they had someone who listened to and understood them. Therapy was deemed helpful for problem-solving and reflection. Mentalizing processes were named most often as important moments in therapy (e.g., gaining more self-control with increasing insight into inner states). While some adolescents indicated that their symptoms improved through therapy, some did not report changes through therapy, or attributed change to life-events or personal development. For some, the term mentalizing had some meaning (e.g., “understanding the other person’s emotions and behaviors and reacting correspondingly”). The psychoeducation was evaluated positively by half of the adolescents due to active involvement of their family or themselves; however, most did not remember the content. As negative aspects, adolescents most often reported that their therapists asked “too many questions”, which was “annoying”. Moreover, critique concerning the less structured phases of treatment was uttered especially by younger patients [22].
The six therapy evaluations from Mainz revealed a similar picture: Three reported they were satisfied with the treatment because it helped them fight less with their families, increase their insight into other people’s feelings, and reduce the urge to fight instead of seeking a solution for problems (e.g., “I learned to tell my friends I need a short break to calm down instead of quitting on them. This helped me not to lose them.”). Three indicated that they changed due to life-events and not therapy. Positive aspects included that therapists were more easy-going than therapists before, and that they could choose for themselves what they wanted to talk about rather than being told what to do. Negative aspects concerned the setting (having to come once a week) and “boring” diagnostic procedure. Similar to the Heidelberg sample, two adolescents did not remember the psychoeducation, and two indicated that they found it neither good nor bad. Three defined the word mentalizing as taking others’ perspectives; one said it was additionally about thinking about one’s own feelings. Most adolescents of both centers thought the scientific assessments were too long and they were annoyed by being asked “the same things twice”.
Organizational requirementsRecruitment potential per center, difficulties and study adaptations
In Heidelberg, 55 individuals were screened within 36 months of recruitment. Of those, eight did not fulfill participation criteria. Of 47 individuals potentially eligible, 29 (62%) were recruited for study participation. The mean overall recruitment rate per month was 0.9. Yet, monthly recruitment rates increased over the course of the study: During the first 24 months, 14 adolescents were recruited, i.e., recruitment rate was around 0.6 per month. At the time, parts of the diagnostic appointments were located in the child and youth psychiatry and part of it in the institute where the study was conducted. As a result, concurring studies were offered at the child and youth psychiatry, and changes in personnel and location seemed to confuse prospective participants. Moreover, participants recruited by the study institute reported reservations towards the child and youth psychiatry; and those recruited by the child and youth psychiatry reported reservations towards the study program as it was unfamiliar. Recruitment rates were lower than necessary for successful implementation of the RCT design. Consequently, the design was changed into a single-arm feasibility study, diagnostic appointments did not any longer include visits to the child and youth psychiatry and recruitment was stimulated again. In the third and last recruitment year in Heidelberg, 15 adolescents were recruited, i.e., the recruitment rate was doubled to around 1.3 per month.
In Mainz, 31 adolescents were screened within 16 months of recruitment. Of those, three adolescents did not fulfill participation criteria. Of 28 individuals potentially eligible for study participation, 16 (57%) were recruited for participation. The mean overall recruitment rate per month was one. Therapies in Mainz were conducted in the outpatient department of the child and adolescent psychiatry, so that in contrast to the Heidelberg study center, recruitment numbers likely benefitted from close connection to the child and adolescent psychiatry. Notably, eleven of the 16 recruited adolescents were included in the first seven months of recruitment from September 2019 to March 2020 up until the beginning of the first wave of the COVID-19-pandemic. In the last five months of recruitment from August to December 2020, five more adolescents were recruited, while from April to July 2020 none were included into the study. Thus, the number of potential participants in Mainz was likely reduced by the start of the pandemic in the middle of the recruitment phase.
Recruitment networks
Especially with study centers not directly connected to recruitment of a clinic, recruitment depended on a network. For the 29 participating adolescents in Heidelberg, nine (31%) were referred from community child services. For three (33%) of those, treatment was court ordered. Seven (24%) were referred from the child and youth psychiatry/general psychiatry. Three (10%) were referred from schools, three (10%) from therapists. Two (7%) came from youth centers or youth homes. One (3%) was referred from a health insurance company and one (3%) from peers familiar with the program. For three (10%) adolescents referral was not documented (recruited before design change). Of the 16 adolescents in Mainz, four were recruited from the inpatient (25%), eleven (69%) from the outpatient department of the child and adolescent psychiatry and one (6%) from an already participating sibling.
MBT adherence of therapists without prior MBT experience
Mean adherence of the 16 sessions was 4 (SD = 0.9), with scores between 2.8 and 5.4, i.e., in part below the threshold of being adherent (3.5, [17]). Nine (56%) of the 16 sessions were adherent. Three sessions (19%, conducted in Heidelberg) did not fulfill the “knock-out” criterion of the therapist displaying the not-knowing stance throughout the session. They could therefore not be labeled as MBT sessions. Four (25%) with scores below 3.5 were characterized by a strong focus on exploring behavior instead of mental states while still displaying great interpersonal warmth and developing the relationship (N = 2, 13%, conducted in Mainz), too little affect focus with MBT interventions not meeting the patient (N = 1, 6%, conducted in Mainz), and cognitive re-structuring coming along with a shortcoming in addressing non-mentalizing (N = 1, 6%, conducted in Mainz).
Organizational requirements for planning of a prospective RCT
An a priori sample size calculation was carried out in G*Power for a 2 (MBT-CD vs. control intervention) × 2 (pre vs. post treatment) mixed design analyzed with a repeated measures analysis of variance. Effect of interest was the between–within interaction effect; a small to medium effect size of f = 0.15 was expected [cmp. 8, 34]. Alpha level was set to 0.05, power to 0.80 and correlation amongst repeated measures to r = 0.5. The calculation resulted in a total sample size of N = 90. Calculated with 43% of drop-out observed in our study, 158 participants would be needed. Assuming a recruitment rate of 1.3 participant per month per, and a recruitment period of ~ 30 months, an effectiveness trial comparing MBT-CD with a control intervention would require at least four recruitment centers. Importantly, this calculation is based on the mean recruitment rate in Heidelberg when a recruitment network had already been established. When centers without an established recruitment network are included, a lower monthly recruitment rate should be considered.
Pilot pre–post analysisConduct disorder and oppositional defiant disorder diagnoses
At the end of treatment, 22 (92%) of 24 treatment completers attended a post treatment diagnostic session. Of those 22, 15 (68%) improved with regard to their diagnoses: 13 (59%) adolescents did not fulfill CD or ODD criteria anymore; for two (9%) adolescents, diagnosis was improved from CD to ODD. Seven (32%) still fulfilled criteria of CD or ODD, respectively (six with CD and one with ODD at T1).
Questionnaire data
Due to incomplete data and low sample size, questionnaire data were only drawn to for a pilot pre–post analysis. For 17 adolescents, complete data for the core measures at t1 and t3 were available. 95% confidence intervals of mean differences between pre- and post-treatment data did not indicate significant pre to post changes in aggression, mentalizing and personality pathology except for empathy pathology: The confidence interval of the mean difference between empathy pathology at t1 and t3 indicated a significant improvement of empathy (mean difference: 6.3, SD = 11.3, 95% CI [0.5; 12.2]; for overview of means, standard deviations, lower and upper bounds of the confidence intervals of mean differences for the whole sample and for each center, respectively, see Tables 1 and 2).
Table 1 Means (AM), standard deviations (SD) and the 95%-Confidence Interval (CI) of the pre to post differences of aggression, personality functioning and mentalizing of N = 17 adolescentsTable 2 Means (AM), standard deviations (SD) and the 95%-Confidence Interval (CI) of the pre to post differences of aggression, personality functioning and mentalizing of N = 8 adolescents in Heidelberg (upper half) and N = 9 adolescents in Mainz (lower half) 
留言 (0)