
記住我



Available online 24 November 2022
 Author links open overlay panelAbstract
Author links open overlay panelAbstractCurrent cholesterol guidelines for primary prevention of atherosclerotic cardiovascular disease (ASCVD) base statin treatment decisions on multiple risk factor algorithms (e.g., Pooled Cohort Equations [PCEs]). By available PCEs, most older middle-aged men are statin eligible. But several studies cast doubt on predictive accuracy of available PCEs for ASCVD risk assessment. Recent studies suggest that accuracy can be improved by measurement of coronary artery calcium (CAC). This method has the advantage of identifying men at low risk in whom statin therapy can be delayed for several years, provided they are monitored periodically for progression of CAC. Thus, there are two approaches to statin therapy in men ≥ 55 years: first all men could be treated routinely, or second, treatment can be based on the extent of coronary calcium. The latter could allow a sizable fraction of men to avoid treatment for several years or indefinitely. Whether with initial CAC scan or with periodic rescanning, a CAC score ≥ 100 Agatston units is high enough to warrant statin therapy. In otherwise high-risk men (e.g., diabetes, severe hypercholesterolemia, 10-year risk by PCE ≥ 20%), a statin is generally indicated without the need for CAC; but in special cases, CAC measurement may aid in treatment decisions.
Section snippetsPolypill Treatment: the Public Health ApproachThe positive results of primary prevention trials have led some investigators to advocate widespread use of statins in the general population6,7. This proposal is often presented as a polypill in which a statin is particularly attractive for middle-aged men, who as a group carry a relatively high risk for ASCVD. A statin is often combined with an anti-hypertensive agent and aspirin. One multinational RCT has tested the feasibility of the polypill concept8; it showed that statins are the
Polypill in Health Care SystemEven within the health-care system, long-term use of statins has been a challenge. As a general rule, the more liberal the use of statins, the greater will be the discontinuation rate. Moreover, many people often are treated unnecessarily because they will never develop ASCVD. The challenge is to identify those most likely to benefit from statin therapy, and among these, to maintain adherence. For example, statins may benefit only those with a particular form of high-risk atherosclerotic plaques
Guideline Based Primary PreventionA more targeted approach to primary prevention is to improve absolute risk estimates for cardiovascular events. This strategy was first developed by the Framingham Heart Study14, which consisted of a risk assessment tool based on multiple risk factors. It identified coronary heart disease (CHD) as the major endpoint. Framingham risk scoring was used in recommendations of the National Cholesterol Education Program (NCEP) as a guide to selection of cholesterol lowering drugs15.
In 2013 a still
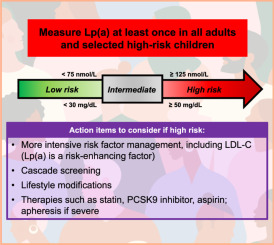
Risk Enhancing FactorsSince risk is uncertain for patients with 10-year risk estimated by PCEs of 7.5-<20% (intermediate risk), additional risk assessment may be informative. These risk factors (called risk enhancing factors) were proposed in 2018 guidelines17 to better define risk status of patients at intermediate risk. Risk enhancing factors included LDL-C ≥ 160 mg/dl (or non-HDL-C ≥ 190 mg/ld.), metabolic syndrome, chronic kidney disease, pre-eclampsia, premature menopause, high risk ethnicity, inflammatory
Coronary Artery CalciumAnother approach to selection of patients for statin therapy is based on severity of subclinical atherosclerosis (atherosclerosis burden)22. Major ASCVD events are more likely to occur in patients with significant atherosclerosis23. The most convenient way to identify subclinical atherosclerosis is by coronary artery calcium (CAC)24,25. Direct visualization of severity and character of atherosclerosis by angiographic means is too expensive and inconvenient for routine clinical use. Also, the
Routine CAC in Women Who Are Statin Eligible by PCEsIn a recent report5, we explored the pros and cons of routine measurement of CAC in women of middle age who are statin eligible by PCEs. Many such women will have zero CAC or CAC 1-99 Agatston units and hence can delay statin therapy for several years before CAC re-scanning. For this reason, we proposed that statin therapy not be initiated unless indicated by CAC scanning. In women with categorical high-risk, statin eligibility is assumed without further risk assessment5,17.
CAC Measurement in MenAtherosclerosis develops more rapidly in men than in women35. On average, atherosclerosis in men occurs about a decade before that of women. This means that more middle-aged men (40-75 years) will become statin eligible before women of the same age. The question being addressed here is whether CAC measurement in men will improve the selection for statin therapy as it does in women.
Figure 1 compares 10-year risk estimates by middle age decades in men of NHANES by PCEs (Figure 1A) (NHANES
Implications of CAC Scanning for Statin Therapy in MenMen 45-54 years. As shown in Figure 1, in the decade of 45 to 54 years, the risk patterns by PCEs and CAC were similar. By PCEs, 53% are low risk; 22% are borderline risk; and 27% have 10-year risk ≥ 7.5% (statin eligible). By CAC, 62% have zero CAC; 21% have CAC 1-99 Agatston units; and 17% have ≥ 100 Agatston units.
In this age range, men at low risk by PCEs have no need for immediate CAC scanning. At borderline risk by PCEs, CAC scanning for men is optional. At 10-year risk ≥7.5% by PCEs, CAC
Categorical High Risk in MenCholesterol guidelines17 recommend statin therapy in most patients with high-risk so that CAC scanning is unnecessary. Nonetheless, measuring CAC is an option. MESA studies have shown that a sizable portion of patients with diabetes41, severe hypercholesterolemia42, and high 10-year risk for ASCVD43, called categorical high risk, carry a sizable portion with zero CAC. Therefore, if CAC is measured and found to be negative, statin therapy can be delayed provided CAC re-scanning is carried out in
Coronary Calcium as Statin Adherence MotivatorLong term adherence rates for statins is a major impediment for achieving full benefit.
One view holds that visualization of atherosclerotic plaques may be a motivating factor to support compliance with statins. Several reports address the potential motivation that can be derived for the finding of significant CAC accumulation38, 46, 47, 48. These promising findings justify further studies to verify benefit.
Strategies for Statin IntoleranceMultiple factors contribute to long term discontinuation of statin therapy49. Much of this is due to flaws in the health care system. Overall, about 10% of all patients claim statin intolerance, most of which are the result of muscle symptoms–myalgia or muscle weakness. Statin intolerance is best treated but switching to another statin or by reducing the dose. Some patients are able to tolerate cutting the dose in half and adding ezetimibe plus maximizing lifestyle changes.
ConclusionsMen develop atherosclerosis more rapidly than women. RCTs show that statin therapy reduces risk significantly in middle aged men who have ASCVD risk factors. According to NHANES data, these include most men over age 55 years. Therefore, one option is to start routine statin therapy in most older, middle aged American men without the need for further risk assessment. On the other hand, a more targeted approach would be to measure CAC in all middle aged men and to start a statin only in those
ContributionsEach author made substantial contributions to1 the conception and design of the study,2 the acquisition of data, analysis, and interpretation of data,3 drafting the article or revising it critically for important intellectual content, and4 final approval of the version to be submitted.
SupportThis work was not supported by a specific grant.
Declarations of InterestNone
View full text© 2022 Published by Elsevier Inc. on behalf of National Lipid Association.
留言 (0)