
記住我
The data used in the present study were based on the Finnish Prenatal Study of Anxiety disorders (FIPS-Anx), which is an epidemiological study that uses a nationwide population-based sample [31]. The FIPS-Anx uses register-based information to examine the association between early developmental factors and family histories of various anxiety disorders.
The cohort for the current study comprised all singleton children born in Finland between 1 January 1987 and 30 March 2009, who were diagnosed with SM between 1 January 1998 and 31 December 2012. The full siblings were born between 1 January 1977 and 31 December 2012, and diagnoses given after 1 January 1996 were included. Subjects, controls and their respective siblings and parents were observed until 31 December 2016 and all mental disorder diagnoses that were registered during the observation years were collected. ICD-10 was in use in Finland at the time of the study. The start date of 1998 was chosen because that was the earliest date when both inpatient and outpatient data were available in the relevant registers.
The data were collected from three nationwide Finnish registers: The Finnish Hospital Discharge Register (Discharge Register), The Finnish Central Population Register (Population Register) and The Finnish Medical Birth Register (Birth Register).
The Discharge Register was established in 1969 and includes information on all mental disorders diagnosed delivered by specialized health care services. It covers all public specialized health care inpatient care units since 1969 and all outpatient units since 1998. This means that all the diagnoses delivered to subjects included in the present study during the observation years were obtained. These comprised the subjects with SM and the controls and their siblings and parents. In Finland, all diagnoses were based on ICD-9 [32] from 1987 to 1995 and on ICD-10 [2] from 1996 onwards.
The Birth Register provides data on children with SM, and their mothers, during pregnancy and delivery. The Register includes information on all live births in Finland since 1987 and the coverage is estimated to be 100% [33]. It was also used to identify controls, and their mothers, and to obtain the data on covariates, including maternal socioeconomic status (SES) and maternal age and marital status during the delivery.
The Population Register is maintained by the Finnish Population Center and local register offices. It contains personal information on all Finnish citizens, such as their name, family members and address, and was used to identify the fathers and full siblings of the subjects and controls. Information on paternal age was also obtained from this Register.
The data collected from the different registers were linked using the personal identity codes that are issued to all Finnish residents at birth or when they become permanent citizens after immigration. The study was approved by the Ethical Committee of the Hospital District of Southwest Finland.
Subjects and their controlsAll the children with SM were registered with the ICD-10 code F94.0 and matched with four controls by their birth date (± 30 days) and sex. The study included subjects who were diagnosed at least once from 3 to 15 years of age. The exclusion criteria for the subjects and controls were coexisting ASD (ICD-10 F84.0-0.9, ICD-9 229), psychotic disorders (ICD-10 F20-25, F28-29, ICD-9 295, 297, 2989X, 3012C) and a moderate or severe intellectual disability (ICD-10 F72-73, ICD-9: 318). The data used in the present study were derived from the larger FIPS-Anx sample, which had excluded controls with anxiety and childhood emotional disorders when the data were originally extracted from the national registers (ICD-10 codes F40–42, F43.0, F43.1, F43.22, F43.23 and F93-94). These categories do not include depressive disorders. This procedure ensured that the controls did not have any of the disorders that were being studied. However, some controls were subsequently diagnosed with these conditions during the observation period that followed the original data extraction. If this happened, they were excluded in line with the original criteria [31].
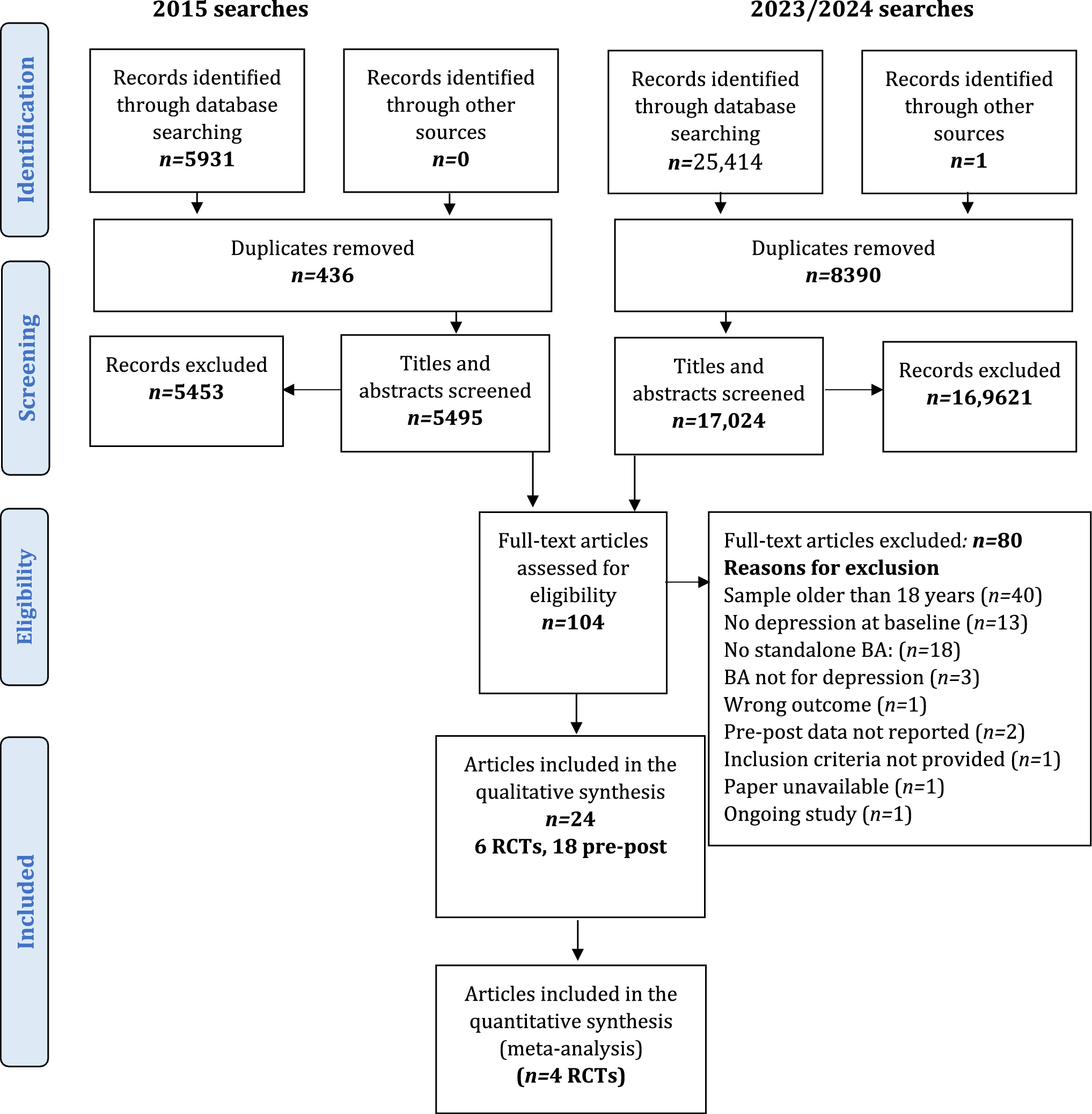
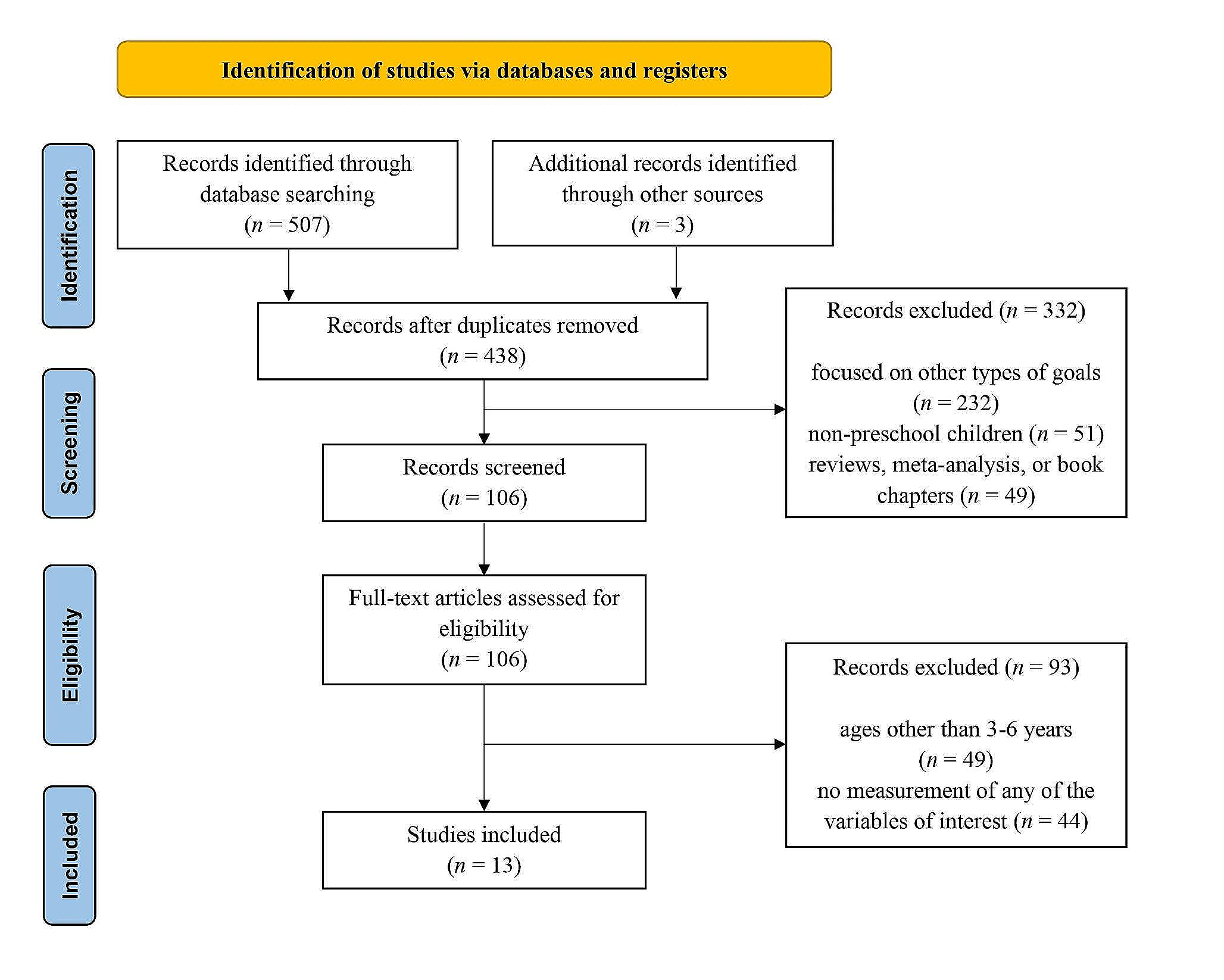
Identifying the siblingsFull siblings of the subjects with SM and the controls were identified from the Population Register. A flow chart of the sample selection is shown in Fig. 1. This shows that the siblings were born between 1 January 1977 and 31 December 2012 and mental disorder and neurodevelopmental diagnoses from 1 January 1996 to 31 December 2016 were included. Siblings born before 1977 or after 2012 were excluded to ensure that there had been sufficient observation time when ICD-10 was used in Finland. Siblings who had died or emigrated before the age of three, or had moved to Finland after age of three, were excluded. Complete matched sets of subjects and controls were included if the subject, and at least one control, had one full sibling or more. We did not exclude siblings who had been diagnosed with SM because we were also interested in examining SM among the siblings, as these studies are scarce. The significance of this dependence was assumed to be low and, to control for this, the unit in each of the analyses was the sibling. A similar approach has also been used in other sibling studies, including those on subjects with attention deficit hyperactivity disorder (ADHD) and ASD [18, 19]. Thus, a total of 658 children with SM with 1697 siblings and 2092 controls with 4211 siblings were included in the final analyses.
Fig. 1
Selection of the study population
Diagnoses among siblingsFirst, we established if any of the siblings in the SM and control groups had mental disorders and this was scored as a yes if there was at least one sibling diagnosed with a mental or neurodevelopmental disorder. These siblings were then assigned to the main diagnostic categories based on their ICD-10 diagnoses (Supplementary Table 1). Due to strong associations between SM and anxiety disorders, various anxiety diagnoses were analyzed separately (Supplementary Table 2). If a sibling had received some of the diagnoses in a category at least once during the observation period, they were assigned to that category. If there were co-occurring disorders, the subject was separately assigned to each category. If the diagnosis was given to the sibling multiple times, only the first diagnosis was considered. This means that we have reported the incidence rates, not the number of diagnoses.
CovariatesA series of potential covariates were included in the analyses, based on the findings of various studies, namely, maternal SES [11, 34], maternal mental disorder diagnoses [11, 12, 35], paternal mental disorder diagnoses [14, 15, 36], maternal and paternal age [37] and maternal marital status [11, 38, 39]. Maternal SES was divided into four categories, based on occupational class, namely upper white collar, lower white collar, blue collar and other [40]. Maternal SES has been shown to be a strong indicator of health inequality in Finland [41]. Maternal SES was only registered for subjects born from 1991 onwards, as it had not been recorded before that point. Maternal and paternal mental disorder diagnoses were used as a variable to describe how many different mental disorder diagnoses parents had received during the observation period. Parental age was used as a continuous variable. Complete data were available for maternal and paternal mental disorder diagnoses and age. Maternal marital status was classified as single or as married or cohabiting. Marital status and maternal SES are provided direct to the register and this means that missing information, due to lack of reporting, was possible.
Maternal SES, maternal marital status and parental age were all obtained during the birth of the subject. Parental mental disorder diagnoses were collected from 1 January 1987 until the end of observation period on 31 December 2016.
Statistical analysesThe number of siblings that the subjects and controls had were compared with Fisher’s exact test, using a Monte Carlo simulation approach. Any interaction between the sex of the subjects and the outcome was tested using the Joint test. Regression models were used to estimate the associations between subjects with SM and siblings with mental and neurodevelopmental disorders. Associations between exposure and outcomes, namely selective mutism in subjects and mental disorder categories in siblings, were estimated separately. The unit of analysis was the siblings. Generalized estimating equations (GEE) for logistic regression models were used to account for matching between the subjects and controls and their siblings. Each stratum included the siblings of one child with SM and the siblings of their matched controls. Observation years were used as an offset in all models, as siblings were observed for different lengths of time. The associations between children with SM and the outcomes in their siblings are reported as odds ratios (ORs) with 95% confidence intervals (CIs). P-values were calculated using Pearson’s chi-square test and values of less than 0.05 were considered statistically significant. The statistical analyses were performed with SAS software version 9.4 (SAS Institute Inc, Cary, NC, USA).
Associations between mental disorders in the siblings and covariates were tested with Pearson’s chi-square test and those with P-values of less than 0.1 were added as covariates to Model 2, which was conducted for coherent data. In the final model, namely Model 3, comorbid diagnoses among subjects with SM were used as covariates, along with the previously used covariates. Comorbidity was used as a dichotomous variable (yes/no) and the subjects with SM were placed in the yes category if they had received any comorbid diagnosis at least once.
This means that there were three models conducted. Model 1 was unadjusted. Model 2 was based on Model 1 and adjusted for significant covariates, which were chosen based on the covariate analyses. In the final model, Model 3, the results were adjusted by the comorbid diagnoses of the subjects with SM and by the covariates chosen based on the covariate analyses.
In addition, we conducted sensitivity analyses on siblings in the SM group who were born between 1 January 1995 and 31 December 2009, to see whether possible changes in the methods of registration during observation years affected the results. These included adding outpatient diagnoses and possible changes in clinical practice due to increased knowledge about SM. Unadjusted analyses were conducted on this subgroup using GEE and the results were compared to the complete data to check whether the same diagnostic categories remained significant.
In addition, sensitivity analyses were conducted for the subgroup of siblings of the subjects with SM that had not been diagnosed with anxiety disorders or childhood emotional disorders. These were then compared to the siblings of their matched controls. These analyses were conducted to examine whether the results were representative, due to excluding these disorders among the controls. Similarly, unadjusted analyses were conducted, and the results were compared to the results from the complete data.
Subjects with ASD, psychotic disorders or moderate or severe mental disability were excluded, because they could not be reliably diagnosed with SM according to ICD-10. However, to explore if there were selective drop-outs due to this exclusion, the characteristics of this excluded group were compared to the complete data. P-values were calculated using Pearson’s chi-square test.
留言 (0)