
記住我






This was a randomized, controlled trial. The study protocol was approved by the Ethics Committee of Peking University Hospital of Stomatology, Beijing, China on 01/29/2022 (No. PKUSSIRB-202272018) and registered with ClinicalTrials.gov on 02/01/2022 (NCT05218590). The study was conducted in the Peking University Hospital of Stomatology in accordance with CONSORT guidelines. Written informed consent was obtained from each participant. All methods were performed in accordance with the Helsinki Declaration and relevant clinical trial management regulations of China.
ParticipantsDuring a preoperative visit, we asked patients to occlude the contralateral nostril in the sitting position to self-assess nasal airflow. This method has been verified as useful and accurate for assessing nostril selection for nasotracheal intubation [10]. Patients who were able to breathe clearly and equally through both nostrils were invited to participate in the study. Other inclusion criteria were adult patients aged 18 to 80, American Society of Anesthesiologists (ASA) physical classification I to II, scheduled to undergo elective oral and maxillofacial surgery that required nasotracheal intubation and was expected to last less than 3 hours, and surgery that was anticipated to have extubation performed in the operating room and would not require preventive tracheotomy.
Patients were excluded for the following: (1) history of, or presented with, an anticipated difficult airway. We assessed the airway mainly according to the difficult airway management guidelines of Chinese Society of Anesthesiology [11], which includes predictors of Modified Mallampati classification (III- IV), inter-incisor gap (< 3 cm), thyromental distance (< 6 cm), mandible luxation, head and neck movement, as well as previous history of difficult intubation, and presence of pathologies associated with difficult intubation; (2) required insertion of nasogastric tube; (3) contraindications of nasotracheal intubation; (4) intubation through one nostril due to surgical requirement; (5) presence of severe nasal obstruction, deformities of the nasal cavity, or other serious nasal diseases. Severe nasal obstruction and history of nasal diseases was subjectively reported by the patients themselves. During the preoperative visit, patients were asked if they had difficulty breathing through their nose and/or history of nasal diseases diagnosed by a specialist. All screened patients underwent panoramic radiography, and/or craniomaxillofacial spiral computed tomography (CT), and/or cone-beam CT. Anesthesiologists and maxillofacial surgeons reviewed these radiographs before surgery; (6) history of epistaxis within a month; (7) previous history of nasotracheal intubation, or nasal or laryngeal surgery; (8) language barrier or history of Parkinson disease, dementia, schizophrenia; (9) refusal to sign consent; (10) participated in other clinical studies.
Randomization and blindingRandom numbers were produced by the SPSS 21.0 software package (IBM SPSS Inc., Armonk, NY, USA) in a 1:1 ratio by an independent biostatistician and sealed in opaque envelopes. The envelopes were sequentially numbered and opened just prior to anesthesia by an anesthesia nurse who did not participate in the rest of the study. Patients were assigned to nasal intubation through either the left or right nostril (right nostril, Group R; left nostril, Group L). In our study, all intubations were performed using a video rigid stylet (Insight iS3, Shenzhen Insighters Medical Technology, Shenzhen, China), which was patented and approved for human use in 2016 (Fig. 1A). This video stylet has a J-shaped stylet with an adjustable semirigid distal portion. It contains a light source and camera at the distal tip and a color display screen. After intubation, the envelopes were sealed again until the end of the trial. During anesthesia, independent care providers who did not participate in the rest of the study recorded relevant data. The outcome assessors were blinded to the study group assignments. However, it was not possible for the anesthesiologists who performed the intubations to be blinded to the group allocation.
Fig. 1
Video rigid stylet and nasotracheal tube. A Video rigid stylet; (B) preformed double-curved nasotracheal tube; (C) before intubation, the nasotracheal tube is preloaded onto the stylet; (D) to intubate, the operator’s right hand holds the handle and the left hand threads the stylet-tube assembly into the nostril
Anesthesia and intubationNo premedication was given in the general ward. Routine intraoperative monitoring included noninvasive blood pressure, pulse oxygen saturation (SpO2), electrocardiogram, oxygen and end-tidal concentration of carbon dioxide, inhalational anesthetic concentration.
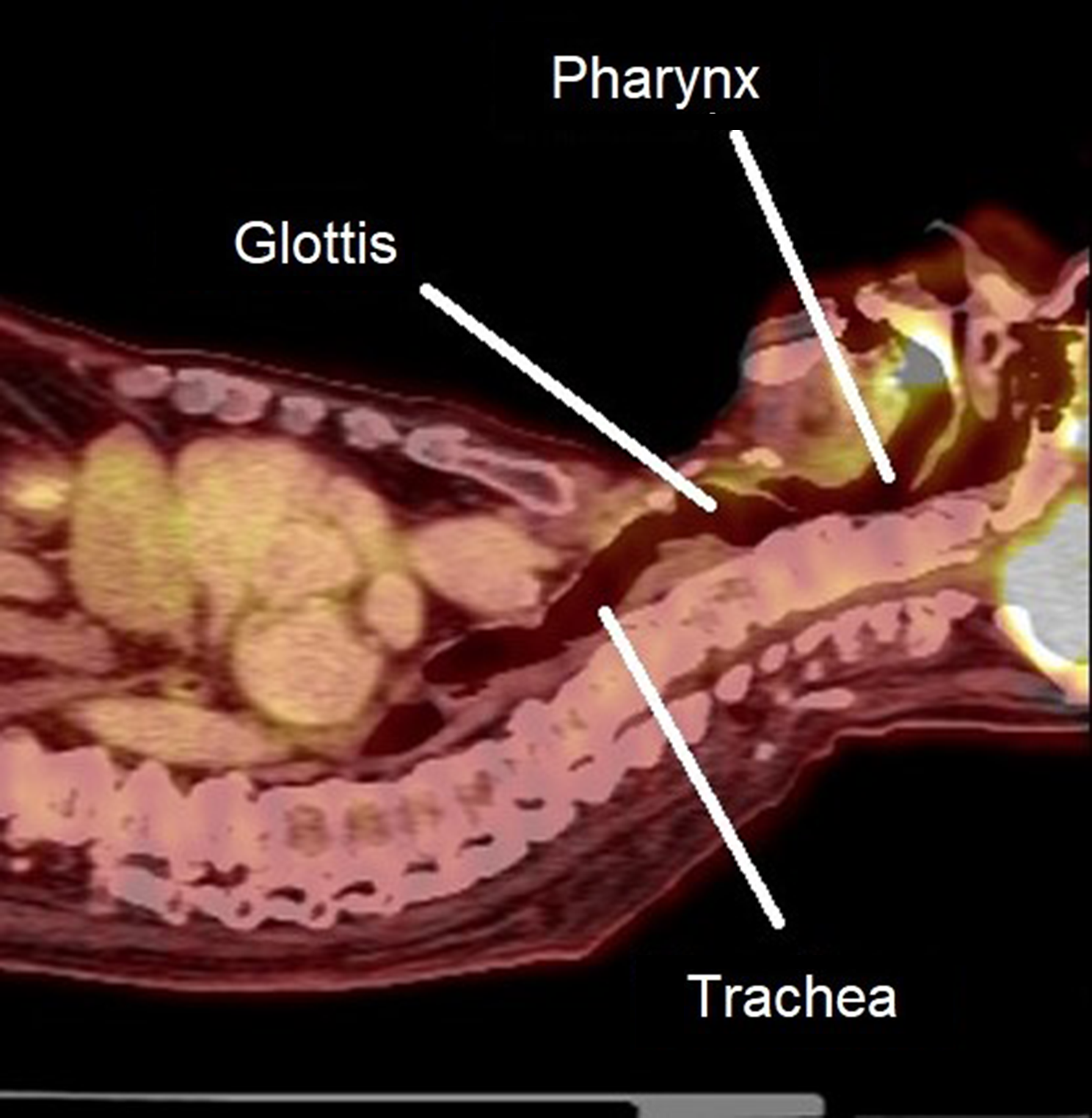
Before general anesthesia induction, midazolam and/or dexamethasone were administered intravenously at the discretion of attending anesthesiologist. Anesthesia was induced with sufentanil/remifentanil, propofol/etomidate, and rocuronium/cis-atracurium. Before intubation, topical epinephrine (1:200,000) was applied in the selected nostril. Nasotracheal intubation was achieved using a preformed double-curved nasotracheal tube (Shiley Nasal RAE, Medtronic; Minneapolis, MN, USA) (Fig. 1B), 6.5 mm ID and 7.0 mm ID for female and male patients, respectively. For intubation with the video rigid stylet, an endotracheal tube was lubricated and mounted onto the stylet (Fig. 1C). The operator’s right hand held the handle of the video stylet and the left hand threaded the stylet-tube assembly through the nostril. The patient’s chin was stabilized by the fingers of operator’s left hand (Fig. 1D). The stylet-tube assembly was then inserted into the selected nostril and advanced into the nasal cavity, the nasopharynx, and the oropharynx. After the glottis was exposed and the assembly approached or entered the glottis, the preloaded tube was advanced over the stylet into the trachea (Fig. 2). Successful intubation was confirmed using capnography. General anesthesia was maintained with intravenous infusion of propofol, remifentanil, or inhalational sevoflurane. After surgery, patients were extubated in the operating room.
Fig. 2
Route of video rigid stylet-guided nasotracheal intubation
All intubations were performed by experienced anesthesiologists, who had more than 10 years of experience and had performed hundreds of nasotracheal intubations using video or optical stylets.
Data collection and outcome assessmentBaseline data included demographic and morphometric characteristics, surgical diagnosis, laboratory workup results, and airway evaluation indicators. Intraoperative data included hemodynamic parameters during intubation, duration of surgery and anesthesia, types and doses of anesthetics, and fluid balance.
Primary outcome was the total time for intubation, defined as the time interval from when the tip of stylet-tube assembly entered the selected nostril to when the tube entered the trachea. Secondary outcomes included: (1) the time for stylet-tube assembly insertion, defined as the time interval from when the tip of the stylet-tube assembly entered the selected nostril to when it accessed the glottis; (2) the time for tube insertion, defined as the time interval from when the stylet-tube assembly accessed the glottis to when the tube was confirmed inserted into the trachea; (3) total success rate; (4) first-attempt success rate; (5) number of intubation-attempts; (6) requirement of airway-assisted maneuvers; (7) incidence and severity of epistaxis. After confirming the location of the tube, an investigator used a fiberoptic bronchoscope to examine the shell of the tube and then examine the posterior pharyngeal wall through the other nostril. No epistaxis was defined as absence of blood on the external surface of the tube and the posterior pharyngeal wall; mild epistaxis was defined as blood observed on the exterior of the tube or posterior pharyngeal wall; moderate epistaxis was defined as pooling of blood on the posterior pharyngeal wall; severe epistaxis was defined as a large amount of blood in the pharynx impeding nasotracheal intubation and necessitating urgent orotracheal intubation [12].
Intubation-related adverse events were monitored for up to postoperative 24 h.
Statistical analysisSample size estimationThe primary hypothesis was that the length of time for nasotracheal intubation differs significantly between the two nostrils. A previous study of patients in our center showed the mean (standard deviation (SD)) duration for nasotracheal intubation using an optical rigid stylet was 27 (3) seconds [13]. In that study, the choice of nostril for intubation was based only on the preference of the anesthesiologist (some patients were intubated through the left and others through the right nostril). Theoretically, this intubation duration should be longer than that through the more suitable nostril. Hence, we defined 27 ± 3 seconds as the time required to complete the intubation through the more suitable nostril. The sample size required to detect 10% of changes in intubation time, at a significance level of 0.05 and a power of 90%, is at least 22 patients per group. Thus, we enrolled 25 patients per group. Sample size was calculated with PASS 11.0 software (NCSS Statistical Software, East Kaysville, UT, USA).
Data analysisData with or without normal distribution were expressed as mean ± SD or median and interquartile range (IQR). Categorical data were presented as a number (%).
For baseline and intraoperative data, quantitative data were compared with t-test or Mann-Whitney U test; qualitative data were compared with chi-square test with or without Yates correction, or Fisher’s exact test. Repeatedly measured variables (hemodynamic parameters and SpO2) were compared with the general linear model.
Our primary outcome, the total length of time of intubation, was compared with Mann-Whitney U test, with differences between groups expressed as median difference and 95% confidence interval (CI).
For secondary outcomes, quantitative data were compared with t-test or Mann-Whitney U test. Qualitative data were compared with chi-square test with or without Yates correction, or Fisher’s exact test. The difference between groups was quantified as the risk ratio (RR), median difference, or mean difference and 95% CI. Safety outcomes were compared with chi-square test with or without Yates correction, or Fisher’s exact test.
A two-tailed P < 0.05 was regarded as statistically significant. Statistical analysis was performed with the SPSS 21.0 software package (IBM SPSS Inc., Armonk, NY, USA).
留言 (0)