
記住我


KEY POINTS
Question: Can Diprospan with ropivacaine, compared to ropivacaine alone, reduce opioid consumption after craniotomy? Finding: Diprospan as a ropivacaine adjuvant to preemptive scalp infiltration analgesia decreased 33 µg (87%) of analgesic consumption within 48 hours postoperatively. Meaning: Diprospan and ropivacaine preemptive scalp infiltration is an effective technique for postoperative analgesia after craniotomy.Many sources suggest that patients undergoing craniotomy experience significant postoperative pain. A prospective study showed that up to 80% of patients experience mild to severe pain in the acute postoperative period.1 Another study revealed that two-thirds of patients undergoing major elective intracranial surgery experience moderate to severe pain for the first 2 days after surgery.2 The consequence of inadequate analgesia can be significant and include arterial hypertension, cerebral hyperemia, edema, hemorrhage, and so on.3–6 Moreover, acute pain after craniotomy is associated with an increased risk of chronic pain.1 However, recent surveys and expert opinion emphasize that postcraniotomy pain continues to be undertreated.1 Therefore, postoperative pain control should be a priority for neurosurgical patients.7
In recent years, local infiltration of analgesia has been widely performed clinically, is regarded as a promising analgesic method that can avoid most of the side effects of systemic drugs,8 and can also be administered preemptively before incision.9 Despite the addition of adrenaline, preemptive incision-site infiltration with local anesthetics can only provide a relatively satisfactory analgesic effect that lasts for a short time preoperatively. However, pain after craniotomy continues through the second to seventh days.10 Therefore, it is necessary to explore other compatible drugs with longer duration of action and stronger analgesic effects.11
Incisional pain leads to the release of inflammatory mediators after tissue damage12; therefore, reducing incisional inflammation could become an effective strategy to control incisional pain. Our research group has previously established that preoperative incision-site infiltration with dexamethasone, which possesses an anti-inflammatory effect, along with ropivacaine, a local anesthetic, has a better postoperative analgesic effect than ropivacaine alone in craniotomy patients; however, the effect was limited.13,14 Yavari et al15 report that, during 24 to 72 hours after endodontic treatment of vital teeth, the analgesic effect of infiltration of dexamethasone and long-acting (LA) betamethasone was the same, but dexamethasone had a better effect in the first 24 hours, and the analgesic effect of LA betamethasone can last up to 7 days. Diprospan is a combination of quick-acting betamethasone sodium phosphate and LA betamethasone dipropionate.16 Compared with LA betamethasone, the onset of action of Diprospan begins in a shorter time.17 However, whether Diprospan as an adjuvant to local anesthetics can also achieve postoperative pain relief after craniotomy has not been determined yet. Hence, we performed this detailed study to assess the treatment effect of preemptive incision-site infiltration of ropivacaine plus Diprospan (versus ropivacaine alone) on postoperative analgesia for patients undergoing craniotomy.
METHODS Study Design and SettingsThis is a prospective, single-center, blinded, randomized, controlled clinical study. The study protocol was approved by the Ethics Committee of Beijing Tiantan Hospital, Capital Medical University (reference no. KY 2018-034-02-3) and registered before patient enrollment at ClinicalTrials.gov (NCT 04073069; principal investigator: Fang Luo; date of registration: August 27, 2019). The study was conducted at Beijing Tiantan Hospital. Patient recruitment extended from September 3, 2019, to August 15, 2020. The final follow-up was completed on February 15, 2021.
Patient PopulationAfter signing the written informed consent, patients who met the following criteria and did not meet any of the listed exclusion criteria were recruited. Patients were taught how to indicate postoperative pain based on the numerical rating scale (NRS). Patients were also taught how to use the patient-controlled analgesia (PCA) device.
Inclusion criteria
Age 18 to 64 years. Participants who were scheduled for elective supratentorial craniotomy. American Society of Anaesthesiologists (ASA) physical status of I, II, or III. Patients undergoing intraoperative pin fixation of the head. Patients with an anticipated full awakening from general anesthesia within 2 hours postoperatively.Exclusion criteria
History of craniotomy. Active psychiatric disorders. Uncontrolled epilepsy. Chronic headache. Preoperative Glasgow Coma Scale <15. Suspected intracranial hypertension. Peri-incisional infection. Symptomatic cardiopulmonary, renal, liver dysfunction, or history of diabetes. High probability of having postoperative radiotherapy or chemotherapy. No plan to extubate or expected delayed extubation. Allergy to opioids, Diprospan, or ropivacaine. Chronic opioid use (>2 weeks) or history of excessive alcohol or drug abuse. Inability to understand the use of NRS or PCA device. Extreme body mass index (BMI) (<15 or >35 kg/cm2). Pregnant or breastfeeding.Withdrawal criteria
Not awake 2 hours after surgery. Delayed extubation. Early revision within the first 48 hours. Voluntary withdrawal. Received radiation therapy and chemotherapy postoperatively. Randomization and BlindingThe allocation sequence was generated using simple randomization by Statistical Package for the Social Sciences (SPSS) version 25.0 (International Business Machines Inc) by an independent researcher before the inclusion of the first participant. A fixed value was set for random number generators, and allocation sequence was reproducible. No block was used in the allocation scheme. Eligible patients were randomly assigned to the Diprospan group or the control group with a distribution ratio of 1:1. Patients and the independent researcher responsible for postoperative follow-up were blinded to allocation. Neurosurgeons and anesthesiologists were unable to be blinded in this study because macroscopic differences are created through the preparation of local infiltration mixtures. However, neurosurgeons and anesthesiologists were given clear instructions not to disclose allocation while interviewing participants.
ProceduresLocal infiltration solution was prepared by an independent researcher as follows: 0.5-mL Diprospan (Diprospan betamethasone 1 mL, propionate 5 mg, and betamethasone sodium phosphate 2 mg) and 15 mL of 1% ropivacaine, diluted to a total volume of 30 mL in normal saline for the Diprospan group, and 15 mL of 1% ropivacaine diluted to a total volume of 30 mL in normal saline for the control group.
Standard monitoring such as blood pressure, heart rate, peripheral pulse oximetry, and electrocardiography was established. Intravenous midazolam 0.03 mg/kg, 0.3- to 0.4-μg/kg sufentanil, 1.5- to 2-mg/kg propofol, and 0.2-mg/kg cisatracurium or 0.6-mg/kg rocuronium were used for standard induction of anesthesia. An endotracheal tube was placed to facilitate mechanical ventilation. Anesthesia was maintained with 4- to 8-mg/kg/h propofol and 0.1- to 0.3-µg/kg/min remifentanil intravenously. Anesthesiologists adjusted the remifentanil infusion dose to maintain the mean arterial pressure and heart rate fluctuations within a 20% range of baseline, and no additional analgesics were administered intraoperatively.
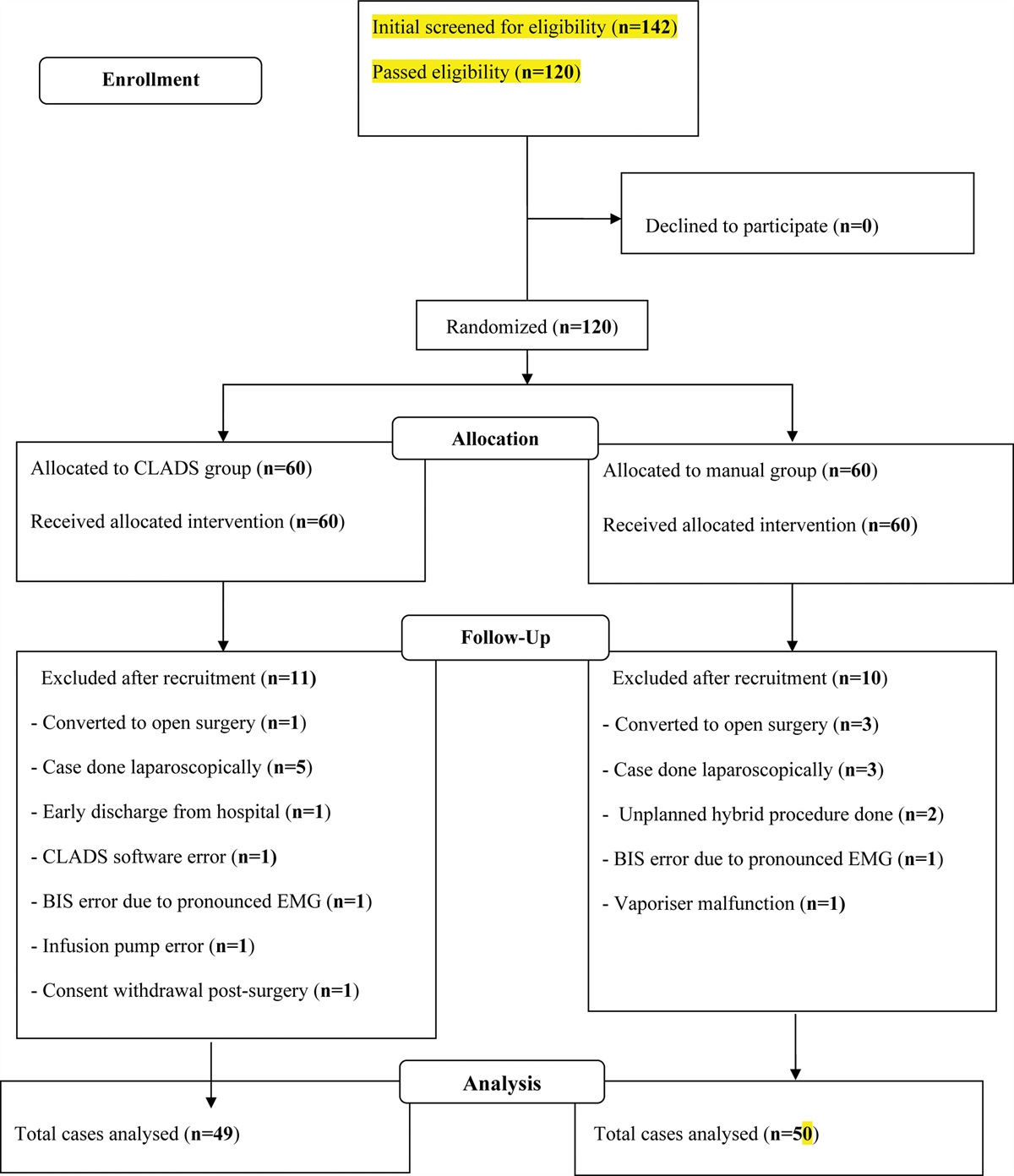
 Figure 1.:
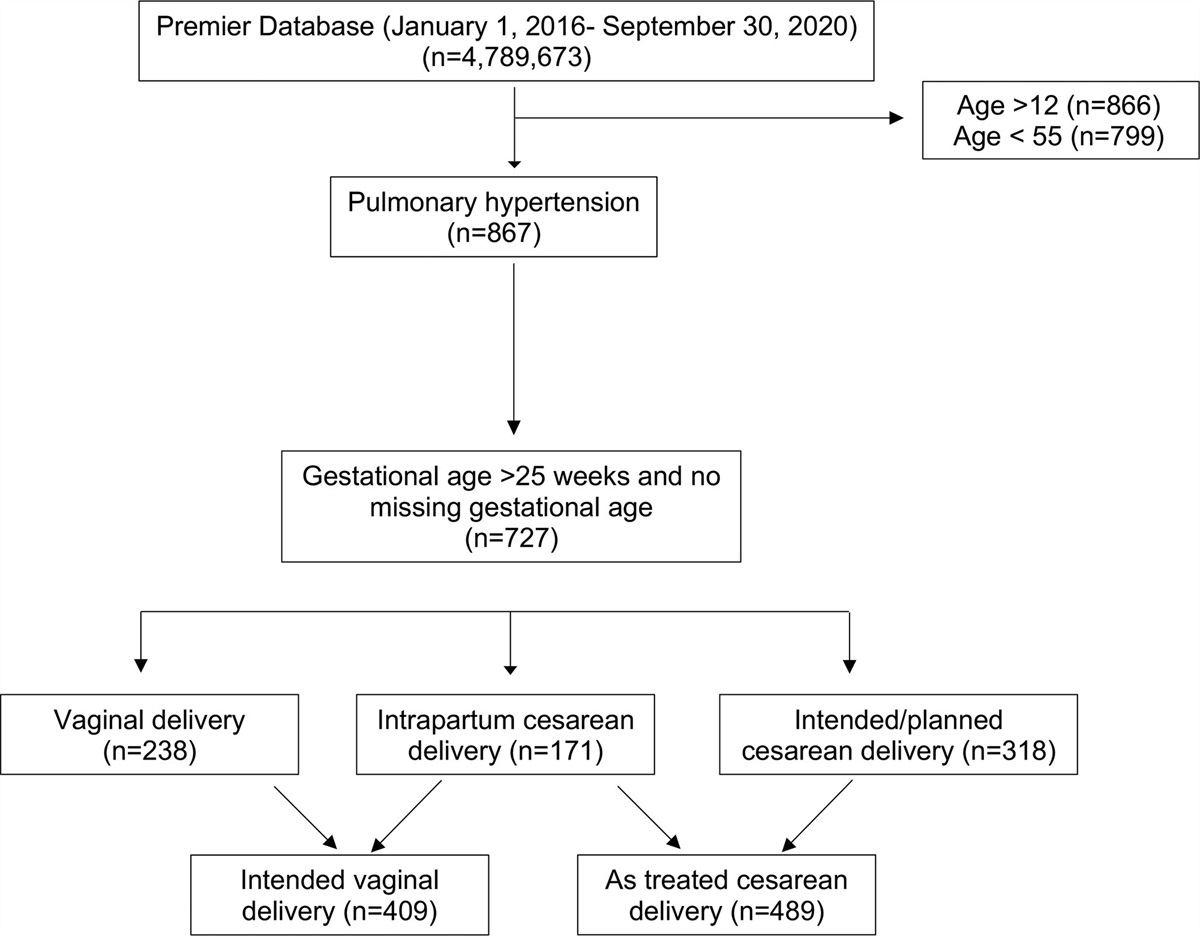
Figure 1.: CONSORT study diagram. CONSORT indicates Consolidated Standards of Reporting Trials.
Table 1. - Patient Characteristics and Intraoperative Data Factor Diprospan (n = 48) Control (n = 48) Standardized Difference Age, y 45.1 ± 13.1 47.0 ± 11.8 −0.15 BMI, kg/m2 24.6 ± 3.7 23.7 ± 3.4 0.26 Tumor size, cm 4.2 ± 1.6 4.2 ± 1.3 −0.03 Length of incision, cm 17.3 ± 2.2 17.4 ± 2.4 −0.03 Female sex 17 (35) 18 (38) −0.04 ASA status 0.02 I 18 (38) 17 (35) II 19 (40) 22 (46) III 11 (23) 9 (19) Location of scalp 0.30 Frontal 22 (46) 17 (35) Temporal 5 (10) 9 (19) Frontotemporal 9 (19) 9 (19) Parietal 5 (10) 4 (8) Other 7 (15) 9 (19)Values are mean ± SD for continuous variables and n (%) for categorical or ordinal. Abbreviation: SD, standard deviation.
 Figure 2.:
Figure 2.: Perioperative HR and MAP. Notes: Data were mean with 95% CI over the study period. There were no statistically significant differences in the perioperative HR and MAP. Diprospan group: ropivacaine plus diprospan group; Control group: ropivacaine alone group; t1: before anesthetic induction, t2: skin cutting, t3: skull drilling, t4:skin closure, t5: surgery ending. CI indicates confidence interval; HR, heart rate; MAP, mean arterial pressure.
Table 2. - Postoperative Pain and Analgesia Situation and Postoperative Analgesic Pump Usage Variables Diprospan group (n = 48) Control group (n = 48) Mean difference or RR (estimate 95% CI) P value Cumulative sufentanil consumption within 48-h postoperatively (µg) 5 (0–16) 38 (30.5–46) – <.001a Number of patients who have no sufentanil consumption, n (%) 18 (37.5) 1(2.1) 1.6 (1.3–2.0)b <.001a The time of first PCA demand (h) 24 (9.5–48) 10 (6–16.5) – <.001a Usage of dexamethasone, n (%) 11 (22.9) 13 (27.1) 1.2 (0.7–1.9)b .488a Dosage of dexamethasone (mg) 0 (0–10) 0 (0–10) – .495aValues presented as median and interquartile range (25%–75%).
Diprospan group: ropivacaine plus Diprospan group; control group: ropivacaine alone group.
Abbreviations: CI, confidence interval; PCA, patient-controlled analgesia; RR, risk ratio.
aWilcoxon rank-sum test.
bThis value is RR.
Local infiltration solution was administered after intubation, before skin incision, and with a 22-gauge needle into the skin at a 45° angle along the incision, throughout the entire thickness of the scalp as well as the head clamp points. Local infiltration was performed by the attending neurosurgeon in charge of the craniotomy. Total volume of local infiltration solution used was also determined by the attending neurosurgeon, according to the length of the incision, and was recorded by the investigator.
Intravenous PCA device Apon electronic infusion pumps (ZZB-I-150, Apon Medical Technology CO, LTD) were connected to the patients before leaving the operation theater. The PCA was formulated as 100-µg sufentanil and 16-mg ondansetron diluted to make a total volume of 100 mL with normal saline. The parameter of PCA was set to provide a bolus of 2-mL intravenous infusion with a 10-minute lockout time, and the maximum dose was limited to 8 μg per hour. No background flow was set. The patients could push the PCA button by themselves when NRS scores were above 4 and could repeat until pain was relieved. If participants experienced inadequate analgesia 5 times after sufentanil bolus, the bolus dose was increased to 3 μg, and the maximum dose was increased to 12 μg per hour.
Outcome MeasuresPatients were visited at regular time points after craniotomy, by a specially trained research assistant who was not directly involved in study design or data analysis. All outcomes and adverse events during hospitalization were recorded through inpatient visits. Data for outcomes after discharge were obtained during in-person follow-up visits or via video call.
Primary OutcomeThe primary outcome of our study was the cumulative sufentanil consumption through PCA device within 48 hours after surgery.
Secondary Outcome. Postoperative pain scores were assessed by NRS (ranging from 0 to 10, where 0 and 10 represent no pain and worst imaginable pain, respectively). The NRS scores were recorded at 2 hours, 4 hours, 8 hours, 24 hours, 48 hours, 72 hours, 1 week, 2 weeks, 1 month, 3 months, and 6 months after surgery. Patient Satisfaction Scale (PSS) (ranging from 0 to 10, where 0 represents unsatisfactory and 10 represents very satisfactory) was also recorded at the same points as the NRS. The number of participants who did not receive any sufentanil via PCA device within 48 hours after the operation. The time of first PCA demand within 48 hours after the operation. Postoperative nausea and vomiting (PONV) was assessed by the simplified PONV scale18 (0, absent; 1, nausea not requiring treatment; 2, nausea requiring treatment; and 3, vomiting) at 2, 4, 8, 24, and 48 hours after surgery. Ramsay Sedation Scale (RSS)19 at the same point in time as PONV. The times of hypotension and respiratory depression requiring clinical interventions within 48 hours after the operation. Recovery: time to tracheal extubation and length of stay (LOS). Wound Healing Score20 (total score of 3, excellent wound healing; score 4 to 5, good wound healing; and score 6+, suboptimal wound healing) at 3 and 6 weeks after surgery. Statistical AnalysisSPSS (version 25.0) was used for statistical analysis. The normality of variables was assessed using the Kolmogorov-Smirnov test. Normally distributed continuous data such as duration of surgery, time to extubation, volume of local infiltration solution, total amount of sufentanil and remifentanil consumption (μg) in surgery, and Wilcoxon rank-sum test were used to compare the skewed data including the total amount of sufentanil and remifentanil consumption in surgery, sufentanil consumption within 48 hours postoperatively, PONV, RSS, and LOS. Analyses of NRS and PSS were performed using linear mixed models, with treatment, time, and treatment by time included as fixed effects and within-person correlation modeled as a random effect. A χ2 test or a Fisher exact test was used to compare the number of patients who had no sufentanil consumption and safety outcomes, and the results were presented as risk ratio (RR) and 95% confidence interval (CI). In addition, the time of first analgesic demand was compared by log-rank test and reported as hazard ratios (HRs) with 95% CI. The median time of the first PCA demand was estimated by Kaplan-Meier curves. Analyses of all outcomes were performed following the intention-to-treat principle. A P value of <.05 was considered statistically significant. Meanwhile, multiple imputations were used to handle missing data on the outcomes at 6 months.
Sample SizeTests for 2 independent means (2-sample t test allowing equal variance) were used to calculate the sample size. Based on previous studies and our clinical experience,21 we estimated that the dose of sufentanil after surgery in participants who received preemptive scalp infiltration with 0.5% ropivacaine was approximately 100 ± 50 μg, and the postoperative pain intensity or analgesic requirements would be decreased by about 35% to 40% with the addition of Diprospan. Thus, we hypothesized that the dose of sufentanil would be 62 ± 50 μg within 48 hours postoperatively in the Diprospan group. Based on 90% power to detect a significant difference (α = 0.05; 2-sided), 38 participants were required in each group. Considering a 20% withdrawal rate, the sample size was 48 in each group. The Power Analysis and Sample Size (PASS) V.15 software (NCSS) was used.
RESULTSOf a total of 120 patients screened (Figure 1), 24 patients (20 patients did not meet the inclusion criteria and 4 patients declined to participate) were excluded. A total of eligible 96 patients (48 patients in the Diprospan group and 48 patients in the control group) were randomized and received either of the study interventions. All participants received the allocated drug in compliance with the protocol and were included in the intention-to-treat analysis of primary outcome. Figure 1 shows the trial profile.
Baseline CharacteristicsPatients’ demographic information is shown in Table 1. There were no significant differences between the 2 groups.
Intraoperative DataOperative duration was slightly longer in the Diprospan group (232.2 ± 12.1 minutes) than in the control group (218.6 ± 12.5 minutes), but the data were not statistically significant (mean difference = 14.4; Supplemental Digital Content 1, Supplement 2, https://links.lww.com/AA/D888). Though there was no difference in the total amount of sufentanil consumption during surgery between Diprospan (36.9 ± 0.8 µg) and control groups (36.3 ± 0.9 µg; mean difference = 0.6), the total amount of remifentanil consumption during surgery in the Diprospan group (8.2 ± 0.3 µg/kg/h) was significantly lower than that in the control group (11.6 ± 0.6 µg/kg/h; mean difference = −3.4). No significant difference was found in the volume of local infiltration solution between the Diprospan group (21.9 ± 0.4 mL, contains Diprospan 0.34 ± 0.05 mL) and the control group (22.5 ± 0.4 mL). There were no significant differences in intraoperative hemodynamic parameters between the 2 groups at all time points (Figure 2).
Primary OutcomeIn the Diprospan group, the cumulative sufentanil consumption within 48 hours postoperatively through PCA was 5 (0–16) µg, which was significantly lower than that in the control group (38 [30.5–46] µg; P < .001; Table 2).
Secondary OutcomesThere were significant time differences for median (interquartile range) NRS (P < .001; Supplemental Digital Content 2, Supplement 1, https://links.lww.com/AA/D889 and Supplemental Digital Content 3, Supplement 3, https://links.lww.com/AA/D890) and PSS (P < .001). NRS was significantly lower, and PSS was significantly higher in the Diprospan group than that in the control group (P < .001). Nineteen (19.8%) participants (18 participants in the Diprospan group and 1 participant in the control group) had no sufentanil consumption within 48 hours after the operation (P < .001). The median time of first PCA demand was 24 hours in the Diprospan group and 10 hours in the control group, and the analgesic demand time on PCA device differed significantly by the type of intervention (HR, 0.299; 95% CI, 0.18–0.49; log-rank P < .0001; Figure 3).
 Figure 3.:
Figure 3.: The time of first PCA demand. Kaplan-Meier estimates the time of first PCA demand among patients who were given diprospan as an adjuvant (diprospan group) or ropivacaine alone (control group) for pre-emptive incision site infiltration. CI indicates confidence interval; HR, hazard ratio; PCA, patient-controlled analgesia.
There were no statistically significant differences in PONV and RSS scores within 48 hours postoperatively between the 2 groups (P > .05; Table 3). No patient in this study experienced hypotensive emergency and respiratory depression within 48 hours after postoperatively. The LOS was not significantly different between the 2 groups (13 [11–14] days in the Diprospan group and 14 [12–16] days in the control group; P = .24; Table 3).
Table 3. - Postoperative Recovery Situation Variables Diprospan group (n = 48) Control group (n = 48) Mean difference or RR (estimate 95% CI) P value PONV 2 h 0 (0–0) 0 (0–0) .808a 4 h 0 (0–1) 0 (0–1) .941a 8 h 0 (0–1) 0 (0–1) .831a 24 h 0 (0–0.5) 0 (0–1) .821a 48 h 0 (0–0) 0 (0–0) .603a Summary, n (%) 25 (52.1) 23 (47.9) 0.92 (0.62–1.3)b RSS 2 h 3 (3–3) 3 (3–3) .696a 4 h 3 (2–3) 3 (2–3) .833a 8 h 2 (2–3) 2 (2–3) .678a 24 h 2 (2–2) 2 (2–2) 1.000a 48 h 2 (2–2) 2 (2–2) .696a Length of stay 13 (11–14) 14 (12–16) .240aValues presented as median and interquartile range (25%–75%).
Diprospan group: ropivacaine plus Diprospan group; control group: ropivacaine alone group.
Abbreviations: CI, confidence interval; PONV, postoperative nausea and vomiting; RR, risk ratio; RSS, Ramsay Sedation Scale.
aThis value is RR.
bWilcoxon rank-sum test.
There were no significant difference in wound healing scores at 3 and 6 weeks after surgery between the 2 groups (P = .608 and P = .916, respectively, Supplemental Digital Content 4, Supplement 4, https://links.lww.com/AA/D891). No other severe adverse events or drug reactions directly associated with incision-site infiltration or local Diprospan use were recorded during the study.
DISCUSSIONTo the best of our knowledge, this is the first study to add Diprospan to ropivacaine for incision-site infiltration in craniotomy. The results demonstrate that preemptive scalp infiltration of 0.5% ropivacaine and average 0.34-mL Diprospan per patient significantly decreased the cumulative consumption of sufentanil within 48 hours postoperatively by about 87%, reduced pain scores by about 75% within 72 hours postoperatively and improved about 55% of patient analgesia satisfaction, when compared to 0.5% ropivacaine alone. Furthermore, there were no side effects associated with Diprospan or this drug combination in the present study.
Similar to several prior studies, where the addition of betamethasone to local anesthetics for incision-site infiltration reduced postoperative pain in dental surgery,15,22 we found that preemptive incision-site infiltration of ropivacaine plus Diprospan significantly reduced analgesic consumption and pain degree after craniotomy. In the past, our research team had added dexamethasone to ropivacaine for scalp infiltration and found that the addition of dexamethasone to ropivacaine for preemptive incision-site infiltration reduced 30% analgesia consumption compared to ropivacaine alone, within 48 hours after craniotomy in adults.14 Subsequently, the postoperative analgesic effect of dexamethasone combination was also verified in pediatric craniotomy by our team.13 The positive results were statistically significant; however, the absolute difference in postoperative analgesic consumption and pain scores might have limited clinical significance. Encouragingly, in the present study, we found that Diprospan as a ropivacaine adjuvant to scalp infiltration analgesia significantly decreased analgesic consumption by 33 µg (87%) within 48 hours postoperatively. We deduce that might be due to the anti-inflammatory effect of Diprospan, which is more powerful than dexamethasone. Actual cumulative sufentanil consumption within 48 hours postoperatively (38 [30.5–46] μg) was lower than expected sufentanil usage (100 ± 50 μg) during the design of the study. The main reason for this unexpected discrepancy may be because we only included patients with supratentorial tumors, and infratentorial tumor was not included. However, the real magnitude of the difference (33 μg) was similar to the expected magnitude of the difference (38 μg). Therefore, the difference was indeed clinically relevant. Hence, the postoperative analgesic effect of ropivacaine plus Diprospan is better than ropivacaine plus dexamethasone.
The amount of remifentanil consumption in the Diprospan group was less than that in the control group. In our previous studies, dexamethasone was not found to have reduced intraoperative analgesic consumptions. This might be attributed to Diprospan containing betamethasone disodium phosphate and betamethasone dipropionate,17 and the effect of betamethasone disodium phosphate emerges shortly after infiltration, which is different from dexamethasone.
Craniotomy-induced tissue injury releases different types of inflammatory mediators such as bradykinin, serotonin, and prostaglandins, which could directly stimulate peripheral nociceptors leading to acute pain.23 An increase in inflammatory factors at the wound site is reported to be detectable 48 hours after injury.24 Infiltration of local anesthetics can block the transmission of pain impulses to the central nervous system and provide analgesic effects.25 However, the effect of local anesthetics is only maintained for a short time. As the local anesthetics metabolize, pain appears gradually. Corticosteroids have a powerful local anti-inflammatory effect. The addition of infiltrated corticosteroids can effectively inhibit inflammation caused by surgery and could become one of the strategies to control incisional pain.26 Diprospan is a corticosteroid with a powerful anti-inflammatory effect, and this study confirms that Diprospan plus ropivacaine has a better postoperative analgesic effect than ropivacaine alone, which simply blocks pain signals without anti-inflammatory effect, whereas this miscible liquid does not only block the transmission of pain but also significantly inhibits inflammation. In the future, further clinical studies need to be conducted to screen out more ideal types of steroids, explore more ideal drug ratios and combinations, and target different surgical incision types.
Several studies have reported that a single local infiltration of a very low dose of Diprospan (≤0.7 mL) is safe; our result (0.34 mL) is consistent with previous studies.15,27 The average dose of Diprospan in this study was 2.38-mg betamethasone (0.68-mg betamethasone disodium phosphate and 1.7-mg betamethasone dipropionate) per patient. Since the dose of Diprospan used in this study was low, no patient experienced any side effects associated with the incisional infiltration of Diprospan, such as postoperative delayed wound healing, infection, peptic ulcer, or hemorrhage. Similarly, in the past, our research team did not find any side effects related to dexamethasone incision infiltration either. Although we did not find any adverse effects of Diprospan on wound healing and infection, the current study is not powered for the possible side effects of the treatment. Thus, the effect of local infiltration of Diprospan on wound healing and infection should be taken with caution.
Despite the noted improvement in postoperative pain, this study has some limitations. First, a single dose of Diprospan infiltration was selected in this study. Further studies are needed to elucidate the optimal dose of Diprospan, by exploring the dose-dependent effects of incision-site infiltration with Diprospan. Second, the amount of remifentanil consumption in the control group was more than that in the Diprospan group. While there is a statistically significant difference between the intraoperative remifentanil doses, this is neither a primary nor a secondary outcome that was preplanned. We speculate that reduced remifentanil admission in the disprospan group may have been driven by decreased intraoperative nociceptive and inflammatory input and thus reduced hypertension and tachycardia in response to surgical stimuli. However, given the fact that the treatment allocation was not blinded to anesthesiologists, this may have influenced the anesthesiologists’ decisions to adjust the remifentanil infusion dose based on a presumed belief of how the presence/absence of Diprospan may have influenced the intraoperative analgesic requirement. In addition, remifentanil may lead to opioid-induced hyperpathia (OIH), which may have influenced pain scores and postoperative sufentanil consumption. Third, this is a single-center study, the extrapolation of the research results is limited, and multicenter research needs to be conducted in the future. Forth, the sample size of this study is not powered to assess relative safety of the interventions; therefore, larger clinical trials need to be conducted to assess this. Fifth, in this study, although there was no statistically significant difference in the incidence and dosage of which perioperative intravenous dexamethasone, a systemic dose of dexamethasone (especially perioperative dexamethasone, at high dose, may confer analgesic benefits) still may mask the effects of a single local low dose of local application of Diprospan. The analgesic effect of single Diprospan for incision-site infiltration without the background of perioperative glucocorticoid deserves further clarification. The analgesic effect of single dexamethasone for incision-site infiltration scalp without the background of perioperative glucocorticoid deserves further clarification. Sixth, Diprospan is a kind of injectable suspension (nontransparent); thus, surgeons and anesthesiologists were not blinded in this study. In future studies, it is feasible to blind the surgeons and anesthesiologists by having the medication prepared in the pharmacy in prefilled, nontransparent syringe. Seventh, though patients were instructed in the appropriate use of the PCA device and rarely reported significant PONV at any follow-up time points, it is still possible that PCA use was also driven by postoperative nausea. Finally, this study included only the patients who were scheduled for craniotomy, and attention to the preemptive infiltration of ropivacaine plus Diprospan in other surgeries such as spine surgery is recommended.
In conclusion, this study demonstrates that local infiltration of ropivacaine and Diprospan significantly decreases analgesic consumption within 48 hours postoperatively, reduces pain scores within 72 hours postoperatively, and achieves patient analgesia satisfaction, when compared to ropivacaine infiltration alone; therefore, it is expected to be an alternative for postoperative analgesia. E
DISCLOSURESName: Xueye Han, MD.
Contribution: This author helped draft the manuscript, perform study analysis and figure generation, and read and approve the final manuscript.
Name: Tong Ren, MD.
Contribution: This author helped analyze the study, generate figures, review the manuscript, and read and approve the final manuscript.
Name: Yang Wang, MD.
Contribution: This author helped supervise study analysis, generate figures, review the manuscript, and read and approve the final manuscript.
Name: Nan Ji, MD.
Contribution: This author helped review the manuscript, perform data acquisition and analysis, and read and approve the final manuscript.
Name: Fang Luo, MD.
Contribution: This author helped conceive the idea for this study, perform the final review of the manuscript, and read and approve the final manuscript.
This manuscript was handled by: Oluwaseun Johnson-Akeju, MD, MMSc.
REFERENCES 1. Flexman AM, Ng JL, Gelb AW. Acute and chronic pain following craniotomy. Curr Opin Anaesthesiol. 2010;23:551–557. 2. Gottschalk A, Berkow LC, Stevens RD, . Prospective evaluation of pain and analgesic use following major elective intracranial surgery. J Neurosurg. 2007;106:210–216. 3. Rigamonti A, Garavaglia MM, Ma K, . Effect of bilateral scalp nerve blocks on postoperative pain and discharge times in patients undergoing supratentorial craniotomy and general anesthesia: a randomized-controlled trial. Can J Anaesth. 2020;67:452–461. 4. Galvin IM, Levy R, Day AG, Gilron I. Pharmacological interventions for the prevention of acute postoperative pain in adults following brain surgery. Cochrane Database Syst Rev. 2019;2019:CD011931. 5. An LX, Chen X, Ren XJ, Wu HF. Electro-acupuncture decreases postoperative pain and improves recovery in patients undergoing a supratentorial craniotomy. Am J Chin Med. 2014;42:1099–1109. 6. Bilotta F, Guerra C, Rosa G. Update on anesthesia for craniotomy. Curr Opin Anaesthesiol. 2013;26:517–522. 7. Yang X, Ma J, Li K, . A comparison of effects of scalp nerve block and local anesthetic infiltration on inflammatory response, hemodynamic response, and postoperative pain in patients undergoing craniotomy for cerebral aneurysms: a randomized controlled trial. BMC Anesthesiol. 2019;19:91. 8. Batoz H, Verdonck O, Pellerin C, Roux G, Maurette P. The analgesic properties of scalp infiltrations with ropivacaine after intracranial tumoral resection. Anesth Analg. 2009;109:240–244. 9. Fitzpatrick CL, Weir HL, Monnet E. Effects of infiltration of the incision site with bupivacaine on postoperative pain and incisional healing in dogs undergoing ovariohysterectomy. J Am Vet Med Assoc. 2010;237:395–401. 10. Kilinc L, Türk B, Türk HS, Cinar S, Turgut S, İslamoğlu S. Peritonsillar dexamethasone-bupivacaine vs. bupivacaine infiltration for post-tonsillectomy pain relief in children: a randomized, double-blind, controlled study. Eur Arch Otorhinolaryngol.
留言 (0)