Impact of Low-dose Chest CT Screening on the Association Between Rurality and Lung Cancer Outcomes
Introduction:
Lung cancer mortality is higher among rural United States populations compared with nonrural ones. Little is known about screening low-dose chest computed tomography (LDCT) outcomes in rural settings.
Materials and Methods:
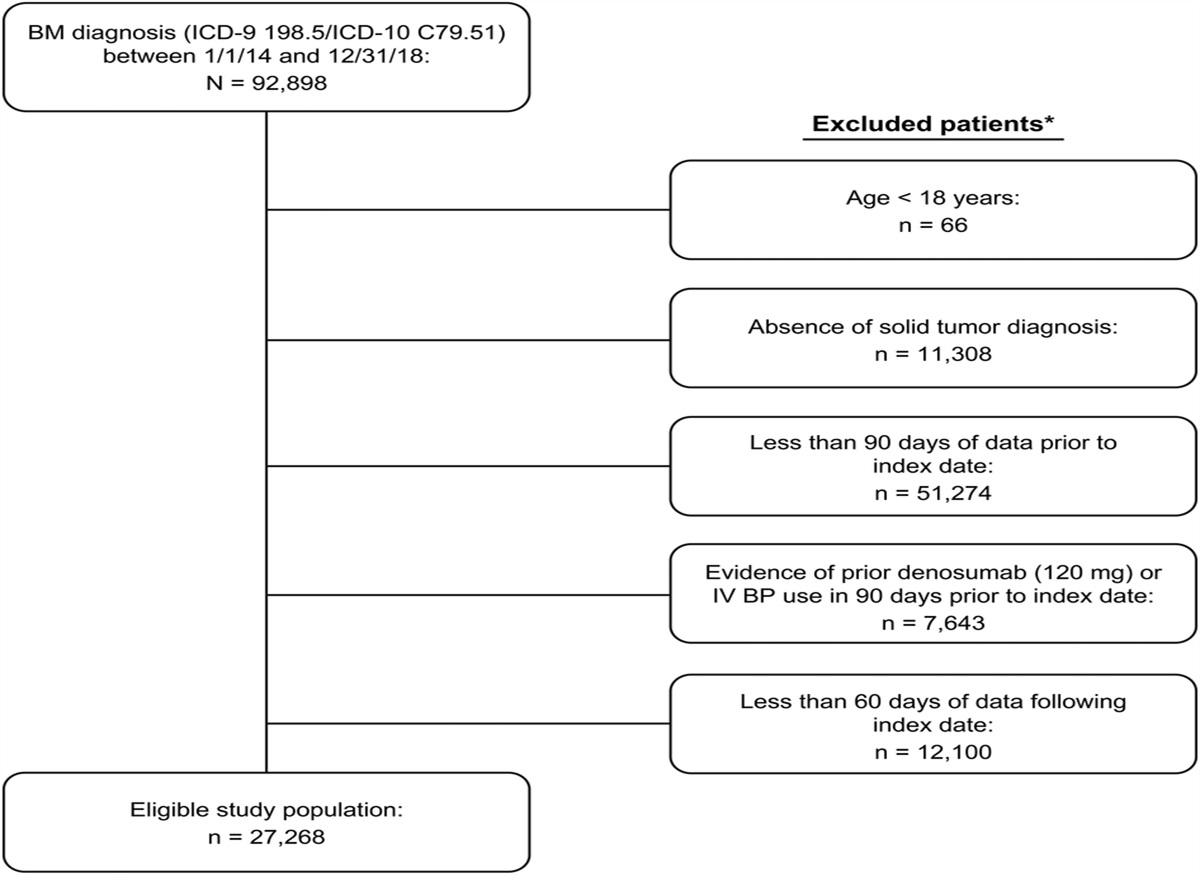
This retrospective cohort study examined all patients (n=1805) who underwent screening LDCT in a prospective registry from March 1, 2015, through December 31, 2019, in a majority-rural health care system. We assessed the proportion of early-stage lung cancers (American Joint Committee on Cancer stage I-II) diagnosed among LDCT-screened patients, and analyzed overall survival after early-stage lung cancer diagnosis according to residency location.
Results:
The screening cohort had a median age of 63 and median 40-pack-year smoking history; 62.4% had a rural residence, 51.2% were female, and 62.7% completed only 1 LDCT scan. Thirty-eight patients were diagnosed with lung cancer (2.1% of the cohort), of which 65.8% were early-stage. On multivariable analysis, rural (vs nonrural) residency was not associated with a lung cancer diagnosis (adjusted hazard ratio 1.59; 95% CI, 0.74-3.40; P=0.24). At a median follow-up of 37.1 months (range, 3.3 to 67.2 months), 88.2% of rural versus 87.5% of nonrural patients with screen-diagnosed early-stage lung cancer were alive (P=0.93).
Conclusions:
In a majority-rural United States population undergoing LDCT, most screen-detected lung cancers were early-stage. There were no significant differences observed between rural and nonrural patients in lung cancer diagnosis rate or early-stage lung cancer survival. Increased implementation of LDCT might blunt the historical association between rural United States populations and worse lung cancer outcomes.

留言 (0)