
記住我




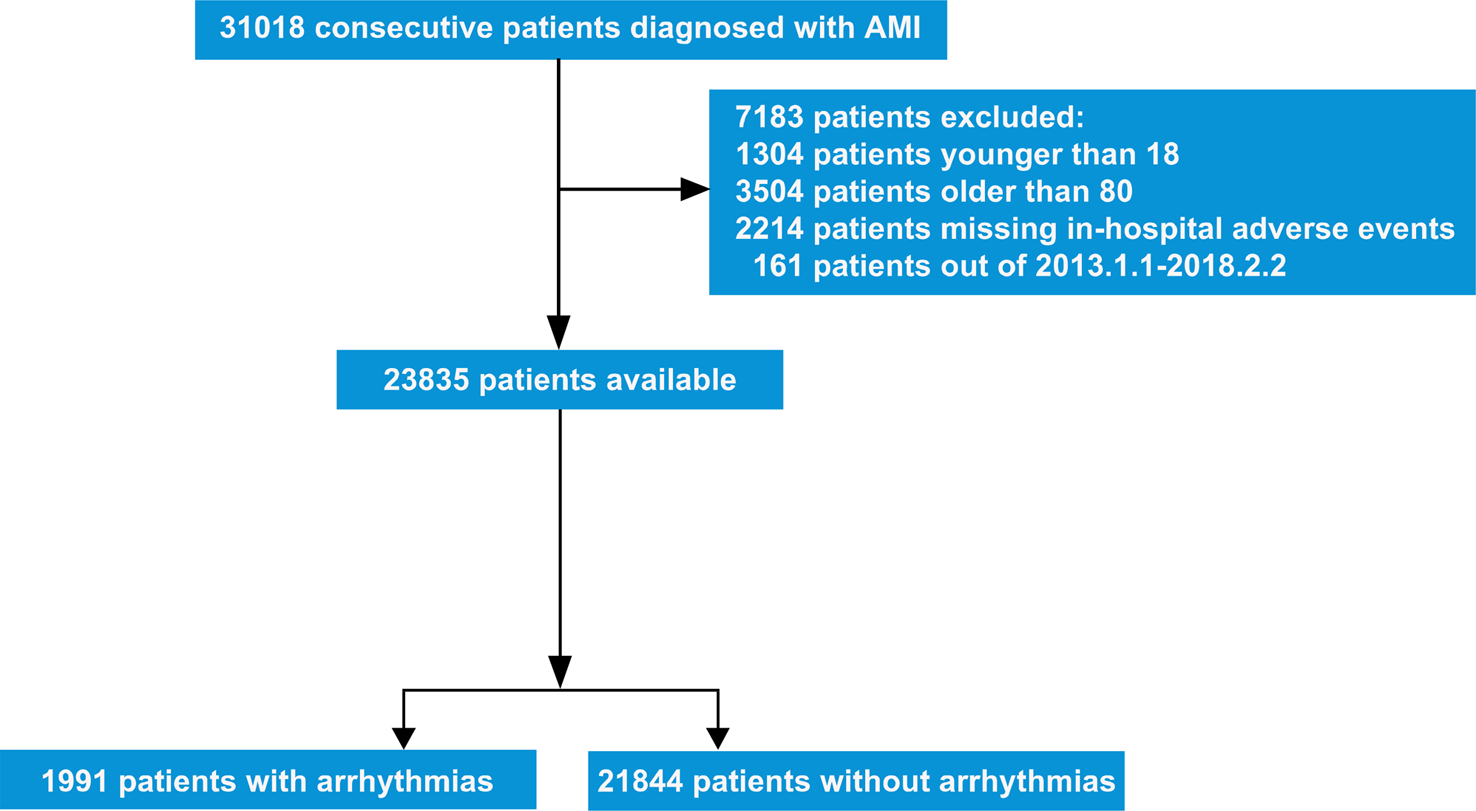




We searched the PubMed database until July 21 2022 using the keywords “Cardiac Schwannoma” and “Cardiac tumour and Schwannoma” to identify the relevant English medical literature. The search identified 332 results. After a careful analysis of the articles, approximately 24 articles met the inclusion criteria and were included. In addition, 3 patients dates from one of the abovementioned paper [5], which could not be retrieved from PubMed, were also added to this review. The study selection process is shown in Fig. 4. Two reviewers independently appraised all included studies using the Joanna Briggs Institute (JBI) checklist for case reports and case series.
Fig. 4
Selection of studies for inclusion
Primary cardiac tumours are very rare, and benign cardiac schwannomas are even rarer. Our review of English literature showed that 27 cases of benign cardiac schwannomas including two cases of type II neurofibromatosis [12, 25] have been reported. The age range was 12–72 years old, the mean age was 50.7 years old, and the male-to-female ratio was about 1:2. These data were consistent with previous reports [5]. Primary cardiac schwannoma is believed to originate from the cardiac plexus or the cardiac branch of the vagus nerve; therefore, it is located primarily on the right side of the heart [26]. However, we found that the right atrium is the predominant site of cardiac schwannomas (12/28), and the incidences of left atrial, bilateral ventricular and aortic outflow tracts have no remarkable differences. This finding could be attributed to the distribution of the sinoatrial and atrioventricular nodes around the right atrium because the distribution of nerve fibres around these structures is remarkably higher than that in the surrounding working myocardium. The case that we reported occurred in the lateral wall of the right ventricle. It is the third case of schwannoma that occurred in the free wall of the right ventricle. This study provides an important supplement to explore the pathogenesis of the lesion and reflect the distribution of cardiac plexus.
Neurilemoma originates from the peripheral nerve sheath, and its pathogenesis remains unclear. No relevant literature has proposed hypotheses regarding its cause. The National Toxicology Program and Ramazzini Institute reported that radiofrequency electromagnetic field substantially increases glioma and schwannoma in the heart of rodents [27]. Stephen Factor et al. reported that a patient with cardiac neurilemoma who received a large total amount of radiotherapy or at least one course of radiotherapy directed to the lower thoracic vertebral region for the treatment of paravertebral mass may have peripherally involved the heart [6]. The relationship between human cardiac schwannoma and radiation needs further research. Additionally, Das Gupta et a1. studied 303 benign schwannomas and reported the interesting correlation of nerve sheath tumours with the past, concurrent or future development of a malignancy unrelated to peripheral nerves [28]. Through case review, we found that seven cases, including our case, were accompanied by other tumours, including six cases of malignancy and one unspecified case. The seven tumours included one autopsies case of ovarian cancer [6] and one autopsies cases of lung cancer [5], one case of renal cancer preceded cardiac schwannoma [3], one case of synchronous sigmoid colon cancer [21], one case of synchronous cancer of the left chest wall [4] and one case of synchronous cavernous mass of the bladder [14], one cases of synchronous lung adenocarcinoma (our case). The connection between schwannoma and other unrelated malignancy needs further experimental verification.
Primary cardiac schwannomas vary in size. The clinical symptoms are mostly caused by compression or obstruction, and some patients may have dyspnoea on exertion (5/28) [12, 17, 18, 23], chest pain (4/28) [3, 7, 8, 19], shortness of breath (4/28) [3, 7, 10, 24], palpitation (2/28) [15, 20], arrhythmia (2/28) [8, 10] and other discomfort. More than one third of patients (10/28) [4,5,6, 9, 14, 16, 21,22,23] had no related symptoms. Our case was hospitalised because of syncope, which is rarely reported in literature. The syncope may be caused by the sudden decrease or pause of cardiac output caused by the cardiac tumour.
Cardiac schwannoma can be detected by X-ray or echocardiogram, CT and magnetic resonance imaging (MRI), which can help to better determine the location and extent of the mass and the involvement of other structures [3]. Tumours are mostly heterogeneous masses with cystic changes, haemorrhages and calcifications. Uneven and mild enhancement may even occur. Some lesions have a broad base and shallow lobes, and most lesions have a clear boundary. The fibrous capsule is also one of the identification points of schwannomas from other tumours. Coronary angiography is required for patients at risk of coronary heart disease or with tumours that may involve the coronary artery [4]. When the exact origin of the tumour cannot be obtained by CT or MRI, 3D printing and model establishment can help to clearly identify the location of the tumour and its relationship with large blood vessels [20]. The nature of the tumour is difficult to identify through imaging.
Most patients with cardiac Schwann cell tumours undergo extensive radical tumour resection and cardiac reconstruction with autologous pericardium or artificial patch under CPB [5]. The degree of involvement and reconstruction of the atrioventricular valve, coronary artery, coronary sinus or pulmonary vein are also important [4, 5, 13]. Among the 28 patients, excepting for 2 autopsy patients, 2 patients whose survival/death was not mentioned in the literature, and 1 patient whose data was not available, the survival rate of the remaining 23 patients was 100% in the follow-up period, and the postoperative prognosis is good. Our operation was also successful, and no recurrence was observed after 5 years of follow-up.
In conclusion, this is a rare case added to the limited existing literature on cardiac schwannoma. Comprehensive analysis of various imaging examinations is helpful to determine the extent of the tumour. Complete surgical resection is recommended for similar cases involving cardiac schwannomas, especially when the patient has related symptoms. Patients generally have a good prognosis. The pathogenesis of cardiac schwannoma needs further research in order to prevent and manage this rare lesion.
留言 (0)