
記住我







A detailed search of the literature was carried out in MEDLINE (PubMed), Embase, and Cochrane databases. We conducted a PubMed search using the following search string: (("ovarian neoplasms"[MeSH Terms] or ("ovarian"[All Fields] and "neoplasms"[All Fields]) or "ovarian neoplasms"[All Fields] or ("ovarian"[All Fields] and "cancer"[All Fields]) or "ovarian cancer"[All Fields]) and ("lymphnodal"[All Fields] or "lymphnode"[All Fields] or "lymphnodes"[All Fields] or ("lymph nodes"[MeSH Terms] or ("lymph"[All Fields] and "nodes"[All Fields]) or "lymph nodes"[All Fields] or ("lymph"[All Fields] and "node"[All Fields]) or "lymph node"[All Fields])) and ("dissect"[All Fields] or "dissected"[All Fields] or "dissecting"[All Fields] or "dissection"[MeSH Terms] or "dissection"[All Fields] or "dissections"[All Fields] or "dissects"[All Fields] or ("lymph node excision"[MeSH Terms] or ("lymph"[All Fields] and "node"[All Fields] and "excision"[All Fields]) or "lymph node excision"[All Fields] or "lymphadenectomies"[All Fields] or "lymphadenectomy"[All Fields]))) and (clinicaltrial[Filter]). The last search was done on January 22, 2022.
All the published randomized controlled trials (RCT) comparing lymphadenectomy versus no lymphadenectomy in epithelial ovarian cancers were included.
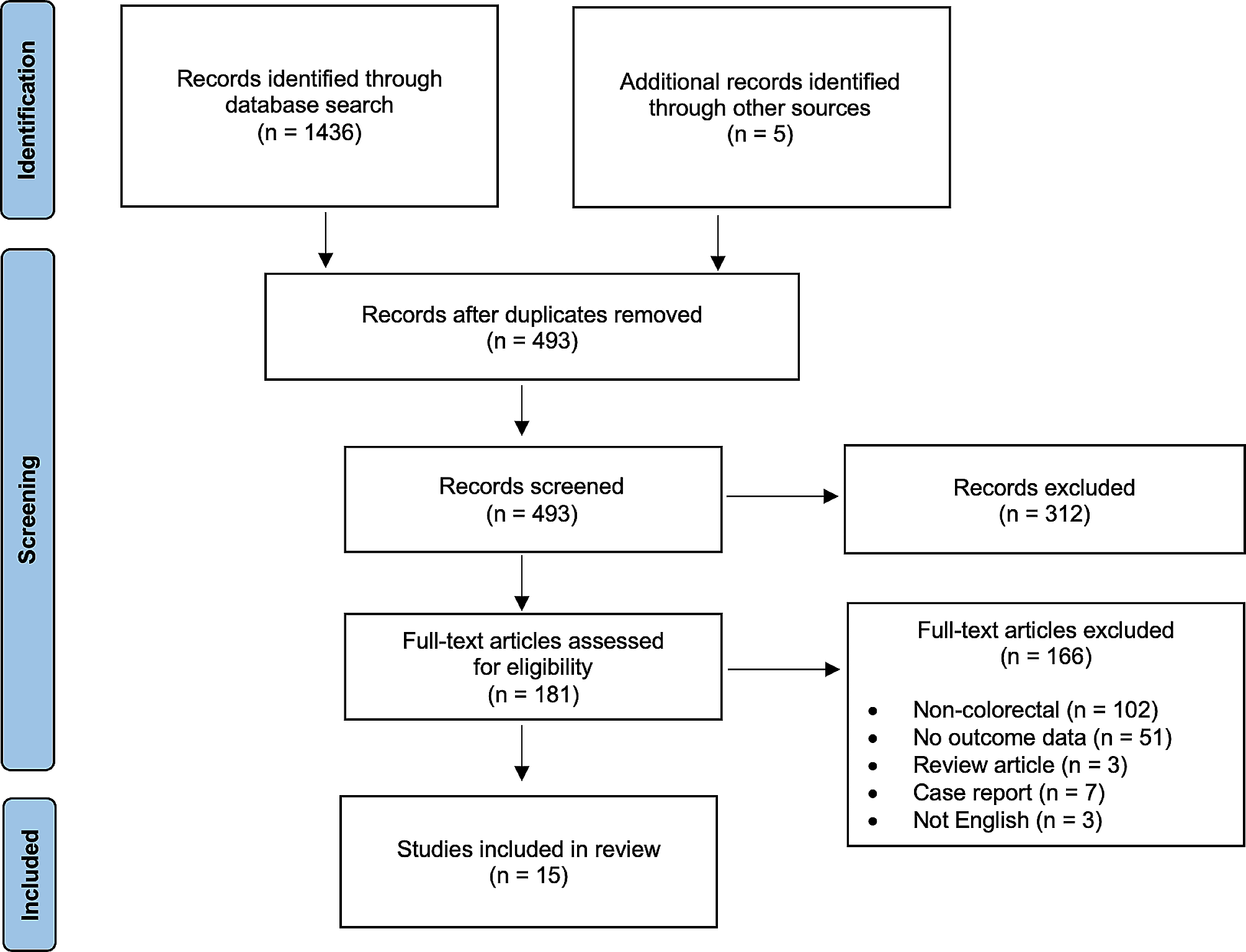
Out of 84 studies found from the above search, 03 were shortlisted after abstract reviews [5, 7, 10] (Fig. 1). Additional crosschecks for any missing studies were done using manual search and back referencing. However, no more studies were found. In all, after the elimination of duplicates and exclusions, only three studies were considered for the final meta-analysis.
Fig. 1 Inclusion and exclusion criteria
Inclusion and exclusion criteriaAll randomized trials that compared lymphadenectomy versus no lymphadenectomy in epithelial ovarian cancers were considered. Operability was considered based on preoperative evaluation of the respective centers and by the authors of each individual RCT.
Exclusion criteria entailed non-randomized studies, cohort, retrospective, observational studies, and unpublished abstracts presented in meetings.
Data extractionTwo authors individually scanned all abstracts and shortlisted studies meeting the above inclusion criteria. Data from each of these shortlisted studies was collected on a pre-set proforma. Any discrepancies in the inclusion were settled after a discussion with a third member. The quality of each study was evaluated using Jadad’s score [11] and the revised Cochrane risk of bias tool (ROB 2.0 _IRPG_ beta v8) [12]. Patients with systematic lymphadenectomy and those without lymphadenectomy were categorized into two groups.
As different variables were evaluated in different studies, only the common variables were considered for the final analysis.
For final analyses, two endpoint variables were compared. The variables studied were progression-free survival (PFS) and overall survival (OS). The OS is defined as the time from the date of recruitment to death, and the PFS was defined as the time from recruitment to the progression of the disease, as described in the studies. Publication bias was measured using a funnel plot. One reference cited in the introduction and discussion is in German [1]. It was translated into English using Google Translate.
Statistical analysisAs the data on individual patients were not available, we performed the meta-analysis of hazard ratio based on the methods described by Tierney et al. (2007) [13]. The statistical software R, especially the package “meta,” was used to perform the entire meta-analysis including the draws based on forest and funnel plots [14].
For OS and PFS data, we extracted the hazard ratio and its standard error based on different trials.
The Cox-Mantel estimate of the hazard ratio is formed by dividing the hazard rate under the treatment group by that under the control group. Obviously, the estimate so obtained measures the change in risk of treatment versus control over the follow-up period. Since the distribution of the log hazard ratio is nearly normal, one can consider logarithmic transformation for the purpose of meta-analysis. The formula for the hazard ratio can be given by
$$\textrm}_}=\frac}_}}}_}}=\frac^}_}}\!\left/ \!_}_}}\right.}^}_}}\!\left/ \!_}_}}\right.},$$
where HT denotes the hazard rate under the treatment group and HC denotes the hazard rate under the control group. Similarly, OT(ET) and OC(EC) denote the observed (expected) number of events (that is, deaths in our case) for treatment and control groups, respectively. One can refer to Parmar et al. [15] and Parmar and Machin [16] for further details.
As explained earlier, since the log hazard ratio is nearly normal, a confidence interval for the hazard ratio can be constructed by transforming it to the logarithmic scale and using the corresponding normal approximating formula given as follows:
$$\ln \left(}_}\right)\pm }_}\left(}_}_}\right)}\right)$$
where \(}_}_}\right)}\) denotes the standard error of ln(HRCM). This can be further expressed as follows:
$$}_}_}\right)}=\sqrt}_}}+\frac}_}}}.$$
Once the interval is obtained, it can be transformed back to get the confidence interval for the hazard ratio.
An alternative estimate of the hazard ratio based on the Mantel-Haenszel estimator and the corresponding log-transformed confidence interval can be expressed as follows:
$$}_}=\exp \left(\frac}_}-}_}}}\right),$$
and
$$\ln \left(}_}\right)\pm }_}\left(}_}_}\right)}\right),$$
where \(}_}_}\right)}\) denotes the standard error of HRMH,given by \(\sqrt}}\) and V is the Mantel-Haenszel hypergeometric variance.
In the absence of data for the individual patients, Tierney et al. [13] suggested methods available to obtain HRs and the associated summary statistics by carefully employing other existing data where the hazard ratio and its associated confidence interval (CI) were presented in a trial report. The variance of ln(HR), say V∗, can be obtained by the following:
$$^=\frac\ \textrm\ \textrm\ \textrm\right)-\ln \left(\textrm\ \textrm\ \textrm\ \textrm\right)}\ \textrm\ \textrm\ \textrm\ \textrm\right)},$$
Obviously, if 95% CI is given in the trial report, the above equation leads to V∗ obtained as follows:
$$^=\frac\ \textrm\ \textrm\ 95\%\textrm\right)-\ln \left(\textrm\ \textrm\ \textrm\ 95\%\textrm\right)}.$$
Likewise, V can also be obtained easily from the CI, if the same is desired. The test of significance, if required, can be performed using z test.
Sometimes, it is desired to perform a test for heterogeneity to examine the null hypothesis that all the studies are leading to the same effect. The heterogeneity is tested using chi-square and I2 statistics where the latter actually describes the percentage of variation across studies that is due to heterogeneity.
The manuscript is presented following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines, and the PRISMA checklist has been provided in the supplemental material [17]. The meta-analysis has been registered with PROSPERO [18] (CRD42021281583).
留言 (0)