
記住我






Collectively, the data supports the urgent need to increase naloxone training for pharmacists and embed naloxone training within the pharmacy curricula. The objective of the current study was to determine the effectiveness of implementing an expanded naloxone training program, which, unlike the studies described above, is an all-encompassing approach that covers a number of items, including: (1) identifying patients at risk of an opioid overdose, (2) choosing a patient-specific naloxone product from a case-based scenario, (3) reducing stigma, (4) providing patient counseling and education, (5) responding to an overdose, (6) learning to follow a statewide board of pharmacy protocol, and (7) using a community pharmacy simulation lab to replicate dispensing a prescription for naloxone.
3. Methods 3.1. Educational Activity and SettingGiven the expanded scope of practice for pharmacists in California, a curriculum-based naloxone certificate training program was created to train student pharmacists to furnish and dispense naloxone. According to the protocol, students should be able to screen potential recipients, provide training in opioid overdose, properly select a patient-specific naloxone product, provide education and counseling on naloxone, offer resources or referrals for opioid addiction treatment to recipients, properly document the encounter and, if appropriate, dispense the product to the patient.
A naloxone training certificate program was provided to P2 students at California Northstate University College of Pharmacy during their fall semester practicum lab course. The naloxone certificate program was first developed and delivered in 2020 and repeated in 2021. Over that two-year period, 185 students were trained through this program. The professor involved in the development and implementation of this course was a community pharmacist with experience in dispensing naloxone to individuals in California and who also trained other pharmacists through California BOP training programs and other continuing education events. This certificate program was used to train student pharmacists to furnish naloxone to a patient, under a pharmacist’s supervision and without a physician’s prescription, under the California BOP protocol [27].Prior to the training session a 28-question naloxone pre-training baseline knowledge and confidence survey was administered. Two survey questions asked about previous naloxone education or training, three survey questions captured demographic information, and the final twenty-three survey questions evaluated student knowledge and confidence in furnishing naloxone and the BOP state protocol. Of the 23 survey questions, 4 were knowledge-based quiz-like questions and 19 were 5-point Likert scale survey questions that were developed to assess self-confidence and familiarity with opioid overdose risks, patient-specific naloxone product selection, naloxone pharmacology, the BOP protocol, and comfortability of counseling and educating patients about opioid overdose and naloxone. The study lead, Dr. Jennifer Courtney, a practicing community pharmacist who is qualified to administer naloxone and who provides naloxone training to CNUCOP students, pharmacists, other healthcare professionals, and community stakeholders, developed the survey. The co-authors, 5 of whom are licensed pharmacists, reviewed the survey prior to administration to help ensure the questions were relevant.
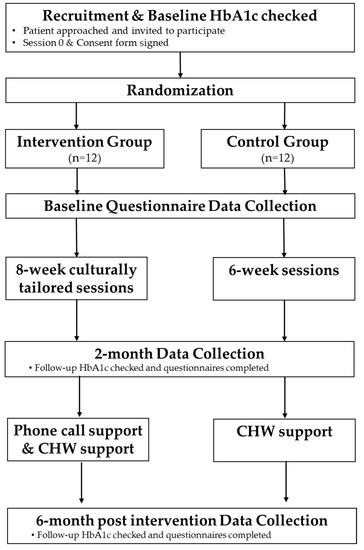
Three identical surveys were administered to students. The pre-training survey was given before the training session, the post-training survey was given after the 3 h in-class training session and TBL applications, and the final post-assessment survey was given after the three final assessments (Figure 1). More details on the assessments are provided below. Please note that the majority of CNUCOP classes are delivered using TBL pedagogy, meaning that students have already experienced TBL pedagogy in prior classes. No identifying information was collected and all surveys were completed anonymously via Survey Monkey. To link the three surveys, each student selected an unidentifiable self-chosen unique code. Informed consent for the study was obtained through a statement at the beginning of the survey and a checkbox stating, “I consent”.The in-class naloxone training included a 1 h lecture-based educational session. After the 1 h naloxone training, a 2 h hands-on team-based application session was provided. Because naloxone stigma is considered a major barrier for naloxone prescribing, one of the team-based applications was designed to address the stigma surrounding naloxone access. Students completed a series of two team-based applications on (1) patient naloxone conversation starters and (2) patient counseling on naloxone products. In pre-established TBL teams, students were prompted to discuss ways to initiate conversations with patients about naloxone. Students were to discuss the benefits of their patient having naloxone on-hand at home and identify analogies or other ways to convey the importance of having naloxone without making patients feel stigmatized. Students were to choose non-stigmatizing language that promotes empathy and understanding and that reduces the perception of judgment. Students were then divided into groups of two to practice naloxone patient counseling. A third application was then given where students practiced documentation, including writing a new prescription for a naloxone product they were furnishing. A follow-up survey was given at the end of the 3 h class session and consisted of 23 of the 28, questions to determine their knowledge and confidence after the in-class training session. The 5 previous training and demographic questions were left out of the second and third surveys due to the ability to link the surveys by the student’s unique identifier chosen.
Participation in the in-class training, activity, and assessment was required as part of the practicum course; however, participation in the study was voluntary. This study was approved by the California Northstate University Institutional Review Board.
3.2. Evaluation and AssessmentThree summative assessments took place, including: (1) a naloxone patient case assessment, (2) the proper typing of a patient prescription label for dispensing, and (3) counseling of a patient on a naloxone product. The naloxone patient case assessment took place in our state-of-the-art Advanced Practice Pharmacy Simulation (APPS) Lab, which simulates a community pharmacy setting. The case was provided to students via a learning management system, CANVAS, and consisted of 6 questions that evaluated the student’s knowledge of opioid overdose risk factors, appropriate naloxone product selection based on patient-specific factors, procedures required by the BOP protocol, and specific drug information regarding naloxone. In addition, students had to properly type a prescription label for the naloxone product they selected for the patient, which was graded on choosing the correct patient, the most appropriate naloxone product for the patient, the proper number of doses required for furnishing under the BOP protocol, and the correct directions for the product. Naloxone patient counseling was scored by a faculty grader using a modified American Pharmacists Association (APhA) patient counseling rubric. The APhA rubric is used as a standard rubric by most pharmacy schools and for the APhA-ASP (Academy of Student Pharmacists) National Patient Counseling Competition. The rubric was modified for furnishing a naloxone product and consisted of a total of 46 points. Fourth-year pharmacy students served as standardized patients for the patient counseling.
3.3. Statistical AnalysisBaseline characteristics collected through the survey were presented as proportions. Knowledge-based quiz-like survey scores were presented as mean scores and standard deviations. Opinion-based Likert scale survey questions were presented as the proportion of subjects choosing to answer affirmatively, akin to “agreed” or “strongly agreed”, when referring to a statement. Normality of knowledge-based quiz-like survey scores was determined using the Shapiro–Wilk test. A comparison of knowledge-based quiz-like survey scores between two surveys administered before or after various phases of the course was conducted in a pairwise fashion using a paired t-test, while a comparison of opinion-based survey questions was conducted in a pairwise fashion using a Wilcoxon signed-rank test. An alpha level of 0.05 and a 95% confidence interval were selected to denote statistical significance. Cronbach’s alpha was calculated to assess the level of internal consistency for opinion-based surveys at all three phases of the course, with values ranging from 0 to 1, where 0 represented a complete lack of internal consistency and 1 represented perfect consistency.
4. ResultsDuring the naloxone training in our 2020 and 2021 cohorts, a total of 107 subjects completed the study, with 107 completing the pre-training and post-training survey, only 68 completing the post-training and post-assessment survey, and 71 completing the pre-training and post-assessment survey. An examination of baseline characteristics revealed that about 15% of students underwent some form of previous naloxone training. If the student answered yes to having previous education or training on naloxone, a follow-up question was asked to describe the training. Most responses indicated informal training either through a self-study or through their Introductory to Pharmacy Practice Education (IPPE) community pharmacy rotation. Some responses indicated that they previously learned basic information about naloxone during interprofessional education (IPE) at another college and briefly during a pharmacotherapy course given at our university.
Demographic analysis of students surveyed found that about 63% of the subjects were female and 96% were younger than 35 years of age, with 66% self-identifying as Asian, 17% as Caucasian, 4% as Black, and 4% Hispanic. A statistically significant increase in the knowledge-based quiz-like scores was observed at every subsequent stage of the training, with the greatest increase of 42.1% observed after the in-class training phase of the course compared to a much smaller increase of 7.2% observed after the assessment phase of the course (Table 1). Likewise, a statistically significant increase in the proportion of students affirmatively answering survey questions was observed at nearly every subsequent stage of the course, with the largest increase observed after the training phase of the course compared to a much smaller increase after the assessment phase of the course. The only exception was for the question asking, “do you believe that utilizing pharmacists to increase naloxone access can save lives”, where a 3% reduction was observed in the proportion answering affirmatively on the post-assessment relative to the pre-training assessment, with no statistically significant difference observed (Table 2). Cronbach’s alpha was determined to be above 0.9 indicating very high internal consistency for the opinion-based surveys administered at all three phases of the training, thereby implying strong reliability of the surveys in general (Table 3).Three summative assessments were given after the in-class training session. The average scores for the naloxone assessments were 83% for the APPS lab patient case scenario (lowest score = 2.3/6, highest score = 6/6), 90.5% for the typed prescription label for dispensing (lowest score = 4.5/10, highest score = 10/10), and 88.5% for the patient counseling (lowest score = 30/46, highest score = 46/46). The only difference between the two cohorts was that the in-class training and applications were virtually administered in 2020, due to the COVID-19 pandemic, and in 2021, they were given in person.
5. DiscussionThe multi-phase curriculum-based naloxone certificate training program, which included lecture-based education, team-based learning applications, case-based scenarios, and summative assessments, was found to improve pharmacy student knowledge and confidence in furnishing naloxone under a state BOP protocol. Prior to the administration of the certificate training program, most students expressed discomfort towards naloxone, which may have resulted from an unfamiliarity with naloxone products. Once students were able to discuss the topic in class and further practice in the APPS lab, students demonstrated improved knowledge and comfort towards furnishing naloxone under protocol.
This study addresses important gaps in previous literature assessing naloxone education and training among pharmacy students. To our knowledge, this is the first study that evaluates such a robust naloxone training program and is also the first to utilize some TBL pedagogy in the training. The previously published six articles include some aspects of the individual training provided but none are all-encompassing like the training provided in our curriculum. We feel that the inclusion of an approach to addressing stigma, furnishing naloxone without a physician’s prescription, and the comprehensive, multi-phase training are the three key things that set our study apart. Schartel et al. assessed the patient counseling component but did not address the real-life simulation of preparing a naloxone prescription for dispensing to a patient. Kavanaugh et al. assessed the effectiveness of naloxone education and preparing students to dispense via a standing order through use of academic detailing. Though it is crucial to learn this skill of providing evidence-based education to physicians in order to improve the quality of care and patient outcomes, a physician’s prescription for naloxone is not generally needed in most states that now operate under a standing prescription order or pharmacist furnishing protocol. Because of this, academic detailing may not be a necessary skill for the dispensing of naloxone. The study by Musco et al. focused on the training of pharmacy students to be able to administer naloxone but did not train students on appropriate furnishing under a board of pharmacy protocol. Given that community pharmacy positions are projected to remain at about 60% of the overall pharmacy workforce through at least 2026, it is equally important to train our student pharmacists who will be filling these community pharmacy roles to have a greater impact on naloxone access [28]. The naloxone training provided by Bachyrycz et al., Jacobson et al., and Donohoe et al. is most similar to the training provided in our college of pharmacy. The training described in the studies by Bachyrycz et al. and Jacobson et al. did not appear to include the simulation of dispensing nor team application-based learning. Donohoe et al. reported the inclusion of a case-based discussion but also did not appear to include a simulation of dispensing. In addition to the differences described above, the previous articles also do not address the stigma associated with naloxone dispensing. Though Kavanaugh et al. incorporated simulated activities based on real-life scenarios that pharmacists may encounter, the simulations included academic detailing to respond to provider barriers and did not include scenarios where patient barriers required identification and consultation. Bachyrycz et al. assessed student attitudes toward prescribing of naloxone but this does not directly translate to stigma. Furthermore, our study is the only one that discusses the use of simulated prescription entry on a pharmacy software for students to practice the documentation and prescription processing piece of naloxone furnishing. Our study was also one of the two that assessed student knowledge and comfort, specifically with furnishing naloxone, in addition to the study by Kavanaugh et al.Our opinion-based surveys had excellent internal consistency as demonstrated by the Cronbach’s alpha score. Based on our data, it was determined that students found most benefit from the in-class lecture and team application-based scenarios. Of the students surveyed after the completion of the in-class naloxone education training and the TBL application session, a significant improvement in confidence, knowledge, and comfort in educating and counseling patients on naloxone was observed. The summative assessments were found to provide further improvement in student-reported knowledge and comfort with naloxone furnishing, though to a lesser extent than the in-class lecture and team application-based scenarios. Though students’ perceived benefit from the summative assessments were not as strong, it allowed for a structured and objective assessment of students’ skill and knowledge in following a BOP protocol on furnishing naloxone and also on providing patient counseling. In addition, the modified APhA patient counseling rubric used to score the students could easily be implemented by other colleges of pharmacy to objectively grade student performance on naloxone counseling.
Limitations that were identified include the small total number of participants (n = 68) that completed all three surveys and the subjective nature of Likert questions that might allow for students to have an unrealistic understanding of their knowledge or comfort with furnishing naloxone. Survey fatigue may have contributed to the lower number of students completing all three surveys, since two were completed on the same day and the last completed just one week later. Though awareness of stigma was addressed through one of the application-based cases and through patient counseling, it was not assessed within the survey questions. Moreover, the case-based scenario summative assessment included only six points and did not include questions on all of the available naloxone products. For future offerings of the training, we plan to improve these limitations through the inclusion of more questions on the survey that specifically assess stigma. Though the patient case assessment was comprehensive, we plan to make further enhancements to increase the number of points available for the assessment and allocate points based on the difficulty of the question. We also plan to include questions for all of the available naloxone products to better assess knowledge and comfort with each formulation available. In addition, we plan to require remediation for all students that do not pass the summative assessments. Though the average grades for each of the three summative assessments was a grade of B or higher, there were students that did not successfully pass at least one of the three assessments. Because the syllabus for the course did not outline a remediation plan, we were unable to require remediation for these.
留言 (0)