1. IntroductionDengue (DENV) continues to be the most important viral vector-borne disease with large morbidity and mortality in Latin America and South-East Asia. Dengue is an arthropod-borne viral disease caused by four dengue virus serotypes (DENV 1-4) transmitted by species of Aedes mosquitoes, particularly A. aegypti, A. albopictus, and A. vittatus. Dengue is endemic in more than 100 countries in Southeast Asia, the Western Pacific, Africa, the eastern Mediterranean regions, and the tropical Americas. Additionally, autochthonous occurrences in southern Europe are a consequence of climate change. Its incidence has multiplied in the last 50 years [
1]. In 2017, there were 580,640 dengue cases (254,453 in Brazil, 89,893 in Mexico, and 76,093 in Peru), with 561,356 in 2018 (265,934 from Brazil, 78,621 from Mexico, and 44,825 from Colombia). According to WHO, in 2020, they reported 2,300,558 cases in the Americas region [
1]. In 2022, up to November 7, 2022, 2,499,358 cases had been reported in the Americas, with an incidence of 252.00 cases per 100,000 pop., 3641 cases of severe dengue (0.1%), and 1135 deaths for a case fatality rate of 0.045% (
www.paho.org (accessed on 8 November 2022)).In the case of Honduras, a Central American country with environmental and social conditions, is prone to vector-borne diseases, including those caused by arboviruses, such as DENV [
2,
3]. Factors such as temperature, vector bionomics (survival, density, frequency, and feeding behaviour), extrinsic incubation period, and vector competence can affect DENV transmission [
4].Multiple arboviruses, primarily alphaviruses, are related to chronic rheumatic manifestations, especially chikungunya [
5,
6]. Other alphaviruses, such as Mayaro and o’nyong-nyong viruses, may produce chronic rheumatic consequences [
7,
8]. The Mayaro virus is an arthritic alphavirus; the infection leads to a disease such as DENV; and there is the susceptibility of human chondrocytes, fibroblast-like synoviocytes, and osteoblasts, which are the main types of cells involved in osteoarthritis [
9]. Viral load accumulates to the point that generalized clinical symptoms (fever, headache, and myalgia) develop, presumably secondary to an antiviral state of the host in which the expression of interferon is abundant [
10]. Furthermore, arboviral infections are frequent causes of febrile illness [
11]. In addition to alphaviruses, flaviviruses, including DENV, may also produce acute and non-acute rheumatic manifestations [
12,
13], although they have been poorly studied.DENV virus infection can lead to asymptomatic or symptomatic infection. Approximately 20% of all patients are symptomatic, and individuals experience symptoms of the disease that cover a broad clinical spectrum from non-severe to severe clinical manifestations. The disease caused by DENV has an abrupt onset with three widely identifiable phases: febrile, critical, and recovery [
14]. Typical symptoms include a fever that can exceed 39 °C and polyarthralgia. Symmetric bilateral arthralgia is found in most patients and is usually located in the peripheral joints, appearing shortly after the onset of fever (2 to 5 days) [
15]. Arthritis is defined as pain with swelling of the joints, while arthralgia often refers to joint pain. However, the use of these terms is often not well defined.Rheumatic diseases can contribute to a severe course of dengue, although their contribution has not been previously characterized [
16]. Chikungunya is a disease, different from dengue, that would progress to a chronic phase, mainly producing chronic inflammatory rheumatism in about half of the patients; according to recent estimates and measurements in Latin America, co-infections between dengue and Chikungunya can occur and have already been reported [
3]. A study in Tolima showed that approximately half of the patients persisted with post-CHIK arthralgia (arbovirus) after 24 weeks of follow-up [
17]. In Chikungunya, possible causes of chronicity in arthralgia are viral persistence, genetic predisposition, induction of autoimmune diseases, tissue damage caused directly by the virus, and exacerbation of a pre-existing joint condition [
18]. Chronic musculoskeletal symptoms, which are likely to be mediated by inflammation potentially resulting from viral persistence, may reappear or persist for more than three months after the acute phase of the disease [
19].The 28 Joint Disease Activity Score (DAS-28) is essential for clinical practice and research, incorporating swollen and sensitive joint counts [
20]. The Arthritis Index from the Universities of Western Ontario and McMaster (WOMAC) is a self-administered health status measure that assesses pain, stiffness, and function dimensions. It produces three subscale scores (pain, stiffness, and physical function) and one total score (WOMAC index) that reflects disability in general [
21].
The present study was carried out in two hospitals with Dengue units located in the northern part of Honduras, in the department of Atlántida (“Hospital General Atlántida”) and in Yoro (“Hospital Manuel de Jesus Subirana”), in conjunction with an intermediate patient care centre (“Centro Santiago Apostol Health Department”). We were wondering if the participants diagnosed with dengue during the 2019 epidemic presented joint involvement by completing the evaluation questionnaires for rheumatic diseases in the WOMAC and DAS-28.
2. Methods
The present research is a prospective study of a cohort of participants who were diagnosed with dengue in the emergency unit or dengue unit of the General Hospital Atlántida, the Santiago Apostol Comprehensive Health Center in Yoro, and the Manuel de Jesús Subirana Hospital in Yoro in the period from December 2019 to February 2020, which corresponds to Phase I, and from March to June 2020, which corresponds to Phase II.
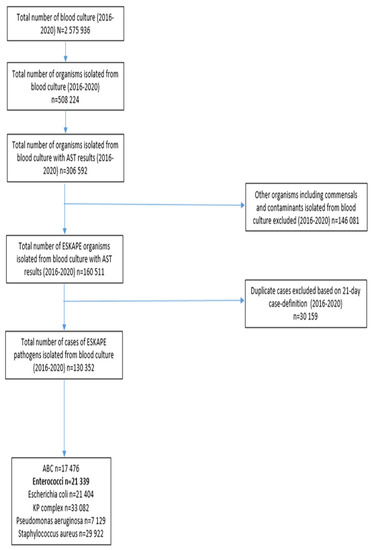
2.1. Inclusion CriteriaParticipants who had met the dengue case criteria included participants who were between 18 and 60 years of age with a diagnosis of dengue and participants who voluntarily agreed to participate in this study through informed consent (
Figure 1). For Honduras, the definition of dengue is a patient with a feverish illness of sudden onset, lasting up to 7 days, with two or more of the following manifestations: headache, myalgia, arthralgias, retro-ocular pain, skin rash, leukopenia, presence or absence of bleeding, and confirmed by a laboratory test, including serology or PCR for DENV. 2.2. Exclusion CriteriaPregnant participants, participants under 18 years of age and over 60 years of age, participants who did not meet the dengue case definition, participants with previous autoimmune or rheumatic diseases, participants without national documentation for identification and without telephone contacts for follow-up, complicated severe dengue cases: severe dengue shock, liver failure, kidney failure, adult respiratory distress syndrome (ARDS), and death (
Figure 1), and patients with suspicion of coinfection (e.g., CHIKV) were excluded. 2.3. Study Phases
Recruitment Phase (3 months): It was carried out on all participants with a dengue diagnosis treated in the assistance centres or dengue units. In this recruitment phase, there were n = 957 participants, of which n = 542 were excluded by the following criteria: Pediatric patient (n = 428), pregnant (n = 9), over 60 years old (n = 75), resigned to participate (n = 14), no identification (n = 1), patient with severe dengue (n = 5), postpartum (n = 4), participant with down syndrome (n = 1), arthritis rheumatoid (n = 2), death (n = 1), no contact number: (n = 2). Participants who managed to enter this study were n = 415.
Follow-up phase (4 months): All study participants were located by telephone through a private project line available in the informed consent given during enrollment. When we contacted the participant, the WOMAC and DAS-28 questionnaires were applied again through a telephone interview. In this phase, there were participants who continued with the follow-up (n = 281), and there were participants who did not continue (n = 134) because they did not answer the scheduled telephone calls or had their cell phones disabled.
The project included an email in the Gmail account (
[email protected]) that allowed answering questions, making comments, or making changes to the telephone number. 2.4. Analysis of Data
Obtaining a sample is affected by the statistical application GPower 3.1. We used a multivariate analysis and the T student and Chi-square tests. The instruments were obtained using the Google Forms application. They were entered and subsequently analyzed in the SSPS version 25 program for the MacBook.
2.5. Ethical Considerations
This study was conducted under the Declaration of Helsinki. This research’s preparation and execution fully complied with the fundamental ethical principles of autonomy, justice, beneficence, and non-maleficence. Act Number 2019062, approved by the Ethics Committee in Biomedical Research (CEIB) of the National Autonomous University of Honduras (UNAH), meeting on 11 December 2019.
The protocol was approved by institutional authorization in writing from the General Hospital Atlántida, La Ceiba, Atlántida; Manuel de Jesús Subirana Hospital; and Santiago Apóstol Comprehensive Health Center in Yoro. Written informed consent was obtained, and a copy of the informed consent was given to each participant, explaining the objectives of the project and her voluntary participation in the evaluations through questionnaires. The information was obtained from interviews conducted by members of the research team trained in applying rheumatological assessment scales (WOMAC and DAS-28). There were no potential risks to the participant during the process, and they had no direct benefits from the research; however, the information obtained will serve to understand arbovirus diseases and their relationship with chronic degenerative diseases such as osteoarticular involvement in an increasingly exposed and aged population. Upon completion of the follow-up phase, participants who were presented with any health problem associated with rheumatological sequelae will be referred for specialized medical care in the local hospitals.
3. ResultsThe group of participants was made up of 58.8% women and 41.20% men and an average age of 33 years, with 24.59% having completed secondary education; in terms of occupation, housewives are the most affected, with 61.07%, followed by 19.88% farmers and 0.41% transport employees being the least affected by the illness (
Table 1).Based on the results obtained, the inference is made that the functional limitations or symptoms related to daily physical activity post-dengueoccur in a higher proportion in the female sex, as assessed by the WOMAC questionnaire (
Table 2). These symptoms or functional limitations when performing daily activities, comparing women vs. men (significantly higher among the firsts, pFinally, at DAS-28 (
Table 3), the total number of patients, in most of whom this questionnaire was assessed (228), showed at least one alteration in 14.91% of the patients, significantly higher among women (22.2%) (p = 0.001) (
Table 3). Although 9.65% presented between one to ten joints with inflammation or pain, 4.39% presented from 11 to 30, and 0.88% presented more than 30 altered joints, with no significant differences by gender. Assessing each joint specifically for inflammation or pain revealed that the knee was the most affected, with significant differences by gender, especially with pain; from women, 16.67% presented pain at the left knee and 15.87% at the right knee (
Table 3). For eight joints, the proportion of those with inflammation was significantly higher among women (pp
Table 3). 4. DiscussionArboviral diseases continue to be a significant public health threat in the world, in endemic and non-endemic areas, due to migration and climate change, which have allowed local transmission in non-endemic territories [
22,
23]. In South-East Asia and Latin America, its burden is significant, with endemic areas presenting periodical epidemics, as is the case of Honduras in Central America [
2,
24]. The chronic consequences of dengue have been poorly studied, including the rheumatic sequelae and manifestations in different populations [
12,
13,
25,
26]. In fact, there are no studies of the follow-up of DENV patients after the acute phase of the disease. In addition, dengue, more than any other arboviral disease, will be the cause of new outbreaks and epidemics in the near future in Honduras and other Latin American countries. During 2019, DENV-1 and DENV-2 were the circulating serotypes (
www.paho.org (accessed on 8 November 2022)); nevertheless, it is important to remember that only a small number of confirmed cases of DENV are sequenced, cultured, and serotyped.The present study suggested that the non-acute DENV affectation, according to the WOMAC questionnaire, was high during the epidemic in Honduras in 2019. Of the 286 participants who continued the follow-up, 63.02% presented with symptoms. Primary joint pain was observed when walking. Comparing arthralgia was more frequently reported by studies in patients with CHIKV, 84.6% [
11], as expected as a classical arthritogenic arbovirus, but less assessed and observed with dengue. Unfortunately, until 2022, no studies have used the WOMAC questionnaire to assess patients affected by DENV. However, not in Chikungunya and Zika either. Follow-up of DENV patients is important, based on the current findings.According to the WOMAC questionnaire, we also refer to the group with the most significant affectation as being female (58.76%) compared with a meta-analysis of the Zika virus, where the cases that reported signs/symptoms of arthritis were primarily women, which represented 66.7% of the participants from 129 patients [
27]. In addition, our study estimated an average mean age of 32 years, compared to dengue cases (median age 24.8 years) [
19].Severe joint pain and stiffness are the hallmarks of arthritogenic alphaviruses [
9]. Therefore, the results could be obtained that they presented with severe pain when performing the following activities as walking (63.023%), pain when going up or down stairs with (25%), pain at night when in bed (19.80%), pain when sitting (20.45%), and pain when standing (24.02%). Additionally, concerning stiffness, we obtained that joint stiffness upon awakening was 19.15%, together with stiffness throughout the day was 10.71%.DAS-28 allows us to observe that a significant proportion of women with joint inflammation and pain, which is higher than zero, is, in general terms, unexpected; showing that dengue may also lead to the development of chronic rheumatological findings, maybe in the lower proportion that CHIKV, but still affecting the everyday life of patients and, consequently, their quality of life. This issue should also be assessed in further studies of post-dengue long-term assessment. For example, a study in Mexico in 2017 using the DAS-28 considered the change between the diagnosis and follow-up of patients with CHIKV infection [
28]. This study found that DAS-28 was significantly low at follow-up, indicating chronic compromise. Unfortunately, in DENV, such tools as the DAS-28 have not been previously used and published in the literature until 2022.




留言 (0)