
記住我
Diabetic foot ulcers (DFUs) contribute significantly to morbidity and mortality associated with diabetes and are extremely costly to health services.
Effective foot self-care behaviors are an important, low-cost approach to reducing the likelihood of DFU development; however, patient adherence to advice is low, and reasons for this remain unclear.
Patients typically only adopt good foot self-care behaviors once DFUs have developed, which is often too late to prevent future occurrence of amputation.
WHAT THIS STUDY ADDSPatient motivation for foot self-care is generated through personal or vicarious experience and fear about the consequences of diabetes.
Healthcare professionals (HCPs) often focus their time on factors that patients do not link to motivation, such as increasing patient knowledge.
Non-foot specialist HCPs displayed an apparent insecurity around their own foot health knowledge which led them to avoid foot self-care discussions.
There was discrepancy between patients and HCPs about who patients should seek out when a foot problem arises.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICYHCPs should support more autonomous motivation for individuals in pursuit of self-care, including: acknowledging barriers; recognising patients’ lived experiences and helping them to develop a personally meaningful rationale for undertaking necessary health behaviors.
There should be renewed focus on developing consistency of messaging by HCPs.
This is both in terms of who the most appropriate HCP is to present developing foot problems to initially, as well as clarifying the roles and responsibilities of HCPs and patients around foot care.
The benefit of foot-specific training being provided to non-foot specialist HCPs should be explored.
IntroductionFor a person with diabetes, the lifetime incidence rate of a diabetic foot ulcer (DFU) is between 19% and 34%, with a yearly incidence rate of 2%, and are the leading cause of non-traumatic lower extremity amputations.1 This is of more striking significance when contextualized by the fact that there is a 45%–57% risk of death within 5 years of a diabetes-related amputation.2 3 It has even been suggested that preventing DFU development is the way to reduce diabetes-associated mortality.4 Accordingly, ever-increasing importance is given to strategies aimed at preventing the development of DFUs—so much so that the James Lind Alliance in partnership with the National Institute for Health and Care Research identified this as one of the top 10 foot health research priorities in the UK.5 Likewise, a Delphi study of key stakeholders in Australia identified that education to improve self-care practices was one of the key priorities for future research to improve diabetes-related foot health and disease.6 With appropriate disease management and effective self-care behaviors, many complications, including DFUs, are deemed to be entirely avoidable.1 3 7 8 While the role of the HCP in helping patients to effectively manage their diabetes remains a crucial aspect of diabetes care, the International Working Group on the Diabetic Foot has cited good foot self-care behaviors as a key approach to prevent the development of DFUs.1 Despite this, a large integrative review identified that HCPs frequently report that foot self-care behaviors are not undertaken consistently enough by people with diabetes.9 Given the harms and costs associated with diabetic foot disease, all approaches that may help to reduce the incidence and prevalence of this require urgent investigation—not least efficacious and cost-effective measures such as appropriate foot self-care behaviors.
Self-care has been defined as the actions an individual takes in managing the symptoms associated with a chronic condition through physical activity and other lifestyle changes.10 In diabetes, self-care is a well-established facet of achieving optimal disease management and clinical outcomes because most of the day-to-day care and management of the disease is handled by patients and/or their families.11 The American Association of Diabetes Educators12 identified seven essential self-care behaviors in diabetes which predict good outcomes, viz.: healthy eating; being physically active; monitoring blood sugar; compliance with medications; good problem-solving skills; healthy coping skills and risk-reduction behaviors (which includes reducing risk of foot ulceration via good foot care). All of these behaviors positively correlate with good glycemic control, reduction of complications and improvement in quality of life.11 13–15 Although patients need to be the ones to act, support from healthcare professionals (HCPs) on what to change and encouragement to maintain changes has been shown to increase confidence and facilitate sustained self-care behaviors.16
Optimal foot self-care behaviors include: daily washing and drying of the feet; daily visual foot examinations; application of skin moisturizer; avoiding walking bare-footed (even within the home); ensuring that bathing water is not too hot; attending regular professional foot care and following professional advice in relation to foot care behaviors.17–21 Despite self-care being widely considered to be the most cost-effective way of managing diabetes and delaying or preventing of the development of associated complications, it is often found lacking in people with diabetes and is sometimes also underappreciated by HCPs.22 Evidence indicates that foot self-care behaviors, specifically, remain underused in the prevention of DFUs.9 11 17 23–25 Mogre et al26 undertook the only large systematic review to date that included adherence to foot self-care behaviors within a range of self-care practices in diabetes. Their review of 72 studies included 10 that specifically looked at foot self-care behaviors in a pooled population of over 1600: 40% of people with diabetes undertook regular foot inspections and just 10% met the criteria of having ‘good’ foot self-care practices. In comparison, adherence rates of 58% for diet; 71% for medication taking and 41% for exercise behaviors were reported. While this review was limited to low-income and middle-income countries, the findings were largely consistent with the literature on foot self-care behaviors in many different countries—including high-income ones.17 23–25 27
It appears that adherence to recommended self-care is limited at best, and that this is a multidimensional phenomenon involving social, economic, patient-related, health system-related and condition-related factors.28 In particular, the complex interplay between the known contributory factors of socioeconomic status; patient knowledge; patient education; patient beliefs; social support; HCP-patient interactions and health service experiences is where there is a need for further understanding.29–34 Additionally, studies that have identified issues of confusion and trust between patients and their HCPs in relation to foot self-care,32 have not explored areas of consensus and tension that may exist and whether they may contribute toward any perceived barriers and facilitators to foot self-care in diabetes. Therefore, this study sought to explore patient and HCP perspectives on barriers and facilitators toward patient foot self-care behaviors in adults with diabetes currently at low risk of developing a DFU. This demographic is an important one to assess as in the context of diabetes, low-risk populations tend to become high-risk in time and the establishing of good self-care behaviors are more effective if employed earlier in the disease progression.9 17
Research design and methodsThis sequential, three-phased qualitative study explored patient and HCP perspectives on perceived barriers and facilitators to foot self-care behaviors in diabetes. The design of each phase is outlined below. The lead researcher in this study is a podiatrist and so the potential impact of this in terms of influencing participant responses and/or the interpretation of the findings was a key consideration. Accordingly, measures to account for—and minimize the impact of—this potential bias are detailed in the methods below.
Phase IDesignSemi-structured interviews relating to foot self-care behaviors and perceived barriers and facilitators to these behaviors were undertaken with individuals with diabetes. In-depth interviews were selected as the most appropriate approach to this phase as they allow for deep and meaningful data to be generated and to obtain the participants’ accounts as personal stories to help drive and shape the meaning of the data that emerge from them.35 The interview schedule was devised by the lead author based on findings and gaps from past literature review and professional expertise. Once initially designed, this was then refined via discussion between all the authors of the study.
Recruitment and procedureParticipants were opportunistically selected and recruited from Berkshire Healthcare NHS Foundation Trust and interviewed between February and July 2020. Eligibility criteria can be found in table 1. Access to participants was via a gatekeeper within the trust. This gatekeeper was a diabetes specialist nurse based out of one health centre. Participants were verbally invited to take part during scheduled clinical appointments and provided with a letter by the diabetes specialist nurse gatekeeper. The letter detailed information about the study and had an accompanying consent form and an explanatory participant information sheet. Potential participants were given time to go away and read these forms and decide if they would like to volunteer to take part. If approached individuals decided that they did want to take part in the study, they completed and signed the consent form and returned it to the gatekeeper who, in turn, provided that to the researcher along with contact details of the volunteer(s) who gave consent to be contacted. All participants were reassured that they were free to withdraw from the study at any point and that not participating in (or withdrawing from) the study would not impact on the care that they received. Volunteers were contacted by the lead author, and interviews arranged via telephone or skype, depending on participant preference.
Table 1Eligibility criteria for study participants
AnalysisInterviews were transcribed, coded and subjected to interpretative phenomenological analysis (IPA).35 Respondent validation of the transcripts was employed for all participants prior to any analysis taking place. Participants were given 3 weeks to request any corrections be made to their transcripts once returned to them. If no comments were received in this timeframe, it was assumed that the transcript was a true and accurate account of the interview. Next, the lead author familiarized himself with the transcripts, and generated individualized narrative accounts for each case to create detailed experiential themes. Subsequently, any patterns across cases were searched for. The coding was single-phased and undertaken by the lead author following immersion with the raw data. These codes were created by the lead author and presented to the coauthors along with copies of the transcripts and discussion between the authors allowed for these codes to be interrogated. Once refined and agreed, these codes were then clustered into topics, subthemes and themes by the lead author. These, too, were subject to interrogation and discussion among all the authors to ensure that the findings from this phase were dependable and trustworthy and bias from the lead researcher was reduced as much as possible.35 36 The lead author took a reflective and reflexive approach to the analysis of the data to ensure that his biases were accounted for in the interpretation of the data. Emerging topics and themes from these interviews provided topics to guide the interview schedule for phase II.
Phase IIDesignA second phase of in-depth, semi-structured interviews about foot self-care in diabetes were undertaken with HCPs. The processes followed for devising the interview schedule was the same as for phase I except that the findings from phase I were an additional basis for some subjects/questions asked in the phase II interviews.
Recruitment and procedureHCP participants were purposively selected and recruited through Berkshire Healthcare NHS Foundation Trust (via an appointed gatekeeper within the trust) and the private sector (via appeals for participants on HCP research volunteer fora) between August and December 2020. Eligibility criteria are located in table 1. Consent was obtained via potential participants being presented with a participant information sheet and a consent form for them to read, sign and return if they agreed to take part in the study. All participants were reassured that they were free to withdraw from the study at any point. In order to yield HCP perspectives on foot self-care behaviors in diabetes that has not been influenced by the phase I findings, the patient perspectives were only presented to the HCPs in the second half of their interviews. HCPs were given several minutes to reflect on the findings from the patient interviews before these were explored with the HCP participants.
AnalysisThe data from these interviews were transcribed, coded and thematically analyzed using IPA to allow for both a standalone account of the HCPs’ perspectives as well as initial identification of any areas of consensus and/or tension between the HCP and the patient perspectives. The processes followed in the data analysis were the same as they were for phase I. The topics and themes from this phase combined with those from phase I to contribute to the interview schedule for phase III.
Phase IIIDesignThe third (III) phase saw phase I and II topics and themes presented back to patient participants for discussion within two patient group interviews. The purpose of this phase was to identify areas of consensus and tension in patient and HCP perspectives on foot self-care in diabetes, and gain patient perspectives of whether these could contribute to low engagement in these practices.
Recruitment and procedureAll participants from phase I were invited to take part. As not all phase I participants accepted the invitation, new participants were recruited via Berkshire Healthcare NHS Foundation Trust in order to increase the participant pool. The eligibility criteria; access to participants and measures to obtain valid, informed consent were identical to the process for phase I. The two types of participants (returning, new) were interviewed in two separate groups. The interviews took place between February and March 2021. The processes followed for devising the interview schedule was the same as for phases I and II except that the findings from phase II were an additional basis for some topics/questions asked in the phase III interviews.
AnalysisThe data from the discussion within the group interviews was then transcribed, coded and analyzed using a simple thematic analysis framework consistent with a hermeneutic phenomenological approach.36 Following the phase III group interviews, respondent validation was once again used for the transcripts (as for phases I and II). Following this, the transcripts were initially coded using codes that were generated during the phase I patient interviews. Using these codes allowed for the identification of topics and subthemes that were consistent with the phase I interviews. However, any new insights that emerged from these group interviews that were distinct from the findings from phase I were coded. If these appeared pertinent to the study aims, they were then collected into codes and, ultimately, themes to be considered. The coding and clustering of topics, subthemes and themes was undertaken by the lead author and openly and continuously discussed with the coauthors to allow for them to be suitably interrogated for trustworthiness and for any researcher biases to be minimized. Furthermore, the reflexive and reflective approach to analysis occurred in phase III as it did for phases I and II.
ResultsDetails pertaining to the recruited participants for phases I, II and III of this study can be seen in table 2 and table 3, respectively. All participants names used in this article are pseudonyms.
Table 2Phase I and III (patient group interviews) sample characteristics
Table 3Phase II (HCP participant) sample characteristics
Patient perspectivesPatient responses derived from phases I and III of the study indicated that they felt that they needed to be motivated and enabled to undertake good foot self-care behaviors.
MotivationThe main factor that underpinned patient motivations toward foot self-care was concerns over the consequences of diabetes. The concerns that the patients interviewed had about the consequences of their diabetes comprised their personal experiences and history of living with diabetes; stark health messaging from HCPs that attempted to drive home the seriousness of their condition and their vicarious experiences of diabetes (ie, witnessing their loved one’s experiences of serious diabetes outcomes). The patients interviewed connected these experiences with worries and concerns that they had about the consequences of their diabetes and the subsequent vigilance that they have developed about their health (including that of their feet) and associated this experience with their own motivation to adopt appropriate self-care behaviors.
[Ian]: I was very, very ill…I am concerned about what could happen. I am really quite attached to my feet and I do keep an eye on them…given my experiences of diabetes I am quite aware of what can happen.
[Felicity]: I saw what my nan went through with it—she lost her leg because she had a sore and she got gangrene and…I think, she had a stroke and I think it was related to her not controlling her diabetes well enough…I feel that I need to make sure that I am looking after myself a lot better.
Those without such personal experience, however, did not appear to consider themselves particularly susceptible to foot problems in diabetes and did not appear to have a personally meaningful reason to adopt foot self-care behaviors. Indeed, they appeared to question the veracity of the foot self-care advice they were given as it did not align with their own lived experiences.
[Arthur]: I didn’t know I had diabetes and I still don’t know I have diabetes. Except now they are telling me that I am losing some sense in my feet…I don’t notice any difference. I can’t see what they’re telling me about my diabetes…I don’t think I would cream my feet. Not unless somebody could give me a very good reason why…I cannot see any reason why I should start creaming them.
EnablementPatients talked about two criteria that needed to be met for them to feel able to adopt self-care recommendations; being informed and being resourced.
‘Being informed’ was noted in the testimonies of those who spoke positively about their experiences of targeted patient education as well as those who bemoaned a perceived lack of it.
[Erica]: I have had a lot of information and a lot of help from the doctor and nurse that I see. The DEAL course was also excellent. In fact, the importance of moisturising your feet was something that came up in that course and I do now keep my feet creamed. So, I think that the discussion that we all had about that and the nail cutting and things like that have definitely been helpful.
[Felicity]: As you are not seeing the same doctors all the time and the ones you see may not always tell you everything, so having something that you get when you are newly diagnosed or whatever that covers everything would be really good. If you don’t know what you should be doing you often end up doing nothing in case it is wrong.
‘Being resourced’ as a contributory means of undertaking foot self-care behaviors covers both external resources and personal resources. Patients identified their need for external resources such as an effective working relationship with HCPs and help afforded by technological/specialist equipment.
[Brenda]: I have always felt that if I am worried about something, there was always somebody at the practice that I could go to, to ask. When I do, they would see me, they would check whatever it was that I was concerned about and, sort of, reassure me… That’s been good.
[Ian]: Now I use a Dexcom G6 glucose blood monitoring system. That is amazing and it really has improved my life beyond belief. Not only that but my wife has the App on her phone as well and so I am incredibly secure in the knowledge that I am a lot safer now…the technological solutions have been fantastic and have really improved my life drastically. More than anything else.
The personal resources they considered important included time and the physical capability to tend to the feet.
[Brenda]: Everything always seems to be done in a rush. So that is one thing that I have found—that it has been difficult to manage time.
[Harriet]: I also have a bad back so I cannot get down to my feet that easily, so I find that I cannot cut my nails and as you get older your nails get stronger. I also have arthritic hands.
Healthcare professional perspectivesThe two main themes to emerge from the interviews with the HCPs centred around ‘HCP beliefs about patient self-care behaviors’ and their ‘perceived barriers to effective care’.
Healthcare professional beliefs about patient self-care behaviorsHCP beliefs about what predicts foot self-care behaviors, and their awareness of patient-specific circumstances played a role in shaping how they sought to optimize the care they provided. Four predictors for self-care behaviors that may influence practice were raised by HCPs based on their clinical experiences: the state of the patients’ glycemic control; patient age; diabetes type and patient fear of the consequences of diabetes complications. Of these, only fear of the consequences of diabetes complications was recognized by all the HCPs interviewed. Furthermore, some of the HCPs interviewed assumed that fear of consequences is associated with motivation and therefore considered it logical to use stark health messaging as a means to increase patient motivation.
Pamela (GP): I think it can be quite simple in many ways, if people are concerned or worried about a particular aspect of their health then they’re probably concerned enough to follow through on the treatment or advice that you give them. It makes the conversation easier in many ways.
HCPs demonstrated awareness of patient-specific circumstances that could impact on self-care behaviors, which included recognition that physical limitations and psychological difficulties can seriously affect somebody’s ability to undertake effective self-care behaviors. Some of the HCPs discussed how they had tailored their communication and practices to more effectively advise and guide patients, differentiating according to each patient’s situation.
Jessica (nurse): My advice depends very much on the person because sometimes something that I might consider to be really simple could actually be quite a mind-set change for some people…I mean just because it is easy for me does not mean that it will be easy for them and so I need to shape my advice with that in mind.
Perceived barriers to effective careHCPs expressed frustrations about what they perceived to be barriers to effective care, which they believed influenced their practice. These were: patient attitudes and behavior; a lack of effective, consistent patient education; service limitations and an insecurity of own foot health knowledge.
HCPs differed in their opinions around the division of foot care responsibilities, with some HCPs bemoaning a lack of patient self-care behaviors, implying patients did not take on enough personal responsibility, while others indicated that patients did not bring foot health problems to the attention of HCPs and seek professional advice early enough.
Kevin (podiatrist): You do get the ones who won’t do what you have asked and instead would just happily come back to see you and let you do it even if you tell them a hundred times that they need to do it every day…Yeah, it gets a bit frustrating.
Mary (podiatrist): We are always trying to advise them to call us asap if there are any problems or any warning signs, but…the amount of times that we have had people come in with sepsis and they have been ill for a week or so and just didn’t call us even though we have told them time and time again. It is like it just goes over their heads. I find it quite hard and frustrating.
There were also differences in beliefs around the reasons why current service provision does not result in sufficient foot self-care; some HCPs perceived this to stem from the lack of effective and consistent patient education.
Mary (podiatrist): Patients first get screened by nurses and maybe healthcare assistants, and I think that education should start there regarding their feet as I am not sure that it really does currently. I mean, a lot of them do not know about foot ulcers and until they come to us for one thing or another and then I may say to them “do you know what a foot ulcer is?” and they don’t have a clue.
Mary further pointed to the inconsistency of professionals managing the foot in diabetes as a contributory factor to barriers to effective foot care in diabetes:
Mary (podiatrist): Sometimes these patients don’t get that consistent education or someone who they’ll see consistently who will be there for them as support. Also, you get a clash of clinician advice and that makes it really difficult. Different people changing the dressings and different people have different ideas of how to manage it and that makes it difficult for the patient as well.
The non-foot specialist HCPs interviewed (ie, diabetes specialist nurses and GPs) indicated a further barrier, of being insecure about their foot health knowledge, which was a key reason that these practitioners did not speak to patients about foot health more frequently. Instead, they tended to signpost patients toward podiatrists for foot-specific advice and guidance, despite finding that getting patient access to podiatrists was not always easy or possible.
Omar (GP): I’d typically pass foot problems to the Podiatry department and they would be the ones more focused on the foot care practices of the individuals concerned. The nurses may play more of a role there too.
Jessica (nurse): I know that it is the bit that is sometimes difficult—you know, timely access to healthcare professionals…I think it is really quite easy for small wounds to escalate to something more serious because people will not have ease of access to care sometimes.
DiscussionThis study sought to explore the perspectives of patients and HCPs on barriers and/or facilitators to foot self-care behaviors in diabetes and areas of consensus and/or tension between patient and HCP perspectives. While previous studies have found that foot self-care behaviors in diabetes may be influenced by how much concern people have about their feet, this is the first study that the researcher is aware of that has been able to expressly link motivation to these behaviors from patients’ personal and vicarious experiences. Moreover, other apparently novel findings from this study were that: HCPs often focus their time on factors that patients do not link to motivation (such as increasing patient knowledge); non-foot specialist HCPs displayed an apparent insecurity around their own foot health knowledge which led them to avoid foot self-care discussions and that there was discrepancy between patients and HCPs about who patients should seek out when a foot problem arises.
Patient perspectivesThe finding that motivation toward self-care is influenced by the amount of concern an individual feels toward the aspect of their health in question is consistent with past qualitative studies seeking to understand the perspectives of people with diabetes.37–39 However, the consideration that this concern is a product of past experience (personal or vicarious) and that HCPs warnings and advice relating the importance of self-care is likely enhanced if their messages reflect these patients’ lived experiences appears to be a novel contribution of this study to the literature.
Around the theme of enablement arose the notions of being informed and being resourced. A closely intertwined relationship between self-efficacy and being suitably informed has been found in previous studies,40 41 where the confidence persons have in their own ability to perform a task tracked closely with how well they felt they have been educated about performing that task. Connecting back to the other theme of motivation, it emerged strongly in our patient interviews that those who had the greatest levels of concern around diabetes consequences were the ones who reported seeking out information. This could suggest that for these individuals, information seeking provides a possible connection between motivation and enablement in the context of self-care behaviors. As patients acknowledged the importance of both motivation and enablement for them to be more likely to undertake good foot self-care behaviors, these findings highlight that these factors may be separate, yet interdependent. This is consistent with the capability-opportunity-motivation-behavior model in which motivation and enablement (capability) are presented as being two of three central factors which are needed for any particular behavior to emerge.42 On a practical level, awareness of this dynamic could mean that HCPs seek to appraise factors of both motivation and enablement (rather than either/or) in any given patient context to see if practical support and advice could help patients initiate and sustain good foot self-care behaviors.
HCP perspectivesThe two main themes from the interviews with the HCPs centred around HCP beliefs about patient self-care behaviors and their perceived barriers to effective care. HCP beliefs about patient self-care behaviors most frequently linked poor adherence of patients with a lack of motivation and, consequently, they focused their communication around ways to improve motivation; yet few reported exploring this assumption with patients (eg, asking them if they struggled to find motivation) as noted in previous studies.43 This suggests that some of the HCP’s efforts to try and increase motivation were not informed by patients’ views which may go some way to explaining the proclivity some HCPs had toward stark health messaging, even if the effectiveness of this strategy is not evident in the literature.44 Indeed, patient participants in our study indicated that they often found stark health messaging to be unhelpful and demotivating.
The perceived barriers to effective care that HCPs offered varied, including: differing perspectives on the division of foot care responsibilities; a perceived lack of effective and consistent patient education; limitations to service delivery; inconsistent personnel; ineffective communication between HCPs and non-timely access to specialists. It is plausible that the differences between HCPs’ views could contribute to the mixed messaging perceived by some of the patients in this study. In turn, this may create uncertainty for patients regarding the division of responsibility for aspects of their foot care. A study by McInnes45 that explored diabetes-related foot care knowledge of podiatrist and non-podiatrist HCPs also reported a lack of consensus between these groups, and more incorrect beliefs and understandings about foot health in diabetes among non-podiatrists. Aligned with the findings of our study, this may be an area worthy of further research as this could suggest that patients are not being routinely steered toward foot health conversations with the HCPs they present to most often and may not be getting early or frequent enough access to the HCPs best placed to have these conversations with them (podiatrists).
Areas of consensus and tensionFigure 1 diagrammatically presents the areas of consensus and tension between patient and HCP perspectives. In this study, consensus between participant groups is determined as having occurred where the general points made by participants are consistent with each other, with few areas of disagreement. Across the patient and the HCP interviews, the four main areas of consensus between these participant groups were: concerns over consequences; importance of patient education; importance of effective patient-HCP communication and frustrations related to the health service.
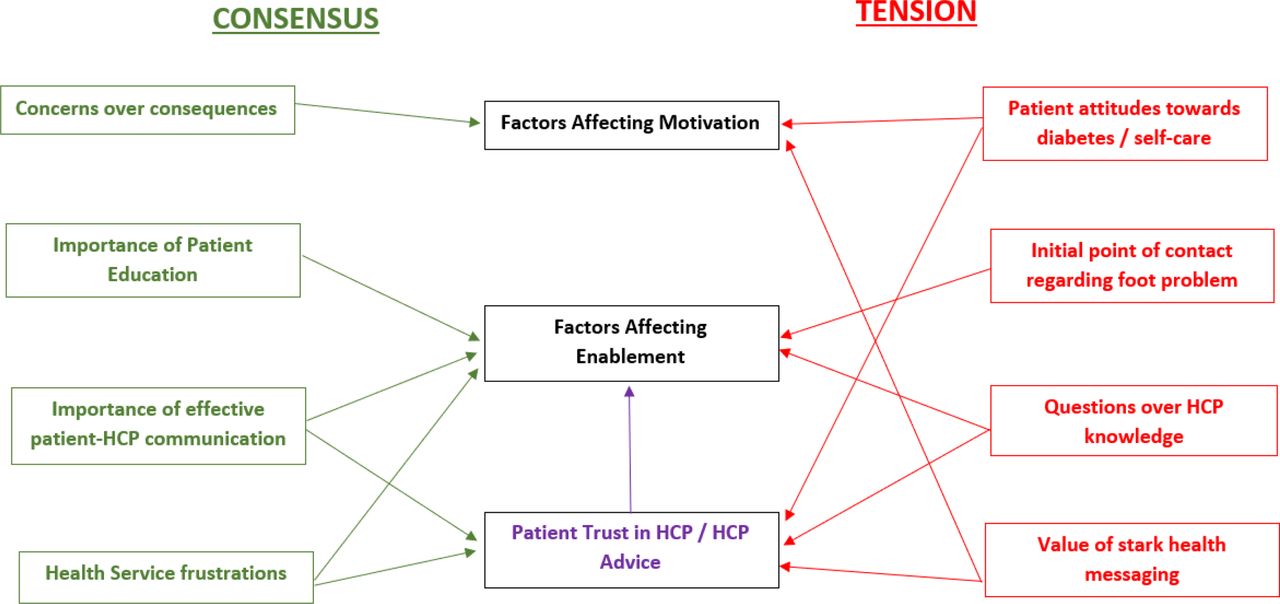 Figure 1
Figure 1 Areas of patient and HCP consensus/tension of perspective and its relationship with barriers and facilitators to good foot self-care behaviors. HCP, healthcare professional.
Alignment in perspectives between patients and HCPs may increase the productivity of the interactions between them in consultations, which may lead to increased quality of care and patient outcomes.46 Also, shared perspectives are believed to foster greater understanding and shared goal-setting, which are crucial to the establishment of an effective therapeutic alliance between patients and HCPs.47 Given the areas of consensus highlighted in this study, using shared perspectives to facilitate more effective communication between patients and HCPs could increase quality of patient care and help patients become suitably motivated to undertake and sustain good foot self-care behaviors. For instance, HCP communication could demonstrate an understanding of the concerns that patients may have; provide a means of explaining how their advice may help prevent those concerns from becoming a reality; show empathy and cognisance of the experiences and challenges faced by the patient in incorporating advice into undertaken behaviors, and do so in a way that seeks to avoid making assumptions and judgments about patients.36 43 46 47
‘Tension’ relates to where there were areas of disagreement and ambivalence in perspectives between the groups interviewed (patients and HCPs). The four main areas of tension within and between these participant groups were: patient attitudes and behaviors (ie, a perception of them as lacking motivation); the initial point of contact regarding foot problems; questions over HCP knowledge (ie, disparate perceptions regarding HCP knowledge of foot-specific issues) and thoughts around stark health messaging. Divergent beliefs between patients and HCPs can affect care through competing therapies; fear of the healthcare system and/or distrust of the medical professionals and/or their prescribed therapies.48 The suggestion is that differences in beliefs may negatively affect treatment decisions and, ultimately, patient outcomes. Of particular interest was the area of tension around differences in perspective over who the initial point of contact should be for an emergent foot problem. The HCPs interviewed all expressed that this should be a podiatrist while the patients more commonly indicated that they would take emergent foot problems to their GP initially. When set against other key areas of tension—confusion over division of foot health responsibility and questions over the HCP knowledge on foot health in diabetes—this may help to identify why some patients may not be getting timely specialist advice and attention for developing foot health problems in diabetes. How these areas of tension may ultimately impact on the provision of care is that differences in beliefs between patients and HCPs have been widely cited to negatively affect treatment decisions and, ultimately, patient outcomes.32 43 46–49 In consideration of the practical implications of these findings, the following suggestions relate to practice improvements and areas where further research may be needed: (1) HCPs should recognize that individuals differ in how they respond to different rationales. Some respond more favorably to gain-framed messaging, whereas others may respond more favorably to loss-framed messaging.50 Recognizing this dynamic should encourage HCPs to develop more flexibility in their approaches to their communication with patients; (2) there should be renewed focus on developing consistency of messaging by HCPs. This is both in terms of who the most appropriate HCP is to present developing foot problems to initially, as well as clarifying the roles and responsibilities of HCPs and patients around foot care; (3) the benefit of foot-specific training being provided to non-foot specialist HCPs should be explored. This would be with a view to help build knowledge and confidence in this area for non-foot specialist HCPs so that patients may more routinely be steered toward the topic of foot health conversations. Furthermore, this may help build patient trust and confidence in these HCPs that they are providing accurate information to patients.32
LimitationsThis study was conducted in an affluent part of the south of England and may not reflect the views and experiences of all patients in differing areas of the country, across varying socioeconomic contexts. The healthcare experiences of individuals are known to vary quite substantially between NHS trusts and regions and so this may not reflect the national picture. The small sample size of each group of participants cannot reflect the whole population or be generalizable in a quantitative sense, nor was it intended to. In particular, the patient participants represented a largely homogenous ethnic make-up (white British), meaning that experiences of different ethnic minorities may be quite different to the experiences identified here. In terms of the HCPs, while there was a useful sample of different HCP disciplines represented in this study, it would have been preferable to have had slightly wider engagement from other HCPs also involved in the delivery of care to people with diabetes. Finally, as the researcher is a podiatrist and this was known to all participants in this study, it should be recognized that this may have had a degree of influence on some of the participants’ responses as well as the analysis of the findings. However, engagement with reflexive research practice, reflection, respondent validation and the aid of the study supervisors in cross-checking the codes and themes as they were created (as detailed in the ‘Research design and methods’ section) have helped to reduce potential biases of the researcher.
ConclusionThis study sought to explore patient and HCP perspectives on the barriers and facilitators to foot self-care behaviors in diabetes, and explore whether any areas of consensus and/or tension in these perspectives contribute to these perceived barriers and facilitators. In so doing, this study has identified points of misalignment between the views of patients and practitioners that may help to explain why adherence to foot self-care among patients with diabetes is low. Our results suggest that better outcomes may stem from HCPs focusing on supporting autonomous motivation for self-care and enhancing the rationale through referencing patients’ own experience rather than focussing on increasing patient knowledge. Renewed focus on consistency of messaging by HCPs around the roles and responsibilities relating to foot health in diabetes, and the benefit of foot-specific training being provided to non-foot specialist HCPs may also help to improve uptake and adherence to foot self-care behaviors in diabetes.
Data availability statementNo data are available.
Ethics statementsPatient consent for publicationEthics approvalThis study was approved by The University of Bath and through Health Research Authority (IRAS ID: 266394). Participants gave informed consent to participate in the study before taking part.
留言 (0)