
記住我

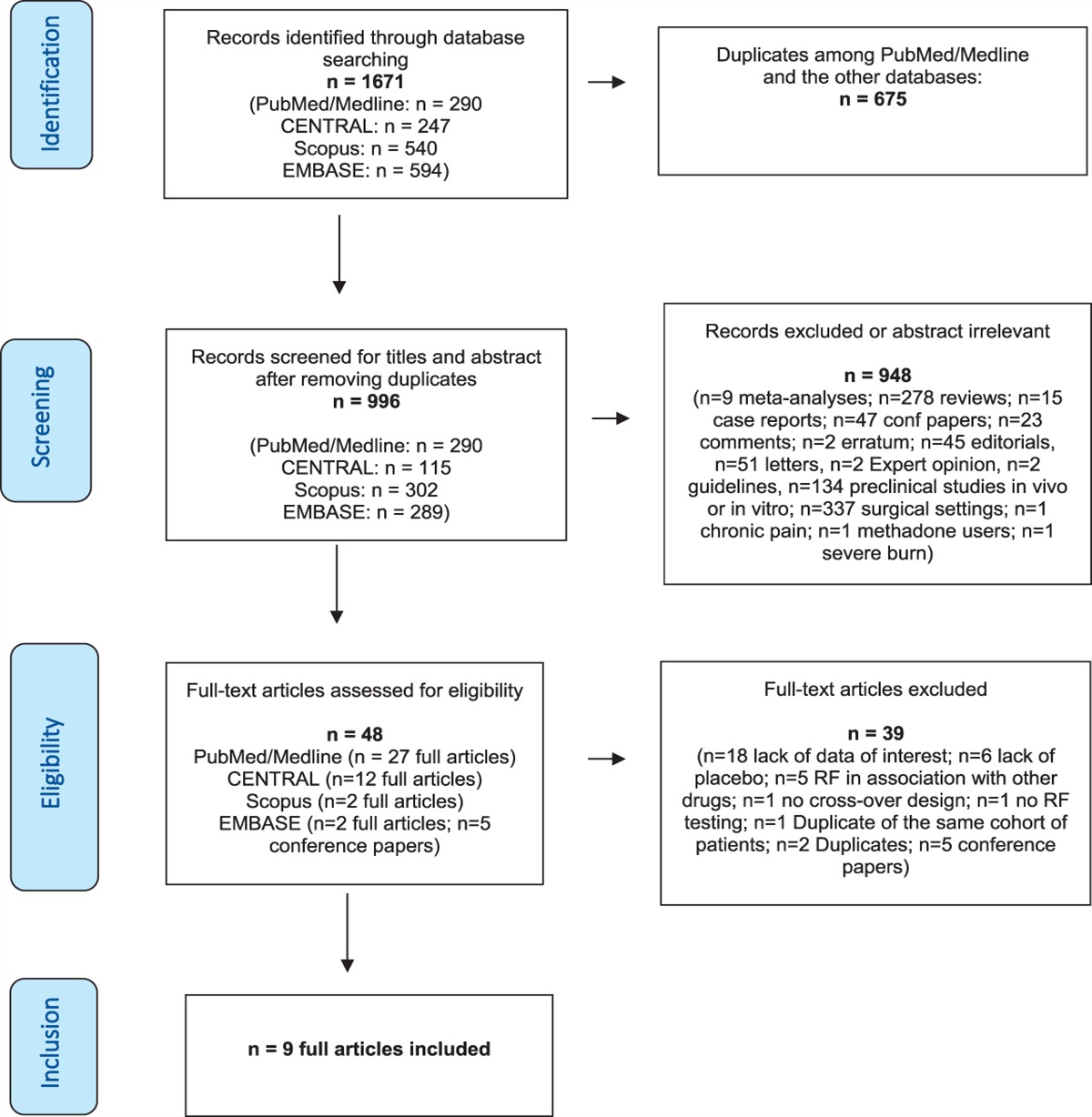

Chronic postsurgical pain (CPSP) is a surgical complication characterized by pain that persists beyond normal healing time.57 Chronic postsurgical pain occurs in 10% to 70% of patients depending on the surgical procedure18,20,25 and is responsible for approximately 25% of referrals to chronic pain clinics.13 The need to prevent and effectively manage CPSP is critical, given its alarming prevalence worldwide and its incidence, which adds millions of new cases to the roster each year.25,38,65 Identifying causal, modifiable risk and protective factors for CPSP can facilitate this goal and advance our overall understanding of the transition from acute to chronic pain.25,51
In addition to its debilitating physical sequelae, chronic pain is associated with alterations in memory, especially that of pain.27,44,45 One area that warrants attention for its potential role in initiating and maintaining chronic pain is autobiographical memory. Autobiographical memory refers to a system of memories for one's personal past consisting of episodic and semantic components. The coherent and flexible construction of these memories is integral to one's sense of self-continuity23,65 and well-being,12,17 facilitating everyday behaviours such as planning and imagining the future,1,2 problem-solving,59,64 and emotional regulation.53 A phenomenon known as overgeneral memory describes a tendency to recollect personal memories that lack specificity.73 It has been proposed that psychological processes of rumination and avoidance, also common in chronic pain, interfere with the search for event-specific knowledge and cause retrieval to fixate at the overgeneral level.75 Although an overgeneral bias is well established in mood disorders,47,76 relatively little is known about autobiographical memory in chronic pain.
Cross-sectional research on the topic yields mixed findings. Some studies have found greater overgenerality30,52,71 and differences in retrieval latency among individuals with chronic pain compared with pain-free controls.30,77 Quenstedt et al.52 extended these findings by showing that individuals with a history of chronic pain have similar patterns of reduced specificity as well as more pain-related content in their recollections and imagined future episodes. These observations align with findings that individuals with chronic pain tend to retrieve memories with congruent emotionality and content.39,77 By contrast, another cross-sectional study failed to find associations between memory specificity and chronic pain but did report state-dependent differences in memory valence.60 However, because not one prospective study has evaluated memory specificity and its association with pain, the temporal relationship between the 2 remains unknown, and hypotheses about determinant factors cannot be ruled out. Moreover, to our knowledge, memory specificity and its relation to pain have not been examined in individuals undergoing major surgery.
This study sought to address these gaps. We assessed autobiographical memory before and after major surgery using a prospective longitudinal design. Presurgical memory specificity, content, and latency were analyzed in relation to pain across multiple postsurgical time points that spanned one year. We hypothesized that an overgeneral memory style, a bias toward surgery-related content, and more negatively valenced memories would individually predict the development of CPSP. We did not have specific predictions about retrieval latency.
2. Methods 2.1. ParticipantsOne hundred nine patients scheduled to undergo major surgery at the Toronto General Hospital were approached for the study. Inclusion criteria were patients scheduled for major surgery; to receive intravenous or epidural opioids postoperatively for a minimum of 48 hours; age between 18 and 60 years; and fluency in English. Patients who were scheduled for other regional anaesthetic techniques during or after surgery were not eligible for participation in the study.
2.2. ProcedureThe study was reviewed and approved by the Research Ethics Boards at Toronto General Hospital (06-0641-AE) and York University (2006-240). Patients were recruited for the study during their preadmission appointment an average of 8.85 ± 6.11 days before surgery. After obtaining informed consent, a set of presurgical questionnaires assessing demographic, health, pain, and psychosocial information were administered. Patients were followed-up on these measures and other pain-related questions in person one month after surgery, whereas 3-, 6-, and 12-month follow-ups were completed by telephone. Questionnaires administered as part of a separate research question concerning psychosocial predictors of CPSP included the PTSD Checklist Civilian Version,72 Pain Catastrophizing Scale,62 Fear of Pain Questionnaire-III,37 and Pain Anxiety Symptoms Scale (PASS-20).36 Seeing as we did not have a priori hypotheses about these measures, they were not analyzed for the current sample and only questionnaires pertinent to the study were included in the final analyses and discussed below. The Autobiographical Memory Test was administered to participants in person by a research nurse during the preadmission appointment as well as one month after surgery (40.45 ± 17.52 days). At each follow-up assessment, we attempted to contact participants by telephone a maximum of 3 times and a voice message was left on the third call. Those who could not be reached were deemed lost to follow-up.
2.3. Measures 2.3.1. PainPain in the current study was defined dichotomously, by its presence or absence. Classification of patients into pain or nonpain groups was based on questions from the Current Pain and Pain History Questionnaire49 administered at baseline and pain-related questions from surveys conducted at each postsurgical follow-up interview. At baseline, participants specifically responded to the question, “Do you have any ongoing pain problems?”. Those who responded “yes” were categorized as having baseline pain before surgery. For each postsurgical interview, participants responded to questions about their postsurgical pain, including “Are you in pain right now?” and “Are you ever in pain?”. If they answered “yes” to either question, they were categorized as having pain at that particular time point. Of the 100 pain values that were missing across the 4 postsurgical time points, 39 of these were inferred based on patients' responses to the same question at subsequent time points (eg, if time point 2 was missing but the responses at time point 3 and 4 were “yes”, time point 2 was recorded as “yes”) and/or based on their responses about the length of time it took for pain to disappear after surgery.
Seeing as most studies to date have linked memory biases to the experience of pain, pain presence was chosen over other clinically relevant measures such as pain disability. The focus on pain might also in part be attributed to the brain regions presumed to be common to memory and pain. The hippocampus, which is known for its key role in processing autobiographical memories, has recently been found to undergo changes that have predictive implications for chronic pain.3,6,42,69 Expansion of the left posterior hippocampus has also been shown to be associated with negative memory biases in patients with chronic pain reflected in a tendency to recall pain as more intense than originally reported.6 Therefore, we expected memory biases in this study to be linked to the experiential components of pain, which seem to relate to the mechanism that links memory and pain.
2.3.2. Hospital anxiety and depression scaleThe Hospital Anxiety and Depression Scale (HADS) is a 14-item self-report measure that screens for anxiety and depression.79 Participants are asked to rate each item on a 4-point scale ranging from 0 to 3 based on how they have been feeling in the past week. Half the items assess for symptoms of depression, namely anhedonia, slowing down, and appearance, whereas the other half screen for anxiety reflected through feelings of tension, restlessness, and autonomic anxiousness. Responses for each subscale item are summed to yield separate anxiety (HADS-A) and depression (HADS-D) scores. The current study also used the HADS total score, which has been found to be a good estimate of a strong general factor representing general psychological distress46 validated in patients with chronic pain.19,31 Higher scores indicate greater severity of emotional distress. The HADS total score and subscales have been shown to have good psychometric properties in patients with acute and chronic pain, including high internal reliability (HADS-A: mean α = 0.83; HADS-D: α = 0.82) and good construct validity.7,31,67 The HADS also had similar good internal reliability in our sample (HADS-A: α = 0.86; HADS-D: α = 0.81; HADS-Total: α = 0.89).
2.3.3. Autobiographical Memory TestThe Autobiographical Memory Test (AMT)73 is the most commonly used measure of overgeneral memory. Few studies report the internal consistency of the AMT, possibly because of the underestimation of reliability for binary data when examined using traditional statistical measures such as Cronbach alpha.22,56 Reported values typically range from α = 0.54 to 0.77,22,63 with higher reliability coefficients associated with alternative statistical methods for dichotomous items.21,22 In this study, participants were instructed to describe the first memory that came to mind of a specific event from their past associated with the presented cue word, which was read aloud by the research nurse. They were also asked to indicate the date and time when the event occurred. If the patient failed to generate a response after 15 seconds, they were prompted again for a specific memory. Cumulative response times were recorded by the experimenter. Cues consisted of 5 pain-related words (ie, pain, hurt, sore, aching, and throbbing) and 5 positive words (ie, pleasure, safe, delighted, relieved, and relaxed), which were selected using the American Heritage Word Frequency Book and matched based on their frequency (F) and standard frequency index.10 Word pairings and their frequencies are summarized in the Supplementary Table (available at https://links.lww.com/PAIN/B616). The order of the cues was randomized for each participant, but words were always grouped according to cue type (ie, pain-related or positive). Three neutral cue words (ie, egg, beach, and clock) were administered at the start of the task so that participants could practice generating memories and clarify instructions if necessary. In the present context, memories elicited in response to pain-related cues are referred to as pain memories.
2.3.3.1. Autobiographical memory test scoringSpecificity coding was completed using the standard method in which participants' responses were classified as either specific or nonspecific/overgeneral.73 The specific category was composed of events that occurred within a distinct spatiotemporal context and lasted less than 24 hours (eg, “My hips were aching Sunday from stretching”), whereas nonspecific/overgeneral responses were those that described events extending beyond a single day (eg, “I've been relaxed the last 3 weeks while I was away on a cruise”), categories of repeated events (eg, “Every time I play squash my legs are always sore the next day”), personal semantic information about the self (eg, “My sister Amy has broken her arm before”; “I've always been quite sensitive”), and general semantic knowledge and associates (eg, “Dogs”; “Ottawa is the capital of Canada”). Responses that were incomprehensible, meta-cognitive, hypothetical, future- or present-oriented, repetitions, or nonresponses were coded as errors and omitted from the analyses. Two hundred thirty-five out of a total of 1872 responses (across both time points) were coded as errors and omitted. The number of specific and nonspecific/overgeneral responses were tallied for each cue type and used in the final analyses. A primary rater first coded all baseline memories and then met with a second rater undergoing training to review coding decisions. After the second rater completed training, both raters independently coded all memories from the second time point and achieved 79.3% agreement (κ = 0.586, z = 14.3, P < 0.001). Raters reviewed all scoring decisions together and resolved discrepancies through discussion until a consensus was reached. They were also blind to participant information including patients' pain status.
Emotional valence was coded by assigning qualitative ratings of positive, negative, or neutral emotionality to each memory. Surgery-related content was assessed by dichotomously coding memories for the presence or absence of any mention of surgery. Valence and content ratings for all memory responses were independently coded, and interrater reliability was high (valence: 93.6% average agreement, κ = 0.593, z = 29.6, P < 0.001; surgery content: 96.7% average agreement, κ = 0.867, z = 34.2, P < 0.001). Raters then met to review all coding decisions and resolved discrepancies through discussion until a consensus was reached. Final numbers for each item were totaled and used in the data analyses.
2.4. Statistical analysesAnalyses were conducted using SPSS (version 27) and R Studio (version 4.0.2 for Mac). A type I error rate of 0.05 was used for all tests of significance. Differences between participants with and without pain at baseline on psychological measures at baseline were assessed using two-sample Mann–Whitney–Wilcoxon tests. Relationships between HADS-A, HADS-D, HADS total score, and memory specificity variables for each cue type at baseline were assessed using Spearman rank–order correlations.
Four generalized estimating equations (GEE) with a logit link function were used to model pain as a repeated binary outcome at 1, 3, 6, and 12 months after surgery with presurgical pain status (yes or no), time (1, 3, 6, and 12 months), and memory variables from the AMT as predictors, and baseline general distress (HADS total score), age, and sex as covariates. Memory variables were baseline specificity categories for each cue type (specific-pain cued, specific-positive cued, overgeneral-pain cued, and overgeneral-positive cued) in the first model, baseline average reaction times for each cue type in the second, baseline valence ratings (positive, negative, and neutral) in the third, and total surgery-related memories from baseline and 1 month in the fourth. Results are presented as odd ratios (OR) and the associated 95% confidence intervals (CI). Figures depict estimated marginal means and the associated 95% CIs.
3. Results 3.1. Participant characteristicsOf the 109 patients approached, 2 were excluded because of lack of proficiency in English, one refused participation, 2 were not included because of the cancellation of the surgery, 2 withdrew the consent after surgery, and 5 additional patients were not included in the analysis as they did not return the preadmission questionnaires. The final sample therefore included 97 participants (one with information missing for sex). Out of 96 participants with available demographic information, 37 were female and 59 were male. The mean ± SD age of participants was 55.2 ± 10.8 years with a range between 19 and 73 years. The average body mass index (BMI) was 28.52 ± 5.23 kg/m2 (n = 95). The majority of participants identified as White (86 out of 94) and almost half had an undergraduate or college degree (44 out of 96). Additional participant demographic characteristics are reported in Table 1. Information regarding the types of surgical procedures patients underwent was collected for 87 individuals and is reported in Table 2. Eighty-two patients out of 95 had a prior history of surgery. Thirty-seven out of 94 patients reported ongoing presurgical pain and 27 out of 95 previously had pain that persisted for more than a month. Finally, 29 out of 96 individuals were currently taking pain medications. Participant pain characteristics are summarized in Table 2.
Table 1 - Participant demographic characteristics assessed before surgery. Demographic characteristics Completers n Sex, n (%) 96 Female 37 (38.54%) Male 59 (61.46%) Age, M ± SD 55.20 ± 10.79 95 BMI, M ± SD 28.52 ± 5.23 95 BMI, n (%) Underweight 18.5 kg/m2 0 (0%) Normal 18.5-24.9 kg/m2 25 (26.32%) Overweight 25-29.9 kg/m2 39 (41.05%) Obese 30 kg/m2 31 (32.63%) Ethnicity, n (%) 94 African-Canadian 5 (5.32%) South Asian 1 (1.06%) Middle Eastern or North African 1 (1.06%) White 86 (91.49%) Hispanic/Latino 1 (1.06%) Highest level of education completed, n (%) 96 Elementary 10 (10.42%) High school 22 (22.92%) Undergraduate university or college degree 44 (45.83%) Graduate university degree 20 (20.83%)Thirty-nine instances of missing pain status values (10.1% of the total dataset) across the 4 postsurgical time points were imputed using the method described above. Missing memory data and pain values that could not be replaced were omitted from the final analyses, leaving 88 cases for the GEE analyses. Comparisons between individuals with and without pain at each time point revealed that patients with ongoing pain had significantly higher baseline scores on anxiety (pain: 8.22 ± 4.56; no pain: 6.54 ± 3.72), depression (pain: 4.81 ± 3.46; no pain: 2.72 ± 2.83), and general psychological distress (pain: 13.03 ± 7.47; no pain: 9.26 ± 6.01), all P < 0.05. There were no significant associations between the psychological measures and memory specificity variables, all P > 0.05 (Table 3).
Table 3 - Means, SDs, and Spearman rank–order correlations between HADS (anxiety, depression, and total scores) and memory specificity variables at baseline (T0). Variable M SD 1 2 3 4 5 6 1. T0 pain-specific 1.53 1.31 2. T0 pain-nonspecific 2.64 1.28 −0.71*** 3. T0 positive-specific 1.94 1.38 0.42*** −0.25* 4. T0 positive-nonspecific 2.53 1.36 −0.29** 0.28** −0.84** 5. T0 HADS-A 7.16 4.13 0.02 0.10 0.03 0.00 6. T0 HADS-D 3.54 3.22 −0.08 0.15 0.01 0.06 0.65*** 7. T0 HADS total 10.69 6.82 −0.02 0.13 0.03 0.01 0.92*** 0.88***M and SD are used to represent mean and standard deviation, respectively. *P < 0.05. **P < 0.01. ***P < 0.001.
Across all postsurgical time points, the number of specific pain memories (memories generated in response to pain-related cues) recalled at baseline was associated with lower odds of having pain at follow-up (χ2wald = 5.67, OR = 0.58, P = 0.017, 95% CI [0.37-0.91]) (Fig. 1). The confidence interval is relatively narrow, indicating a more precise estimate. The main effects of time and presurgical pain were significant, indicating that the percentage of individuals with pain decreased over time (1 month: χ2wald = 42.098, OR = 15.64, P < 0.001, 95% CI [6.81-35.89]; 3 months: χ2wald = 13.01, OR =3.95, P < 0.001, 95% CI [1.87-8.34]; 6 months: χ2wald = 4.33, OR = 2.00, P = 0.037, 95% CI [1.04-3.85]) and that presurgical pain was positively associated with postsurgical pain at all time points (χ2wald =6.85, OR = 2.86, P = 0.009, 95% CI [1.30-6.27]), respectively. The confidence interval for the main effect of time at 1 month was quite wide, whereas the other intervals are relatively narrow, indicating a more precise estimate. Two-way and 3-way interactions among memory variables, time, and presurgical pain were not significant.
 Figure 1.:
Figure 1.: Incidence of pain at postsurgical follow-ups based on the number of baseline-specific memories generated in response to pain-related cue words. Note. The plot depicts estimated marginal means. Error bands represent 95% confidence intervals.
3.2.2. Memory reaction timesReaction times were ln-transformed to adjust for violations of normality gauged from histogram plots and significant Shapiro–Wilk tests (P < 0.05). Longer reaction times for pain-related cues were associated with greater odds of developing postsurgical chronic pain (χ2wald = 7.40, OR = 2.65, P = 0.007, 95% CI [1.31-5.37]) (Fig. 2). The confidence interval is relatively narrow, indicating higher precision. There were also main effects in which the percentage of individuals with pain decreased over time and baseline pain was positively associated with postsurgical pain across all time points, both P < 0.05.
 Figure 2.:
Figure 2.: Incidence of pain at postsurgical follow-ups based on the average reaction times in response to pain-related cue words at baseline. Note. The plot depicts estimated marginal means. Error bands represent 95% confidence intervals.
3.2.3. Memory valenceBaseline valence ratings were not predictive of pain at any of the postsurgical time points. Main effects of time and baseline pain, however, remained significant, both P < 0.05.
3.2.4. Surgery-related memory contentBecause of a large percentage of missing HADS data at 1 month (41.5%), the measure was not included as a covariate in this model. More surgery-related memory content generated at the 1-month assessment predicted higher odds of pain across all postsurgical time points (χ2wald = 4.38, OR = 1.31, P = 0.036, 95% CI [1.02-1.68]) (Fig. 3). Precision of this estimate is relatively high, given the narrow confidence interval. There was no main effect of surgery content from presurgical memories. Main effects of time and baseline pain remained significant.
 Figure 3.:
Figure 3.: Incidence of pain at postsurgical follow-ups based on the number of surgery-related memories generated 1 month after surgery. Note. The plot depicts estimated marginal means. Error bands represent 95% confidence intervals.
4. DiscussionResearch shows that individuals with chronic pain tend to exhibit an overgeneral memory bias (OGM) characterized by personal recollections that lack specificity. However, because of the cross-sectional nature of prior work, the temporal relationship between chronic pain and OGM has, heretofore, been unknown. This study examined autobiographical memory (AM) as a risk/protective factor for CPSP. As hypothesized, the results show that fewer specific pain-related AMs recalled before major surgery significantly predicted pain status 1, 3, 6, and 12 months later. These results build on previous research by demonstrating that the degree of specificity in individuals' recollections, particularly pertaining to pain, predicts CPSP status across the first year after surgery, even after controlling for known confounders including baseline pain status, general psychological distress, age, and sex. In addition, participants who took longer to retrieve pain-related memories before surgery as well as those who recalled more surgery-related content during the acute postsurgical phase were more likely to report pain up to one year later. Contrary to our predictions, we did not find any differences in presurgical memory valence between patients who did and did not develop CPSP. Consistent with the literature, baseline pain also emerged as a risk factor for the development of CPSP.24,25
Notably, the prospective nature of this study indicates that the relative paucity of specific autobiographical pain memories recalled before surgery is a risk factor for the development and maintenance of chronic pain status up to 1 year after major surgery. According to Conway's self-memory system,11 AMs are accessed through an effortful generative retrieval process that progresses in a hierarchical manner beginning with conceptual themes and lifetime periods, followed by general memories of repeated and extended events, and ultimately ending with event-specific knowledge restricted to a particular spatiotemporal context. Processes involving rumination, functional avoidance, and limitations in executive control are posited to contribute to OGM by truncating this search process.75,76 Although this model has predominantly been tested in emotional disorders, similar mechanisms might apply to OGM in patients scheduled for major surgery who develop CPSP.
Indeed, cognitive-affective biases play an important role in chronic pain.40,50 For individuals who are particularly susceptible to psychological and emotional distress, self-relevant cues (eg, pain-related words) might interrupt the search for a specific memory by activating iterative retrievals of conceptual pain memories that coincide with rumination and potentially interfere with inhibitory control. It is possible that this sort of abstract thinking perpetuates a maladaptive self-concept centered around pain that, upon repeated activation, triggers a cascade of psychological consequences and ultimately predisposes individuals to more severe pain outcomes.41,50 Conversely, a tendency to retrieve specific events and their experiential details might allow for greater contextualization of self-relevant pain information and provide evidence that can disprove dysfunctional pain-related beliefs. Confronting one's pain in this way can aid in coping and recuperation.
It is also possible that memory processing in surgical patients might be limited to the OGM level because of their evasion of specific pain memories associated with intense or negative emotions. Pain-related anxiety and traumatic stress responses, including avoidance of pain-related situations, are common antecedents to pain chronicity and disability.4,26 Several studies have found that attentional avoidance of certain pain-related stimuli predicts the development of postoperative and chronic pain.28,58 Importantly, in this study, OGM predicted CPSP even after controlling for the effects of other psychosocial factors. Therefore, these results suggest that the observed reduction in specificity is likely not attributable to underlying psychopathology. Further work is needed to clarify the role of dysfunctional emotional, cognitive, and executive processes, and their contributions to overgeneral pain memories in patients undergoing major surgery. Investigating these biases simultaneously can elucidate whether and how these mechanisms interact to influence memory and subsequent pain outcomes.70
This study also adds to previous research by demonstrating that participants who took longer to access pain memories before surgery were at greater risk of developing CPSP up to one year later. These findings suggest that access to personal pain memories for these individuals was more effortful and less direct, requiring the use of generative memory processes.68 As discussed above in relation to OGM, limited access to these memories might inhibit individuals' ability to properly process past pain experiences and result in unfavorable outcomes. Cross-sectional research by Liu et al.30 similarly found that after controlling for negative affect, chronic pain outpatients showed slower AM retrieval. Other cross-sectional studies have also found shorter retrieval latency for pain-related memories77 where pain as a negative state was interpreted to enable quicker access to memories of similar emotionality or content.5 Considering that participants in this study were tested before the development of CPSP, however, quicker access to pain-congruent information would not necessarily be expected the way it is in individuals who have chronic pain. On the contrary, cognitive slowing might occur because of the fact that more effort is required to complete goal-directed tasks when greater demands are placed on working memory to mitigate distractions caused by preexisting pain and psychological dysfunction, which often precede CPSP.15,35,48 Research is needed to investigate these possibilities.
Regarding memory content, the present results indicate that individuals who remembered more surgery-related memories one month after their operation were more likely to develop CPSP. This aligns with numerous studies in patients with chronic pain and other clinical populations (eg, PTSD and complicated grief) that also show a tendency to recall memories and imagine future episodes containing mood-congruent content.9,32,39 One interpretation of these results can be gleaned from the self-memory system model of AM, which postulates that memories are shaped by an individual's current self-representation and goals.64 As such, memories that are congruent with one's self-image are considered more accessible than those that are not.
Future research should clarify whether AM is a causal factor in the development of CPSP. If it is, the results from this study present important implications for the prevention and treatment of chronic pain.16,51 For example, novel interventions could be developed to modify patients' presurgical memories with a focus on training individuals to selectively retrieve specific pain memories and enhance episodic reexperiencing of past events. Memory specificity training programs are effective not only for improving specificity but psychological well-being as well.33,34,43,55 Moreover, psychotherapies used for presurgical and postsurgical pain management could be enhanced to incorporate memory reframing techniques that restructure negative pain associations. Indeed, considering that patients in this study who were vulnerable to CPSP showed a preoccupation with surgery, setting positive goals and reducing rumination could be conducive to recovery. Nonetheless, the utility of such treatments is contingent on the causal role of AM, which has yet to be determined.
This study has several limitations. First, our sample size precluded exploring interaction effects without overfitting the GEE models. Limited demographic information was collected and the sample was overwhelmingly White, which may reduce generalizability of findings. Future studies with larger and more diverse samples could examine how different types of AM biases might interact to predict CPSP. In addition, although the AMT is a very popular method for assessing OGM, elicited responses tend to be very brief, which can be difficult to reliably interpret and qualify. Moreover, entire memories are dichotomously scored according to temporal specificity. This approach contradicts cognitive models that suggest AMs simultaneously consist of both episodic and semantic details.29,66 Memory assessment tools that allow for elaboration and use a more nuanced scoring method (eg, The Autobiographical Interview29) could provide insight into the types of details represented in the personal memories of surgical and chronic pain patients. Future studies might also consider using different versions of the memory task on each test occasion to control for prior exposure or practice effects. Finally, neurocognitive and psychiatric conditions were not screened for in the current sample. This would have been important for dissociating these factors from memory performance and pain. In the same vein, including objective measures of episodic and semantic memory could provide a control for general dysfunctions of declarative memory.
In summary, the results of this study indicate that differences in AM style are a risk factor for the development of CPSP. Reduced presurgical specificity for pain-related memories and a bias toward surgery-related content during the acute postsurgical phase were predictive of chronic pain after major surgery. Moreover, more effortful retrieval reflected in longer response times for presurgical pain memories also predicted worse postsurgical pain outcomes up to one year later. Future research should investigate the effectiveness of treatment strategies that take advantage of AM as a modifiable risk factor by optimizing patients' access to specific memories of past pain experiences and redirecting focus toward more constructive memory content. Contextualizing memories in this way might facilitate postsurgical recovery and present a promising new path for preventing the transition from acute to chronic pain.
Conflict of interest statementA. Waisman is supported by a Natural Sciences and Engineering Research Council (NSERC)-Alexander Graham Bell CGS-M Award. J. Katz is supported by a Canadian Institutes of Health Research (CIHR) Canada Research Chair in Health Psychology at York University. H. Clarke is supported by a Merit Award from the Department of Anesthesiology & Pain Medicine at the University of Toronto. The remaining authors have no conflicts of interest to declare.
Appendix A. Supplemental digital contentSupplemental digital content associated with this article can be found online at https://links.lww.com/PAIN/B616.
Supplemental video contentA video abstract associated with this article can be found at https://links.lww.com/PAIN/B617.
References [1]. Addis DR, Schacter DL. The Hippocampus and imagining the future: where do we stand? Front Hum Neurosci 2012;5:173. [2]. Addis DR, Wong AT, Schacter DL. Remembering the past and imagining the future: common and distinct neural substrates during event construction and elaboration. Neuropsychologia 2007;45:1363–77.
留言 (0)