Study design and study subjects
The present study is a prospective, single-blind, RCT, performed according to the principles of good clinical practice and the International Declaration of Helsinki. The study was approved by the Ethics Committee of Istanbul University, Istanbul Faculty of Medicine, Istanbul (dossier no: 1281/2016). The study is retrospectively registered on Clinicaltrials.gov (Ref. NCT04202367, first registration date was 17/12/2019.) and reported according to the CONSORT statement.
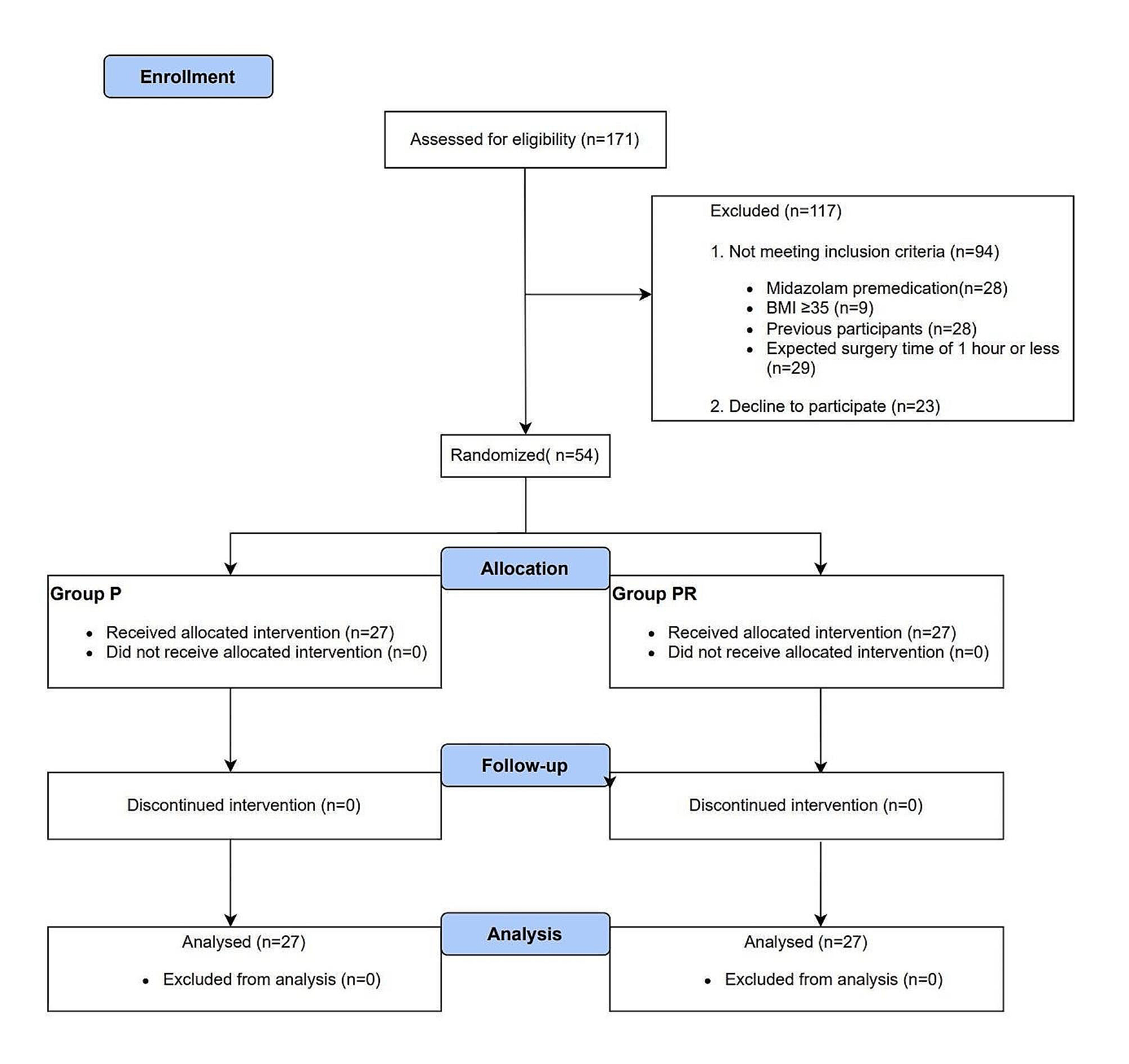
After obtaining written informed parental consent, 74 (37 in group 1 and 37 in group 2) children were allocated to this trial. Children aged between 1 and 8 years in the ASA I and II, undergoing unilateral open inguinal hernia repair were eligible for the study. Children aged less than 1 or more than 8 years; those with a neurological deficit, bleeding diathesis, or a history of allergy to local anesthetics; children whose physical examination revealed an infection in the region to be injected; those who have mental retardation or communication problems; and subjects who did not accept to participate in the study were excluded.
Patient randomization
After inclusion/exclusion criteria were met, randomization was performed using a web-based system that generates numbers for the participants (www.graphpad.com/quickcalcs/randMenu/). Allocation numbers were presented in sealed opaque envelopes, which were prepared by an independent researcher before the start of the study, and these envelopes were opened in the operating room by the anesthetist on the day of surgery. This investigation was planned as single-blinded. Since the LA doses were visibly distinguishable, blindness could not be provided by the operating anesthetist. However, clinical follow-up data were collected by researchers who were blinded to the dosage and volume of the LA.
Anesthesia, intervention, and post-interventional follow-up
Patients were monitored with standard ASA recommendations including pulse oximetry, non-invasive blood pressure, end-tidal CO2, temperature, and electrocardiogram. Patients were premedicated, 30 minutes prior to the surgery, with oral midazolam 0,5 mg.kg− 1 once diluted in apple juice. For the induction of anesthesia, sevoflurane 4–6% was administered via a face mask. Subsequently, intravenous rocuronium (0,3–0,6 mg.kg− 1) was administered and a laryngeal mask was installed, and TAPB was performed prior to incision.
To perform the lateral approach; the iliac crest, 12th rib and midaxillary line were identified as the landmarks, and the in-between area was disinfected using 2% chlorhexidine in 70% alcohol [10]. A high frequency (7–15 MHz) linear ultrasound probe (GE Logiq-e Nextgen model, General Electric medical systems, Phoenix, AZ, USA) was covered with a sterile sheath, and placed on the midaxillary line transversally between arcus costarum and iliac crest. Once the muscular fascia between the internal oblique and the transversus abdominis muscle was identified, a peripheric block needle (22G, 50 mm, Stimuplex®; B. Braun, Melsungen, Germany) was advanced in-plane from anterior to posterior aiming for the interfascial space. Needle tip placement was checked via 0.5 ml saline injection, and if the desired fascial expansion was observed, the prepared LA solution was injected [4, 13].
A US-guided TAPB was provided in equal doses (1 mg.kg− 1) but with different concentrations of bupivacaine on the ipsilateral side of the incision.
Group 1: Patients received 1 mg.kg− 1bupivacaine 0.25%, 0.4 ml.kg− 1.
Group 2: Patients received 1 mg.kg− 1bupivacaine 0.125%, 0.8 ml.kg− 1.
Anesthesia was maintained with sevoflurane 2% in oxygen (FiO2 = 0.35) using a closed-circuit respirator and intravenous 0.1 μg.kg− 1.min− 1 remifentanil infusion. All subjects received paracetamol 15 mg.kg− 1 intraoperatively. Dexamethasone 0,15 mg/kg and ondansetron 0,1 mg/kg were given as a bolus for the prophylaxis of postoperative nausea and vomiting (PONV).
Postoperative pain was assessed by FLACC (Face, Legs, Activity, Cry, Consolability) behavioral pain assessment score at 15-, 30-, 45- minutes, and 1-, 2-, 6-, and 24-hour. Tramadol 1 mg.kg− 1 was administered intravenously as a rescue analgesic if the pain score was equal to or more than 4 at the post-operative care unit. The total analgesic requirement was recorded. All children were prescribed oral paracetamol 15 mg.kg− 1 four times per day for postoperative pain. All children were discharged on the same day after being comfortable, mobile, and tolerating oral fluids.
Primary outcome
The primary outcome was the efficacy which is assessed by postoperative FLACC behavioral pain assessment score up to the first 24 hours. FLACC evaluation was taught to the caring legal guardians by the ward nurse in the preoperative period when the children were admitted to the ward. Acute postoperative period FLACC scores were recorded by the anesthesiology research team. Detailed information was obtained by calling the parents of the children who were discharged earlier than 24 hours.
Secondary outcomes
The secondary outcomes included the percentage of patients receiving rescue analgesics on the first postoperative day, the cumulative dose of rescue analgesic consumption, length of hospital stay, the incidence of side effects including nausea, vomiting, hypotension, motor weakness, and urinary retention, complications (e.g., visceral puncture, vascular injury) and satisfaction of the patients’ parents and the surgeons. The satisfaction was questioned as “pleased” or “not pleased”.
Statistical analysis
Sample size calculation was performed using G* Power version 3.1.9.2 (Kiel University, Kiel, Germany) software. According to our 10-patient pilot study, FLACC scores data at postoperative 6th hour (0.7 ± 0.2 for Group 1 and 0.5 ± 0.3 for Group 2), 27 patients per group were needed with a power of 0.8 while alpha was 0.05. Considering a 20% drop-out, a total number of 66 patients were planned to enroll in the study. The Shapiro-Wilk test method was used to test the normality of the continuous data. Baseline characteristics are presented as mean ± standard deviation or median (minimum-maximum) for quantitative variables, and as number (percentage) for qualitative variables. Categorical data were compared using a χ2 test with Fisher’s exact test, depending on sample sizes. For continuous outcomes, we compared groups using the Student’s t-test or Mann–Whitney U-test, depending on the data distribution. Data analysis was performed using SPSS 22 software (IBM Corp., Armonk, NY, USA). A p-value ≤0.05 was considered significant in outcome analysis.







留言 (0)