
記住我
Editor,
Cardiac tachyarrhythmias have been treated by catheter ablation for nearly half a century.
Due to the duration and discomfort of the procedure, ablations are usually carried out either under general anaesthesia or conscious sedation. Although patient comfort is the most important immediate priority, the choice of general anaesthesia over sedation is often influenced by the type of ablation being performed.
Herein, we seek to provide a succinct overview of the practical considerations of different anaesthetic strategies for the various types of ablation procedure.
Atrial fibrillationAtrial fibrillation, caused by chaotic electrical activity in the atria (Fig. 1), is the most common arrhythmia with a UK prevalence of 3.29%.1 Pulmonary vein isolation (PVI) using radiofrequency or cryoballoon ablation is a well established treatment for atrial fibrillation. Three-dimensional electro-anatomical mapping is often used for radiofrequency ablation, with which a left atrial ‘geometry’ is created by the movement of a mapping catheter within the chamber onto which electrical data can be superimposed to diagnose arrhythmia mechanisms and localise arrhythmogenic foci (Fig. 2). Movement during acquisition of the geometry can lead to dislocation of catheter projection relative to the anatomical map, resulting in ablation at incorrect sites, and a higher likelihood of mechanical complications due to catheter trauma.
 Fig. 1:
Fig. 1: Diagrammatic representation of chaotic disordered atrial electrical activity as the mechanism for atrial fibrillation.
 Fig. 2:
Fig. 2: Electro-anatomical maps of the left atrium created using Carto (above) and Rhythmia (below).
A popular method of delivering general anaesthesia is total intravenous anaesthesia (TIVA) using infusions of remifentanil, an ultra-short acting opioid, and propofol alongside depth of anaesthesia monitoring. Conscious sedation using opioid or benzodiazepine boluses may be used in cases where general anaesthesia is not desired.2 Use of general anaesthesia results in better contact force and a more contiguous lesion set when compared with conscious sedation for radiofrequency PVI,3 as patient immobility and controlled respiratory excursion allow better catheter stability and tissue contact.4 This translates into lower longer-term arrhythmia recurrence.3–7 Outcomes may be further improved using high-frequency jet ventilation to minimise thoracic respiratory excursion,8,9 though this is potentially offset by the added complexities associated with the technique, which limit its appeal at present. The additional time taken to anaesthetise patients appears to be compensated by shorter ablation time, resulting in a similar overall duration of the procedure between general anaesthesia and sedation.4,7
Left atrial geometry is not required for cryoballoon ablation, and accordingly, general anaesthesia use does not appear to confer any outcome advantage.10 In contrast to radiofrequency procedures, however, overall laboratory times are longer when general anaesthesia is used.
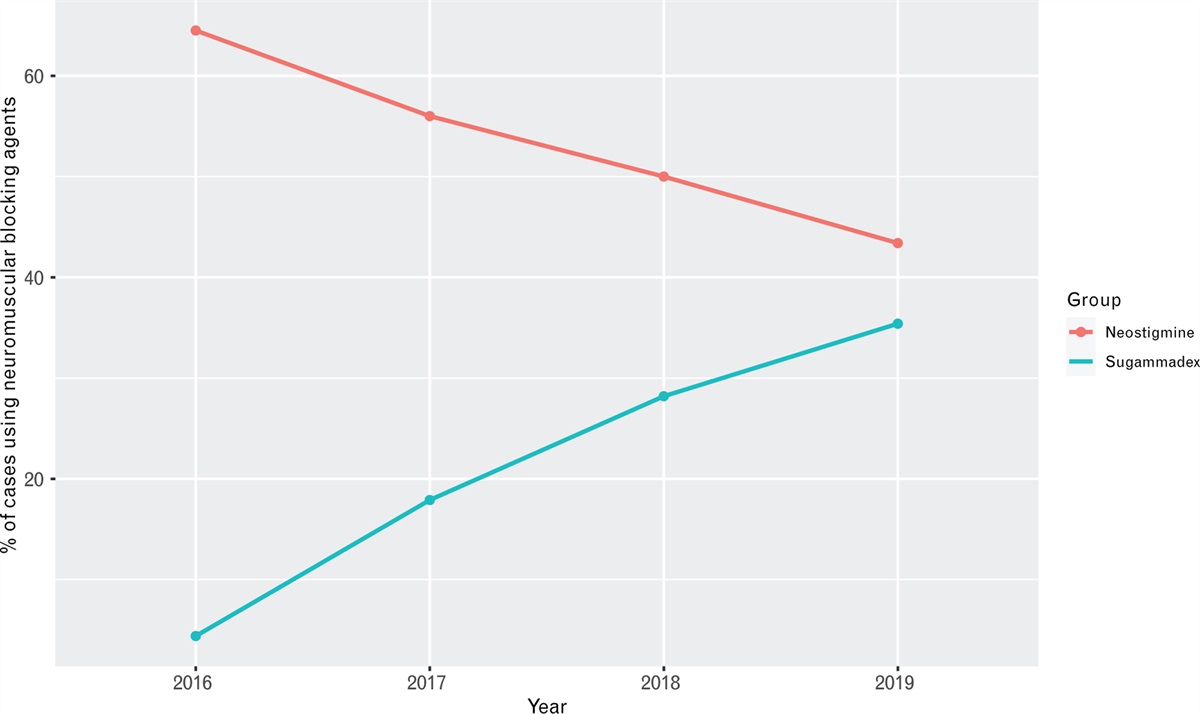
Heterogeneous strategies across studies make direct safety comparison between general anaesthesia and sedation difficult, though complication rates are low overall. Hypotension is frequently observed with general anaesthesia or deep sedation use, particularly in older patients. This is generally mild and reversible with no reports of procedure abandonment or longer-term sequelae.4,11–13 Postprocedure complications arising from general anaesthesia/deep sedation are significantly more frequent in patients at least 75 years of age.11 Thus, once out of the laboratory, an appropriate period of observation is necessary to assess for anaesthesia-related complications.14 TIVA decreases the incidence of postprocedure nausea and delirium compared with volatile anaesthetics15 and reduces the requirement for neuromuscular blockers, thereby avoiding the adverse effects associated with this.16
There is no significant difference in the rate of major complications, such as atrio-oesophageal fistula, cardiac tamponade or death, between atrial fibrillation ablation under general anaesthesia or conscious sedation. Higher rates of thermal oesophageal injury have been reported in general anaesthesia cases,17 but all lesions are normalised by 2 months.
Supraventricular tachycardiaSupraventricular tachycardia (SVT) is a term that covers atrioventricular nodal re-entrant tachycardia (AVNRT), atrioventricular re-entrant tachycardia (AVRT) and atrial tachycardia (Fig. 3). Arrhythmia induction is required during ablation to clarify the diagnosis and map the substrate. This requirement and the relatively short ablation time therefore support the use of light sedation over general anaesthesia in SVT ablation in adults.
 Fig. 3:
Fig. 3: Schematic diagram representing mechanisms of supraventricular tachycardia.
General anaesthesia can suppress arrhythmia induction through dampening of afferent sympathetic inputs on the cardiac conduction system. Furthermore, isolated case reports describe termination of SVT following propofol administration,18 which may be due to its inhibitory effect on cardiac ion channels.19,20 In addition, dexmedetomidine may depress sinus and atrioventricular node function due to sympatholytic properties.21 However, neither propofol nor dexmedetomidine use appears to affect baseline electrophysiological parameters or arrhythmia inducibility,22,23 although sympathomimetic agents such as isoprenaline or ketamine coadministration are more frequently required for tachyarrhythmia induction.24,25
Typical atrial flutter ablation does not require arrhythmia induction, as there is a clearly defined critical anatomical target for ablation, the cavotricuspid isthmus (Fig. 4). Typical flutter ablation is a shorter and generally less uncomfortable procedure than radiofrequency atrial fibrillation ablation, and conscious sedation is usually adequate.26
 Fig. 4:
Fig. 4: Diagrammatic representation of a macro re-entrant, anticlockwise circuit around the right atrium, characteristic of typical atrial flutter, with a critical isthmus for ablation: the cavotricuspid isthmus (zigzagged line).
Ventricular tachycardiaFocal ventricular tachycardia can occur due to abnormal automaticity or triggered activity most frequently in the right or left ventricular outflow tract. Ablation for outflow tract ventricular tachycardia relies on triangulating the source of premature ventricular contractions (PVCs) to a specific area of myocardium. The higher the PVC frequency, the higher is the likelihood of accurate localisation and procedural success. Comparison studies between sedation strategies for outflow tract ventricular tachycardia ablation are lacking. Accepted practice is to provide light sedation, if needed, to avoid PVC suppression.
Re-entrant ventricular tachycardias result from a circuit created by the adjacency of rapidly conducting healthy myocardium to an area of slowly conducting scar. Patients often have structurally abnormal hearts with poor contractile reserve. Ventricular tachycardia induction is dependent on the contribution of modulating factors such as autonomic tone and focal triggers. International guidelines caution against the use of general anaesthesia for ventricular tachycardia ablation where possible,27 largely due to the suppression of sympathetic tone and the direct molecular influence of some anaesthetic agents on myocardial conductivity.27,28 Nevertheless, ventricular tachycardia ablation can be a long procedure and general anaesthesia may be warranted for patient comfort and stillness.
The combination of ventricular tachycardia provocation and the hypotensive effects of general anaesthesia renders haemodynamic management challenging, with greater reliance on intravenous inotropic support compared to sedation.29 Invasive blood pressure monitoring may aid early identification and treatment of haemodynamic instability, and reliable vascular access is obligatory. A peripheral intravenous cannula will often suffice, but it is important to have resources available to secure central venous access without delay should the need arise.
ConclusionCardiac electrophysiology procedures are wide-ranging. Generally, minimal sedation is more desirable for re-entrant and automatic arrhythmias, as this increases the chances of successful arrhythmia induction whilst minimising intra-procedural haemodynamic disturbance. For radiofrequency atrial fibrillation ablation, wherein arrhythmia induction is not required, there is evidence suggesting that general anaesthesia use confers better long-term outcomes.
Acknowledgements relating to this articleAssistance with article: none.
Financial support and sponsorship: none.
Conflicts of interest: none.
This manuscript was handled by Mona Momeni.
References 1. Adderley NJ, Ryan R, Nirantharakumar K, et al. Prevalence and treatment of atrial fibrillation in UK general practice from 2000 to 2016. Heart 2019; 105:2733. 2. Neal S Gerstein, Andrew Young, Peter M Schulman, et al. Sedation in the electrophysiology laboratory: a multidisciplinary review. J Am Heart Assoc 2016; 5:e003629. 3. Chikata A, Kato T, Yaegashi T, et al. General anesthesia improves contact force and reduces gap formation in pulmonary vein isolation: a comparison with conscious sedation. Heart Vessels 2017; 32:997. 4. Choi Y, Kim SH, Kim JY, et al. Randomized comparison between dexmedetomidine–remifentanil and midazolam–fentanyl for deep sedation during catheter ablation of atrial fibrillation. Int J Arrhythm 2019; 20:1. 5. Di Biase L, Conti S, Mohanty P, et al. General anesthesia reduces the prevalence of pulmonary vein reconnection during repeat ablation when compared with conscious sedation: results from a randomized study. Heart Rhythm 2011; 8:368372. 6. Martin CA, Curtain JP, Gajendragadkar PR, et al. Improved outcome and cost effectiveness in ablation of persistent atrial fibrillation under general anaesthetic. EP Europace 2018; 20:935942. 7. Pang N, Gao J, Zhang N, et al. Comparison of the different anesthesia strategies for atrial fibrillation catheter ablation: a systematic review and meta-analysis. Cardiol Res Pract 2022; 2022:1124372. 8. Sivasambu B, Hakim JB, Barodka V, et al. Initiation of a high-frequency jet ventilation strategy for catheter ablation for atrial fibrillation. JACC Clin Electrophysiol 2018; 4:15191525. 9. Hutchinson MD, Garcia FC, Mandel JE, et al. Efforts to enhance catheter stability improve atrial fibrillation ablation outcome. Heart Rhythm 2013; 10:347353. 10. Wasserlauf J, Knight BP, Li Z, et al. Moderate sedation reduces lab time compared to general anesthesia during cryoballoon ablation for AF without compromising safety or long-term efficacy. Pacing Clin Electrophysiol 2016; 39:13591365. 11. Wutzler A, Loehr L, Huemer M, et al. Deep sedation during catheter ablation for atrial fibrillation in elderly patients. J Interv Card Electrophysiol 2013; 38:115121. 12. Kottkamp H, Hindricks G, Eitel C, et al. Deep sedation for catheter ablation of atrial fibrillation: a prospective study in 650 consecutive patients. J Cardiovasc Electrophysiol 2011; 22:13391343. 13. Salukhe TV, Willems S, Drewitz I, et al. Propofol sedation administered by cardiologists without assisted ventilation for long cardiac interventions: an assessment of 1000 consecutive patients undergoing atrial fibrillation ablation. Europace 2012; 14:325330. 14. Reddy SA, Nethercott SL, Chattopadhyay R, et al. Safety, feasibility and economic impact of same-day discharge following atrial fibrillation ablation. Heart Lung Circ 2020; 29:17661772. 15. Schraag S, Pradelli L, Alsaleh AJO, et al. Propofol vs. inhalational agents to maintain general anaesthesia in ambulatory and inpatient surgery: a systematic review and meta-analysis. BMC Anesthesiol 2018; 18:162. 16. Hunter JM. Reversal of residual neuromuscular block: complications associated with perioperative management of muscle relaxation. Br J Anaesth 2017; 119:i53i62. 17. Di Biase L, Saenz LC, Burkhardt DJ, et al. Esophageal capsule endoscopy after radiofrequency catheter ablation for atrial fibrillation: documented higher risk of luminal esophageal damage with general anesthesia as compared with conscious sedation. Circ Arrhythm Electrophysiol 2009; 2:108112. 18. Hermann R, Vettermann J. Change of ectopic supraventricular tachycardia to sinus rhythm during administration of propofol. Anesth Analg 1992; 75:10301032. 19. Buljubasic N, Marijik J, Berzci V, et al. Differential effects of etomidate, propofol, and midazolam on calcium and potassium channel currents in canine myocardial cells. Anesthesiology 1996; 85:10921099. 20. Odening KE, Hyder O, Chaves L, et al. Pharmacogenomics of anesthetic drugs in transgenic LQT1 and LQT2 rabbits reveal genotype-specific differential effects on cardiac repolarization. Am J Physiol Heart Circ Physiol 2008; 295:H2264H2272. 21. Hammer GB, Drover DR, Cao H, et al. The effects of dexmedetomidine on cardiac electrophysiology in children. Anesth Analg 2008; 106:7983. 22. Lai LP, Lin JL, Wu MJ. Usefulness of intravenous propofol anesthesia for radiofrequency catheter ablation in patients with tachyarrhythmias: infeasibility for pediatric patients with ectopic atrial tachycardia. Pacing Clin Electrophysiol 1999; 22:13581364. 23. Wutzler A, Huemer M, Boldt L-H, et al. Effects of deep sedation on cardiac electrophysiology in patients undergoing radiofrequency ablation of supraventricular tachycardia: impact of propofol and ketamine. EP Europace 2013; 15:10191024. 24. Hayashi T, Mizukami A, Kuroda S, et al. Outcomes of deep sedation for catheter ablation of paroxysmal supraventricular tachycardia with adaptive servo ventilation,. J Arrhythmia 2020; 37:3342. 25. Char D, Drover DR, Motonaga KS, et al. The effects of ketamine on dexmedetomidine-induced electrophysiologic changes in children. Paediatr Anaesth 2013; 23:898905. 26. Lena P, Mariottini CJ, Balarac N, et al. Remifentanil versus propofol for radio frequency treatment of atrial flutter. Can J Anaesth 2006; 53:357362. 27. Aliot EM, Stevenson WG, Almendral-Garrote JM, et al. European Heart Rhythm Association (EHRA); Registered Branch of the European Society of Cardiology (ESC); Heart Rhythm Society (HRS); American College of Cardiology (ACC); American Heart Association (AHA). EHRA/HRS Expert Consensus on Catheter Ablation of Ventricular Arrhythmias: developed in a partnership with the European Heart Rhythm Association (EHRA), a Registered Branch of the European Society of Cardiology (ESC), and the Heart Rhythm Society (HRS); in collaboration with the American College of Cardiology (ACC) and the American Heart Association (AHA). Heart Rhythm 2009; 6:886933. 28. Nof E, Reichlin T, Enriquez AD, et al. Impact of general anesthesia on initiation and stability of VT during catheter ablation. Heart Rhythm 2015; 12:22132220. 29. Wutzler A, Mueller A, Loehr L, et al. Minimal and deep sedation during ablation of ventricular tachycardia. Int J Cardiol 2014; 172:161.
留言 (0)