To the best of our knowledge, the association between PED, CSC, and VKH has not been reported. For the first time, our study revealed that the occurrence of PED might be associated with CSC development in VKH cases. PED with high choroidal hydrostatic pressure predisposes to the later development of CSC in VKH cases with corticosteroid therapy. Notably, our results indicated that PEDA might be a significant predictive factor for CSC development in VKH cases.
CSC can develop following the administration of corticosteroids via diverse routes [11]. Corticosteroids could elicit or aggravate CSC by inducing choroidal enlargement, which may be caused by the inappropriate mineralcorticoid receptor activation and upregulation of endothelial vasodilatory potassium channel KCa2.3 (calcium-dependent channel) [12]. However, the pilot study demonstrated that steroid-induced CSC might be an idiosyncratic response in selected vulnerable individuals rather than a dose-dependent effect [13]. CSC induced by corticosteroids has been reported to occur in a wide variety of ocular inflammatory conditions but with a relatively low incidence. Majumder et al. revealed that the prevalence of CSC in uveitis was approximately 0.13% in a large retrospective study involving 22,721 patients in India [14]. We found that the specific incidence rate of CSC in VKH was 1.06% in our cohort of 235 patients. This rate is much higher than that revealed in the Indian uveitis population, which included patients with all types of uveitis.
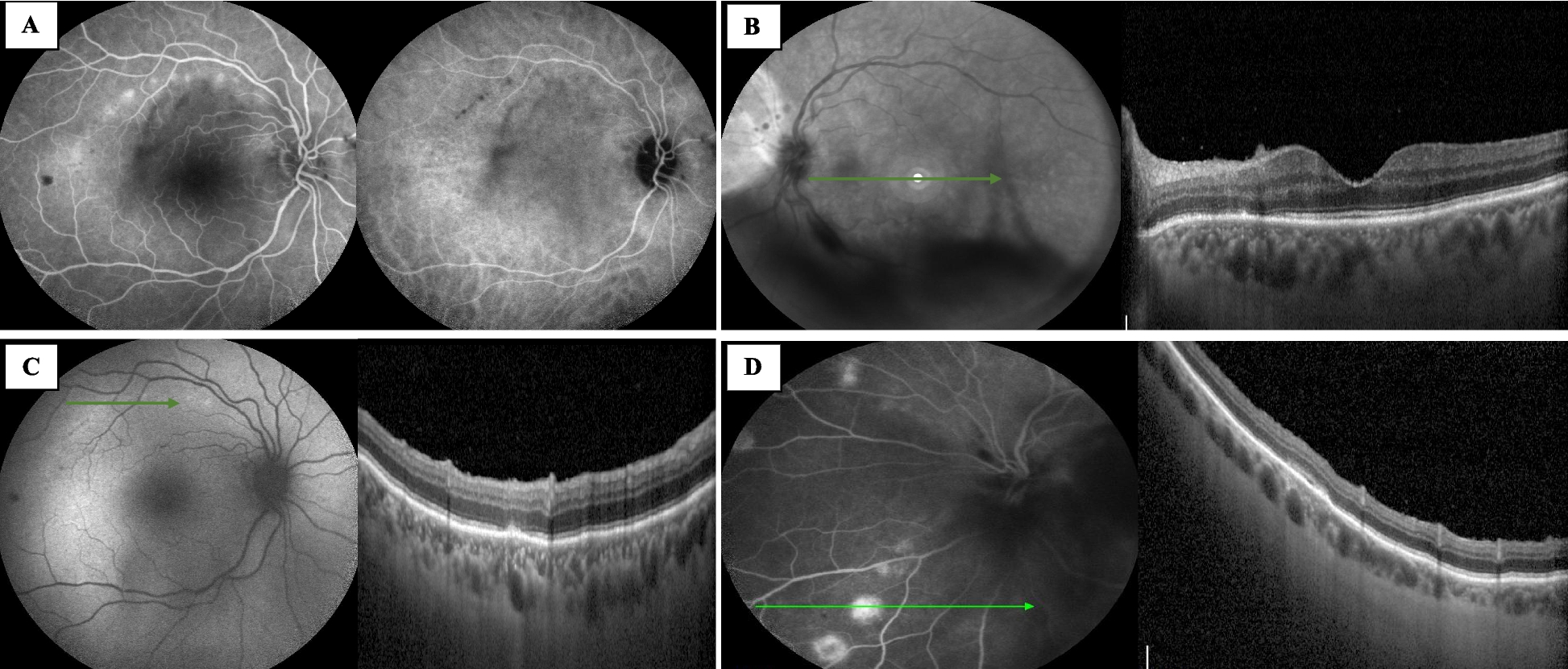
VKH disease and CSC are considered to be completely different diseases with different pathophysiologies. However, CSC may clinically mimic VKH or develop in VKH cases. Hence, it is of paramount importance to differentiate CSC from the relapse of inflammation once dome-shaped neurosensory retinal detachment reoccurs or worsens in VKH, as the management of these two conditions is paradoxical. Delayed diagnosis of CSC lead to permanent retinal damage with subsequent poor visual prognosis [15, 16]. Multimodal imaging examinations are useful in discriminating CSCs from VKH. On OCT, fluctuations of ILM, subretinal septa, subretinal membranous structures and hyperreflective dots, bulges of RPE, folds of RPE, and a resultant high RPE undulation index are characteristics of VKH. However, isolated serous PED always points to CSC because of its high prevalence in CSC, and it is regarded as an intermediate stage between pachychoroid and classic CSC [15, 17,18,19,20]. Meanwhile, mechanical disruption at the RPE level is the most plausible factor responsible for generating the focal leakage points in CSC [21]. The subfoveal choroidal thickness increases markedly during the acute phase of both VKH and CSC, and it is thicker in acute VKH than in acute CSC [17, 19]. The thick choroid of acute VKH is diffuse and homogenous and the infiltration of inflammatory cells and the proteinaceous fluid exudates may obscure the choroidal vessel margin [22]. Nevertheless, the choroidal thickening of CSC is considered to result from a thinned inner choroidal layer and enlarged underlying hyporeflective choroidal lumina [22,23,24]. The typical FFA manifestations of VKH are numerous punctate hyperfluorescent dots at the RPE level in the early stage, followed by staining and pooling of the dye in the subretinal space, optic disc hyperfluorescence, and leakage in the late stage [3]. Nonetheless, in classic CSC, unifocal leakage at the RPE level with an “ink-blot” or “smokestack” pattern is typical, but in eyes with steroid-induced CSC, the intense leakage from multiple regions is often seen [15, 25]. Typical ICGA signs of VKH include early hyperfluorescent stromal vessels, late hypofluorescent dark dots, and fuzzy or lost vascular patterns of large stromal vessels due to choroidal inflammation [1,2,3, 26]. Whereas geographic areas of hyperfluorescence with blurred contours are the hallmark of choroidal hyperpermeability in CSC [15].
The explicit pathogenesis of VKH and CSC remains poorly understood. In acute VKH, the diffuse and homogenous choroidal inflammation leads to multiple blood-retinal outer barrier dysfunctions, so multiple accumulations of fluid with the abundant protein under the neurosensory retina occur, which are distinctive signs of acute VKH [1, 27].. Occasionally, the unusual sign of PED occurs in acute VKH cases, whose pathophysiology is speculated to be composed of hyperpermeability of choroidal vessels resulting from choroidal inflammation and the relatively high hydrostatic pressure across the swelling choroidal vascular bed [7]. In contrast, high hydrostatic pressure in the choroid is believed to be the primary underlying pathophysiology in classic CSC, which pushes the RPE forward to relieve pressure and causes RPE detachment from the Bruch membrane [28]. The PED enlarges as the pressure further increases, which will add angulation and mechanical stress to the base of the PED and may weaken or rupture the RPE monolayer layer [28, 29]. The prospective study of acute CSC indirectly confirms these pathological processes, and transverse and RPE fit C-scans matching the leakage site were superimposed on an OCT fundus photograph and linked to the leakage location on the FFA, in which PED was observed in 85% of eyes and RPE microrips were detected in 54.5% of eyes [21]. Once the excessive hydrostatic pressure is released, there are no more persistent triggers in CSC. Therefore, the possibility of spontaneous resolution of the serous neurosensory retinal detachment is relatively high, and observation is the main treatment modality. As Gupta et al. reported in the natural course of CSC, RPE microrips close spontaneously [21].
Interestingly, VKH and CSC seemed to occur simultaneously in case 10 before corticosteroid application since multimodal images revealed characteristic changes in both VKH and CSC at her first visit, just one day after the disease onset. On the second FFA, both multiple subretinal staining and optic disc hyperfluorescence disappeared after corticosteroid therapy, indicating that the high-dose systemic corticosteroid has effectively suppressed acute intraocular inflammation. Meanwhile, the distinctive signs of CSC are also obvious, and the patient’s vision even continuously deteriorates. The leakage points with ‘ink-blot’ on the second FFA coincide with the intense hyper-fluorescence of the first FFA, and ICGA shows the apparent dilatation of large choroidal veins. The persisted ERDs and PED in both eyes subsided gradually after one month of discontinuation of oral prednisone, continuous treatment of immunosuppressants and biologics, and the subthreshold micropulse laser for RPE microrips. Importantly, there was no recurrence of ocular inflammation or neurosensory retinal detachment throughout the whole follow-up. These results suggest that VKH and CSC occurred simultaneously in case 10 at the onset of the diseases. According to this case, we can speculate that in other VKH and PED patients, the initial PED may result from a combination of two distinct mechanisms: inflammation of VKH and high hydrostatic pressure. The PED resolves with high-dose systemic corticosteroid treatment if the main cause is inflammation of VKH, or develops into classic CSC once high hydrostatic pressure is the main cause.
PED is a common sign in CSC, in which the prevalence of PED with or without associated ERD is reported to be 44.2–100% [15, 17,18,19]. Conversely, PED is observed in 0–10% of eyes with acute VKH disease, according to several cross-sectional OCT-based studies [17,18,19,20, 30]. The prevalence of PED in acute VKH patients in our study is 2.55% (12/470). PEDs resolved with corticosteroid therapy in 7 eyes, while in the other 5 eyes PEDs persisted and colocalized classic CSC developed during the treatment course. To further determine the relationship between PED and CSC development in VKH patients, we proposed the PEDA, an index reflecting the PED deformation and hydrostatic pressure, to predict the outcomes of PED. The calculation of PEDA is simple and can be easily applied clinically. Since the PEDA formed between the lifted RPE and Bruch membrane represents primarily superoinferior stretches, a lower PEDA value indicates a smaller horizontal and greater perpendicular PED dimension, implying a higher hydrostatic pressure and more RPE stretches. Therefore, once the hydrostatic pressure further increases under the treatment of systemic corticosteroid, patients with small PEDA may be more likely to develop defects of the RPE monolayer to relieve pressure, which is the classic CSC. Our measurement values of initial PEDA demonstrate the hypothesis, in which the PEDA values in the CSC group were significantly smaller than that in the non-CSC group. Moreover, when comparing the PED before and after CSC development in Case 5, we can obviously identify that the pressure within the PED was released after the onset of CSC, the angle of the PED became obtuse and the value of PEDA increased. For VKH patients with small PEDA, immunomodulatory and/or biologicals could be the first choice. If the therapy of rapid and aggressive high-dose systemic corticosteroid along with immunomodulatory and/or biologicals is adopted, close follow-up will be necessary to monitor the changes in PED and the occurrence of classic CSC, and timely adjustment of the therapeutic regimen may lower the risk of vision impairment. In our cohort, the BCVA improvement of the CSC group tended to be less than that of the non-CSC group, although there was no statistical difference due to the small sample size, indicating that the early diagnosis of CSC is important for saving vision.
Discontinuation of corticosteroids is suggested as the first step in the treatment of CSC in ocular inflammatory conditions, and adding immunosuppressants and/or biological agents may be required to control ocular inflammation [14, 31]. CSC leakage points outside the fovea could be treated with continuous-wave laser photocoagulation [14]. In our series, four CSC eyes received subthreshold micropulse laser photocoagulation for foveal leakage and yielded favorable results. In contrast to the traditional continuous-wave laser, the subthreshold micropulse can provide the required activation energy of the RPE cells without damaging the retina [32, 33].
The retrospective nature of the present study brings some limitations. First, these results only provided preliminary conclusions due to a small sample size and low incidence. Second, the application of PEDA was restricted since it could not be calculated in cases where severe vitreous opacities, mature cataracts, or other conditions that prevent the presence of clear OCT recordings. Third, details of the choroid cannot be obtained in every case due to the limited penetration of OCT and poor delineation of the deeper posterior border of the choroid, and it is better to use enhanced depth imaging mode scans of OCT for precise measurement in future clinical cases. Despite its limitations, the study certainly adds to our understanding of the associations between PED in VKH patients and CSC development. Further research is needed to confirm the predictive value of PEDA and to clarify the mechanism of classic CSC development in VKH cases.





留言 (0)