
記住我









Initially, the patient was admitted to the hospital with a STEMI (ST- Elevation myocardial infarction). Three DES (Drug Eluting Stents) were implanted in the LAD (Left anterior descending artery) and its diagonalis branch. The interventional cardiologists, did not express any suspicion about possible mass lesions in and around the pulmonary artery at the time of coronary artery stenting.
While still in the hospital, the patient developed ventricular fibrillation four days later. ROSC (Return of spontaneous circulation) occurred after a ten-minute resuscitation.
The patient was then transferred to the ICU (Intensive care unit). He was in need of catecholamines, had ventricular tachycardia, and was on invasive ventilation when he was admitted to the ICU. He eventually transitioned to a sinus rhythm after receiving further medication.
A TTE (Transthoracic echocardiography) showed a reduced left ventricular ejection fraction (LVEF) and a dilated right ventricle with signs of acute right heart load. The thorax CT-scan showed a massive bilateral pulmonary embolism. Heparin medication was initiated, and the patient was immediately transferred to a tertiary care hospital’s cardiology department.
After exclusion of an intracranial hemorrhage via cranial CT-scan, a lysis therapy with Alteplase followed. The patient was extubated the next day and weaned off the catecholamines. The following TTE two days after lysis showed a regressive right heart load, slight tricuspid valve insufficiency (TAPSE = 22 mm, PAPdpmax = 43mmHg + 10mmHg CVP) and a slightly reduced LVEF, with the pulmonary valve described as inconspicuous.
The patient was transferred back to the referrer hospital on the third day, with the recommendation for therapeutic anticoagulation and further examination to identify the source of the emboli.
The patient was released home and then proceeded to a rehabilitation clinic for physical treatment after his further stay in the hospital was uneventful.
Twenty days later while in the rehabilitation center the patient got an extreme tachyarrhythmia, as well as acute onset of dyspnea and was taken to the hospital (one and a half months after the STEMI).
An emergency surgery was required due to suspicion of an apical aneurysm with covered perforation of the ventricle, an additional three centimeter pericardial effusion with compression of the right ventricle, and suspected recurrent thrombus in the pulmonary artery and RVOT (Right ventricular outflow tract) (TTE before surgery: TR PPG 40mmHg; TAPSE normal range; pulmonary valve Vmax 2.5 m/s. RV-PA PPG/MPG 24/14 mmHg; thrombus in pulmonary artery and right ventricular outflow tract (3.6 × 8.3 cm)).
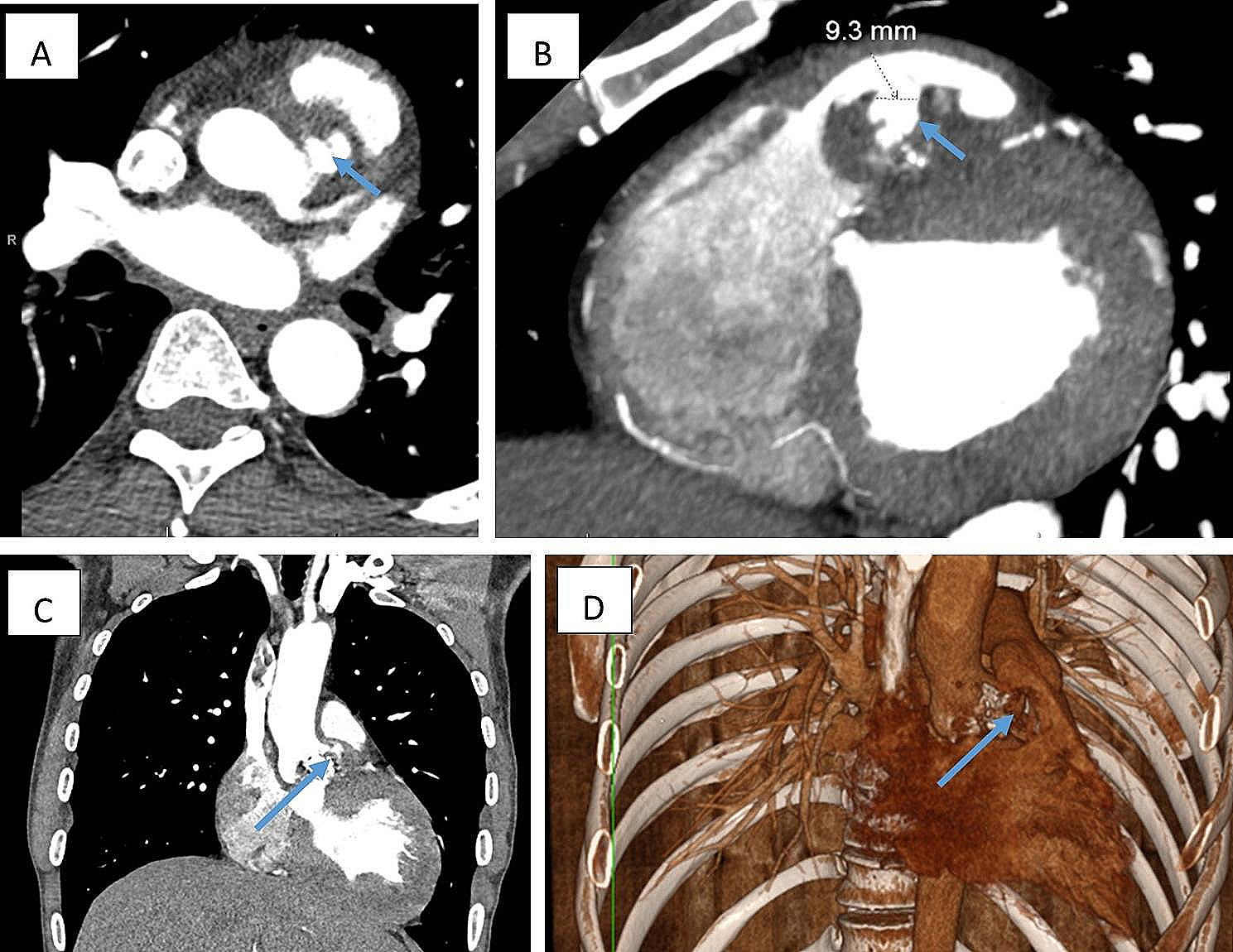
On the same night, a CT-scan revealed a mass in the pulmonary artery, RVOT, and pulmonary valve (Fig. 1). The patient was immediately transferred to a specialized cardiac surgery center for an urgent operation.
Fig. 1
Preoperative CT-scan showing the tumor in the main and right pulmonary arteries
For the operation the ascending aorta and both caval veins were cannulated after opening the pericardium, removing 400 ml blood from the pericardial cavity, and heparinization. The patient was then cooled to 33 °C. Two liters of Custodiol solution were used for cardioplegia.
After a longitudinal opening of the main pulmonary artery, a tumor adherent to the lateral wall of the pulmonary artery, covering almost its entire lumen, with infiltration of the pulmonary valve and extension to the RVOT was seen. Resection of the tumor from the lumen of the pulmonary artery together with the lateral wall of the artery, the pulmonary valve, and the infiltrated part of the RVOT followed. After the above-mentioned portions were removed, local metastases were seen on the main right pulmonary artery. Further, the tumor had also infiltrated the dorsal wall of the main pulmonary artery, the upper wall of the left atrium, and the left ventricle. A complete resection was not possible. Further revision of the distal branches of the pulmonary artery was not performed.
After that, the RVOT was reconstructed. Seven 2−0 Ethibond pledgeted sutures were placed in the height of the previous pulmonary valve annulus. Following the measurement, a partial implantation of a 25 mm CE Perimount bioprosthesis was performed with the help of the previously inserted pledgeted sutures. A 10 × 4 cm Gore-Tex-Patch was used to reconstruct the RVOT. The patch was sewn up to the level of the pulmonary valve using a 4 −0 Prolene continuous suture. The rest of the pulmonary valve was implanted on the Gore-Tex-Patch using 2 − 0 Ethibond pledgeted sutures. The patch’s upper part was then sewn to the pulmonary artery’s lateral wall to repair it (Fig. 2).
Fig. 2
A section of the resected tumor
The weaning from cardiopulmonary bypass was uneventful.
Intraoperative TEE (transesophageal echocardiography) showed a good function of the implanted pulmonary valve.
The patient’s postoperative recovery was uneventful. The histological findings confirmed the suspicion of a high-grade angiosarcoma. PET/CT also showed that the tumor had progressed to the left ventricle. Metastases were not discovered. After discussion of the case in our tumor board the patient was scheduled to begin chemotherapy after some recovery time. On the 13th postoperative day, he was discharged and died two months later at home.
留言 (0)