
記住我





First-trimester bleeding occurs in 20–40% of pregnancies and accounts for almost 500,000 emergency department (ED) visits in the United States annually.1,2 The most common causes for these presentations include threatened miscarriage and the spectrum of early pregnancy loss; however, more serious etiologies include ectopic pregnancy.2 The criteria for diagnosing ectopic pregnancy include an extrauterine yolk sac or embryo on ultrasonogram, rising or plateauing quantitative β-hCG levels without products of conception on uterine aspiration, or visualization at laparoscopic surgery with subsequent histologic confirmation.3,4 However, these criteria are often not met, and many patients receive a diagnosis of pregnancy of unknown location. This diagnosis often entails extensive follow-up, involving serial β-hCG tests, repeat ultrasonograms, and multiple office visits. Of concern, several studies have found an increase in the number of ruptured ectopic pregnancies during the coronavirus disease 2019 (COVID-19) pandemic.5,6 Numerous challenges have arisen while caring for patients in the midst of this pandemic, including isolation precautions, the need for additional supplies, and providing limited hands-on patient care without compromising the quality of care. Furthermore, patient hesitation in seeking medical attention has increased, adding another challenge for health care professionals. These changes have further highlighted the need to optimize the current approach to first-trimester bleeding to both reduce patient reluctance in seeking medical care and better utilize the resources and visits involved in the evaluation of pregnancy of unknown location.
This study aimed to validate the use of a bedside test strip to improve the evaluation of pregnancy of unknown location in individuals who present with first-trimester vaginal bleeding. This bedside test is based on prior research that has already validated the use of alpha-fetoprotein (AFP) to diagnose miscarriage.7 The initial proof of concept was based on the quantification of AFP in vaginal blood and in maternal serum. In a pregnant individual at any gestational age, the AFP concentration is at least 1,000 times higher in the fetal serum than in the maternal serum. Therefore, high AFP concentrations in the vaginal blood are suggestive of the passage of embryonic or fetal tissue and, hence, miscarriage.7,8 A second study demonstrated the successful same-day diagnosis of miscarriage by sampling blood collected on hygienic pads and the quantitative measurements of AFP using an automated laboratory analyzer.8
The current study was designed to offer a simple diagnostic alternative that does not require the use of an automated laboratory analyzer. More specifically, this study aims to validate the accuracy of bedside lateral flow immunoassay test strips for AFP in correctly detecting embryonic or fetal tissue. We chose to evaluate the only AFP-detecting strip with U.S. Food and Drug Administration (FDA) approval, the ROM Plus test strip. ROM Plus is a medical device originally intended for use in the detection of amniotic fluid leakage that detects not only AFP, but also insulin-like growth factor–binding protein 1 (IGFBP-1). Insulin-like growth factor–binding protein 1 is a protein present in extraembryonic coelomic fluid, adjacent to the chorion, and is also expressed by the fetal liver and kidneys.9 Similar to AFP, IGFBP-1 levels in amniotic fluid and embryonic tissue are up to 100–1,000 times higher than in maternal serum.10–12 Although there are no prior data on the detection of IGFBP-1 in the diagnosis of miscarriage, as with AFP, it would presumably be similarly sensitive in detecting miscarriage given the marked difference in concentrations demonstrated between embryonic or fetal serum and maternal serum. This potentially increases the veracity of the test strip for the detection of miscarriage, because the strip detects an additional protein present in embryonic and fetal tissue. Furthermore, should the test strip result be positive for the passage of embryonic or fetal tissue in vaginal blood, we hypothesized that this could not only diagnose a miscarriage, but also rule out the presence of an ectopic pregnancy.
METHODSThis study received IRB approval from the Maimonides Medical Center IRB (project number 2020-12-09) and the Yale University IRB (project number 2000023829). This was a prospective cohort study including individuals recruited between January 2020 and August 2021 from Maimonides Medical Center and the Yale Health System (convenience samples). Written consent was obtained from all study participants.
The inclusion criteria included both pregnant and nonpregnant individuals, older than age 18 years, presenting with vaginal bleeding or who were scheduled for dilation and curettage (D&C). Exclusion criteria included individuals with diagnosed malignancies that could potentially affect the AFP concentrations in serum or vaginal blood (eg, liver cancer) and pregnant individuals with multiple or molar pregnancies.
Three groups were evaluated. The negative control group included nonpregnant individuals undergoing D&C or experiencing spontaneous vaginal bleeding (eg, menstrual flow or abnormal uterine bleeding). The positive control group included individuals with confirmed intrauterine pregnancy undergoing D&C for termination of pregnancy or missed miscarriage. Intrauterine pregnancy was confirmed by histopathology to contain an embryonic or fetal tissue component, rather than just placental tissue, as observed in complete moles. Finally, the study group included pregnant individuals with first-trimester bleeding. These individuals were followed by the research team until a definite pregnancy diagnosis was obtained. Individuals with pregnancies that could not be confirmed as ectopic or intrauterine were excluded from the test performance analysis.
To calculate the minimum required samples, a large effect size of 0.85 was used based on prior data indicating that the mean AFP concentration in fetal serum is about 10,000-fold higher than in maternal serum.7,8 To achieve a power of 80%, the minimum number of samples in each group was calculated to be 22. In this study, the number of recruited individuals exceeded this minimum.
We defined active miscarriage as incomplete or inevitable miscarriage with vaginal bleeding. We also included patients with an open cervix immediately after the passage of fetal tissue in the active miscarriage group. Threatened miscarriage was defined as vaginal bleeding in the setting of an ongoing, viable intrauterine pregnancy and a closed cervix. Complete miscarriage was defined as vaginal bleeding and no intrauterine fetal tissue after a previously documented intrauterine pregnancy and a closed cervix. Ectopic pregnancy was defined as an extrauterine fetal pole or yolk sac seen on official ultrasonogram or confirmed by histopathology after surgery. If surgery was performed, an attempt was made to aspirate the fluid from an intact gestational or yolk sac using a 21-gauge, 4-cm–long needle with a syringe. These ectopic pregnancy fluid samples were also tested with the test strips and sent for AFP quantification (Roche Cobas e411 automated analyzer).
The blood specimens were tested for the presence of embryonic or fetal tissue using ROM Plus, an FDA-approved kit that contains a cotton swab, diluting solution, and a lateral flow immunoassay strip capable of detecting AFP and IGFBP-1. The detection thresholds for AFP and IGFBP-1 were 150 ng/mL and 5 ng/mL, respectively. Vaginal blood was collected by introducing a swab into the vagina or by absorption through a hygienic pad or gauze. The swab or piece of pad was inserted into the solution provided in the kit, and the test strip was then introduced into the diluting solution. A positive test result produced two bars on the test strip, and a negative test result produced a single control bar. See Video 1 for details.
When applicable, official ultrasonograms, β-hCG tests, and histopathology reports were reviewed by the study team to confirm pregnancy status and the presence or absence of embryonic or fetal tissue in the vaginal blood or specimens evacuated from the uterine cavity. A sensitivity and specificity analysis was performed to validate the performance of the test. In addition, positive samples for AFP (either the swab, pad, or gauze) were refrigerated at 4°C in specimen containers and retested 3–20 days later to ascertain the stability of AFP and reliability of the test.
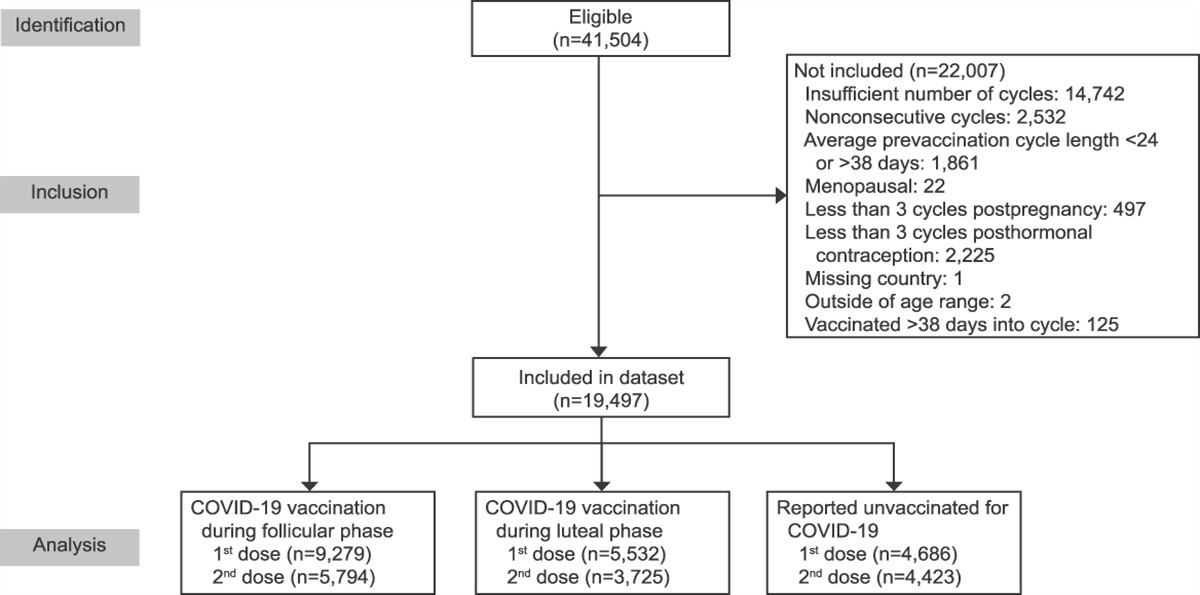
RESULTSA total of 90 individuals were recruited for the study (Fig. 1). In the negative control group, 22 of the 23 samples tested negative for the presence of embryonic or fetal tissue using the test strip. In the positive control group, 31 of the 31 samples tested positive for the presence of embryonic or fetal tissue using the test strip. The study group (n=36) included 12 individuals with ectopic pregnancy, 16 with incomplete or inevitable miscarriage (ie, active miscarriages), four with threatened miscarriage, and four with complete miscarriage. The vaginal blood samples from all 12 individuals with ectopic pregnancy, all four with threatened miscarriage, and all four with complete miscarriage tested negative for embryonic or fetal tissue using the test strip. Of the 16 individuals with active miscarriage, 14 had accurate positive test results for the presence of embryonic or fetal tissue using the test strip. Of note, we were able to obtain a definitive diagnosis in real time or retrospectively for all 36 individuals in the study group, with no remaining cases diagnosed as pregnancy of unknown location.
 Fig. 1.:
Fig. 1.: Research groups. Red text indicates the groups with embryonic or fetal tissue expected to be present in vaginal or uterine blood samples. Black text indicates groups without expected embryonic or fetal tissue in vaginal or uterine blood samples. D&C, dilation and curettage.
Overall, 47 individuals had confirmed vaginal or uterine blood samples with embryonic or fetal tissue. The test strip was accurately positive in 45 of those 47 cases (Table 1), resulting in a test sensitivity of 95.7% (Table 2). The remaining 43 individuals had confirmed absence of embryonic or fetal tissue in their vaginal or uterine blood samples. The test strip correctly identified 42 of those 43 cases (Table 1), resulting in a test specificity of 97.7%.
 Table 1.:
Table 1.: Test Strip Results Compared With the Clinical Diagnosis
 Table 2.:
Table 2.: Test Strip Performance*
Of the two samples with false-negative test results using the test strip, the first was a sampling error. This occurred when the sample was transferred from gauze to cotton swab, resulting in no vaginal blood being added to the diluting solution. On repeat testing, with the presence of vaginal blood, this sample correctly tested positive with the test strip. The second false-negative result was in the setting of hemorrhage, which likely resulted from massive dilution of fetal AFP or IGFBP-1 by maternal blood.
Regarding AFP stability, on retesting 15 of the positive samples, which was performed 3–20 days later, the results remained the same—a positive test result using the test strip. The only false-positive result contained a very faint test bar, as interpreted by one of the study team members. On repeat testing, this test clearly had a negative result, with the appearance of only a single control bar on the test strip.
Among the 12 ectopic pregnancies in our study, three were unruptured ectopic pregnancies in the fallopian tube that were removed by laparoscopic salpingectomy. The fluid from the intact gestational sac or yolk sac was aspirated using a 21-gauge, 4-cm–long needle with a syringe. These fluid samples were also tested with the test strips as well as being sent for AFP quantitative assay (Roche Cobas e411 analyzer). In all three cases in which fluid was obtained directly from the ectopic pregnancy during laparoscopy, the test strips showed positive results and the measured levels of AFP ranged from 3,000 to 7,000 ng/mL. In these three cases, the corresponding vaginal blood samples were negative.
Regarding the exclusion criteria, none of the study participants had a known AFP-producing malignancy, higher order pregnancy, or any form of gestational trophoblastic disease.
DISCUSSIONThis study was designed to validate the accuracy of a bedside lateral flow immunoassay test platform for AFP and IGFBP-1 (ROM Plus) to accurately detect embryonic or fetal tissue. We found that the test strip can accurately and reliably detect either the presence or absence of embryonic or fetal tissue. In cases with embryonic or fetal tissue present, such as active miscarriage or suction D&C, test sensitivity was 95.7%. In the absence of embryonic or fetal tissue, such as vaginal blood sampled in cases of ectopic pregnancy, threatened or complete miscarriage, or nonpregnant individuals, the test strip had a specificity of 97.7% for obtaining a negative result. These high sensitivity and specificity performance values were obtained with all tests being performed in real-time, common clinical scenarios encountered in a high-volume, urban obstetrics and gynecology unit. The kappa agreement coefficient was 0.93, a near perfect agreement between the test readers and the clinical diagnosis.
The ROM Plus test is based on a lateral flow immunoassay strip for AFP and IGFBP-1. It was originally created for diagnosing rupture of amniotic membranes (https://www.laborie.com/blog/product/rom-plus-range/). This study describes an off-label use of ROM Plus, which broadens its utility to the evaluation of early pregnancy bleeding. Given that this product tests for two proteins, both present at significantly increased levels in pregnancy tissue compared with maternal serum, the sensitivity may be increased in comparison with test kits capable of detecting AFP alone. Furthermore, this study evaluates the use of an FDA-approved bedside product, which we believe increases the veracity of our data because they are based on a test strip that has undergone a rigorous approval process dictated by the FDA.
There are limitations to this test. Technical errors in sample collection and testing may occur, as we experienced in our study. For example, there was one false-negative result on initial testing due to no vaginal blood being added to the diluting solution (after an attempt to transfer a sample from one medium to the other). On retesting, this sample correctly tested positive when vaginal blood was in contact with the test strip. Typical use of the test kit, with at least some vaginal blood introduced to the solution, produced the correct results in all other cases. Another limitation of this test was observed in the case of hemorrhage. The presence of very large amounts of maternal blood may dilute the embryonic or fetal component containing AFP and IGFBP-1 to the point of reaching a false-negative result. This was encountered in one case of active miscarriage in our study. Other limitations may be related to rare scenarios that we did not encounter in our current study. These scenarios may include heterotopic pregnancies, interstitial ectopic pregnancies (accounting for only 2–6% of all ectopic pregnancies13), or twin pregnancies in which there is loss of one twin with preservation of the other, leading to confounding results. In these scenarios, clinical judgment is paramount.
Outside of these rare situations, this bedside test has proven to be both highly sensitive and specific in common obstetric scenarios, with a vast array of possible applications. It can be used in EDs, outpatient clinics, and even potentially by patients in their homes if it were to become available over-the-counter. In the case of ED or office presentations, this test could be used for almost any pregnant patient with vaginal bleeding to determine whether embryonic or fetal tissue is present in that vaginal blood. In the instance of no prior documented intrauterine pregnancy, a positive test result (ie, presence of embryonic or fetal tissue in vaginal blood) could allow physicians to more comfortably forego the additional serum and ultrasound testing and subsequent visits involved in a pregnancy of unknown location workup, thereby likely decreasing time, expense, and uncertainty on the part of the patient and the physician. We encountered this scenario in four cases in which ultrasonography did not identify the location of the pregnancy, but the test strips were positive for AFP and histopathology retrospectively confirmed a miscarriage. These cases reinforce the utility of this test in expediting a final diagnosis and avoiding unnecessary tests and interventions such as methotrexate for pregnancy of unknown location. However, a negative test result (ie, absence of embryonic or fetal tissue in vaginal blood) in a pregnancy of unknown location workup may represent an ectopic pregnancy, a complete miscarriage, or a threatened miscarriage. Therefore, a negative test result should still mandate detailed history taking, close follow-up, and maintaining a high suspicion for ectopic pregnancy until proven otherwise.
In the case of a previously documented intrauterine pregnancy, a negative test result may offer reassurance that the vaginal bleeding is not fetal in origin and a positive test result may reinforce the diagnosis of miscarriage. Furthermore, on repeat testing 3–20 days later, the positive test results remained consistent, indicating the stability of at least one of the proteins (AFP, IGFBP-1, or both), which allows for delayed testing if a patient does not present immediately. For example, if a patient brings in embryonic or fetal tissue or a pad with dried vaginal blood days later, this test could still be reliably used to detect embryonic or fetal tissue and facilitate a diagnosis.
We were able to demonstrate that, in all three cases of ectopic pregnancy in which the ectopic pregnancy tissue could be sampled directly, the test strip result was positive, with these results confirmed using a quantitative AFP analyzer. All of the corresponding vaginal blood samples showed negative test strip results, as expected. This is an additional piece of evidence corroborating the clinical advantages provided by the test.
The utility of this test can also go beyond presentations to health care professionals. In cases of patients with confirmed intrauterine pregnancies, this test kit may be used in the presence of vaginal bleeding at home, a significant benefit during the COVID-19 pandemic. With patient education and counseling, the test strip kit may allow individuals to screen themselves at home, particularly those hesitant to present to medical departments or those in remote areas. This added knowledge of a positive or negative test result may also allow patients to be more prepared and potentially give them added confidence in seeking medical care when needed. Furthermore, given the increasing abortion care restrictions, another benefit of this test may be earlier diagnosis of miscarriage. In states with greater restrictions, physicians may need to take additional steps to diagnose early pregnancy loss; this test may aid in and expedite this diagnosis to hopefully decrease the barriers to care some individuals may experience.
We found that a test strip that detects AFP and IGFBP-1 accurately and reliably identifies the presence of embryonic or fetal tissue in vaginal blood and uterine samples. When positive, this may be a vital, noninvasive aid in ruling out ectopic pregnancy and diagnosing miscarriage at the bedside. A simple bedside test is highly desirable given its potential for reducing the number of visits, investigations performed, and personnel involved in the evaluation of first-trimester bleeding and pregnancy of unknown location.
REFERENCES 1. Wittels KA, Pelletier AJ, Brown DF, Camargo CA Jr. United States emergency department visits for vaginal bleeding during early pregnancy, 1993-2003. Am J Obstet Gynecol 2008;198:523.e1–6. doi: 10.1016/j.ajog.2007.11.011 2. Norwitz ER, Park JS. Overview of the etiology and evaluation of vaginal bleeding in pregnancy. Accessed April 10, 2022. https://www.uptodate.com/contents/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnancy 3. Tubal ectopic pregnancy. ACOG Practice Bulletin No. 193. American College of Obstetricians and Gynecologists. Obstet Gynecol 2018;131:e91–103. doi: 10.1097/AOG.0000000000002560 4. Tulandi T, Levine D, Schreiber CA. Ectopic pregnancy: clinical manifestations and diagnosis. Accessed March 15, 2022. https://www.uptodate.com/contents/ectopic-pregnancy-clinical-manifestations-and-diagnosis 5. Dvash S, Cuckle H, Smorgick N, Vaknin Z, Padoa A, Maymon R. Increased rate of ruptured tubal ectopic pregnancy during the COVID-19 pandemic. Eur J Obstet Gynecol Repord Biol 2021;259:95–9. doi: 10.1016/j.ejogrb.2021.01.054 6. Casadio P, Youssef A, Arena A, Gamal N, Pilu G, Seracchioli R. Increased rate of ruptured ectopic pregnancy in COVID-19 pandemic: analysis from the North of Italy. Ultrasound Obstet Gynecol 2020;56:289. doi: 10.1002/uog.22126 7. Mor A, Tal R, Haberman S, Kalgi B, Nasab SH, Minkoff H. Same-day confirmation of intrauterine pregnancy failure in women with first-and early second-trimester bleeding. Fertil Steril 2018;109:1060–4. doi: 10.1016/j.fertnstert.2018.02.006 8. Mor A, Gardezi M, Jubanyik K, Simsek B, Seifer DB, Patrizio P, et al. Miscarriage determination in first trimester based on alpha-fetoprotein extracted from sanitary pads. Fertil Steril 2021;116:462–9. doi: 10.1016/j.fertnstert.2020.10.006 9. Martina NA, Kim E, Chitkara U, Wathen NC, Chard T, Giudice LC. Gestational age-dependent expression of insulin-like growth factor-binding protein-1 (IGFBP-1) phosphoisoforms in human extraembryonic cavities, maternal serum, and decidua suggests decidua as the primary source of IGFBP-1 in these fluids during early pregnancy. J Clin Endocrinol Metab 1997;82:1894–8. doi: 10.1210/jcem.82.6.3974 10. Rutanen EM, Bohn H, Seppälä M. Radioimmunoassay of placental protein 12: levels in amniotic fluid, cord blood, and serum of healthy adults, pregnant women, and patients with trophoblastic disease. Am J Obstet Gynecol 1982;144:460–3. doi: 10.1016/0002-9378(82)90254-x 11. Rutanen EM, Pekonen F, Kärkkäinen T. Measurement of insulin-like growth factor binding protein-1 in cervical/vaginal secretions: comparison with the ROM-check Membrane Immunoassay in the diagnosis of ruptured fetal membranes. Clin Chim Acta 1993;214:73–81. doi: 10.1016/0009-8981(93)90304-m 12. Nonoshita LD, Wathen NC, Dsupin BA, Chard T, Giudice LC. Insulin-like growth factors (IGFs), IGF-binding proteins (IGFBPs), and proteolyzed IGFBP-3 in embryonic cavities in early human pregnancy: their potential relevance to maternal-embryonic and fetal interactions. J Clin Endocrinol Metab 1994;79:1249–55. doi: 10.1210/jcem.79.5.7525630 13. Brincat M, Bryant-Smith A, Holland TK The diagnosis and management of interstitial ectopic pregnancies: a review. Gynecol Surg 2019;16:2. doi: 10.1186/s10397-018-1054-4
留言 (0)