
記住我


The COVID-19 pandemic has caused significant morbidity and mortality across the globe, but children seem to be much less affected than adults.
During the first wave of the pandemic, a cluster of patients presenting with signs of hyperinflammation, cardiovascular shock and fever was identified1 with similar cases appearing in the following weeks. This was defined as paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) by the Royal College of Paediatrics and Child Health (RCPCH)2 followed by the Centers for Disease Control and Prevention (CDC),3 who described it as multisystem inflammatory syndrome in children (MIS-C).
During its first emergence in the UK, most patients were transferred to tertiary centres for management, collaboratively with paediatric infectious diseases (PID), cardiology and paediatric intensive care unit (PICU) teams.4 However, as our understanding of the condition has developed, more patients are now managed in a district general hospital (DGH), with virtual multidisciplinary team (MDT) involvement. Challenges include diagnostic uncertainty, access to investigations, the variable clinical phenotypes of PIMS-TS, high impact of complications and the requirement for specialist input.5
Here we present a structured approach to management of children presenting with suspected PIMS-TS in a DGH.
DefinitionChildren frequently present with a history of persistent fever, associated with gastrointestinal symptoms and/or mucocutaneous manifestations. Respiratory symptoms are infrequent6 (table 1). Many children seem relatively well at presentation but have disproportionately marked fever and/or unusual mucocutaneous features.
Table 1Case definition for novel hyperinflammatory condition seen in children during COVID-19 pandemic from RCPCH and CDC
The median age is 9 years, but cases have been described as early as 3 months of age. There seems to be a male predominance, and most children have no underlying comorbidities.7 Black, Asian and minority ethnic (BAME) groups appear to be more affected, and SARS-CoV-2 exposure in the preceding 4–6 weeks was commonly found in these patients.4
Initial evaluation in the emergency departmentA thorough history and examination is vital to establish features of PIMS-TS, attempt to differentiate it from its clinical mimics and identify complications that may preclude the patient from being managed in the DGH.
Deciding which children to investigate can be challenging; children with early PIMS-TS are often deceptively well looking, but self-limiting febrile illness remains a more common presentation, and overinvestigation should be avoided. We suggest a pragmatic two-stage approach, supported by the national consensus pathway8 (figures 1 and 2).
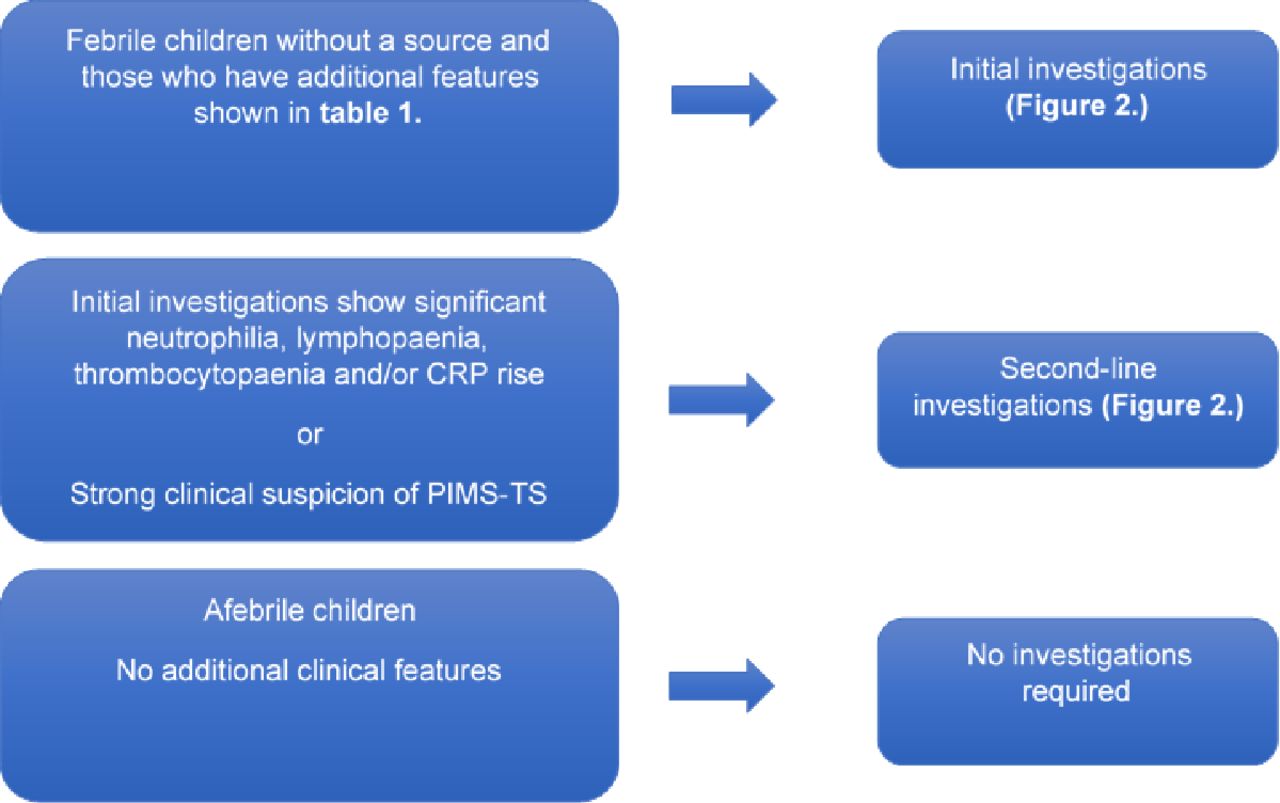 Figure 1
Figure 1 Decision-making chart of investigation.
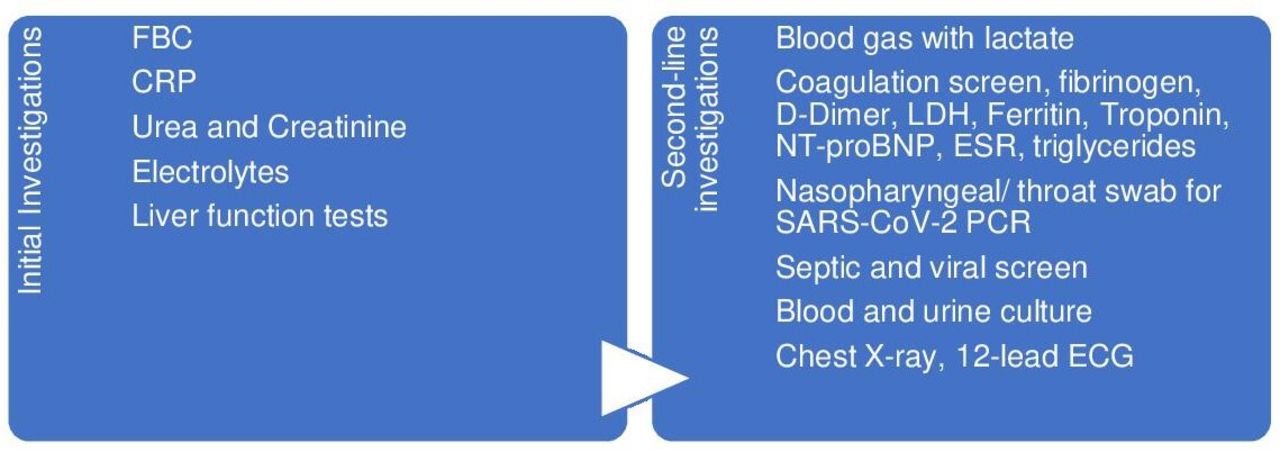 Figure 2
Figure 2 Investigations in children with suspected PIMS-TS. CRP, C reactive protein; ESR, erythrocyte sedimentation rate; LDH, lactic acid dehydrogenase; PIMS-TS, paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2.
There are reports of children who present appearing well and are discharged home, but re-present to hospital following rapid clinical deterioration.9 Therefore, robust safety-netting advice should be given to parents/carers.
Second-line investigations should include a chest radiograph and a 12-lead ECG, looking for signs of myocarditis (T wave inversion, pathological Q waves and ST changes).10 Additional investigations might be required depending on the severity of presentation (box 1). D-dimer results should be interpreted carefully, as there is little paediatric experience of its response to inflammation.
Box 1 Additional investigationsAbdominal ultrasound: if there is abdominal pain (±surgical input).
Echocardiogram: when criteria for paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 are met.
Save EDTA and serum for PCR and serological studies.
Blood for SARS-CoV-2 serology.
Blood and stool for SARS-CoV-2 PCR.
Blood for pneumococcal, meningococcal, group A Strep and Staphylococcus aureus PCR.
Antistreptolysin O titre and anti-DNAse B.
Epstein-Barr virus (EBV), cytomegalovirus (CMV), adenovirus and enterovirus PCR.
Stool for virology.
All children with PIMS-TS should be invited to join the RECOVERY research study, other relevant studies recruiting locally (including DIAMONDS) and be reported to the British Paediatric Surveillance Unit as a case of PIMS-TS.
Criteria for admission in a DGHMost children managed in the first wave of COVID-19 pandemic presented with severe disease8 and required transfer to a tertiary centre, with 44% needing PICU admission.5
With increasing knowledge of the disease, the current management should be determined by the severity of the clinical picture and selected cases can be managed on a paediatric ward or high dependency unit of a DGH. These children may deteriorate rapidly, and close monitoring is vital. A febrile child with hyperinflammation who is haemodynamically stable can be managed in a DGH, but should be discussed daily with their tertiary team (cardiology, rheumatology or infectious diseases, according to local pathways) to guide risk stratification and management decisions.
An echocardiogram should be performed in the first 24 hours of admission in stable children—if unavailable in the DGH, day transfer to a tertiary unit may be considered—and reviewed by a paediatric cardiologist. Daily bloods including inflammatory markers, clotting profile and troponin/NT-proBNP should be done.
Criteria for transfer to a tertiary centreAll children who present severely ill, with shock and multiorgan failure, should be retrieved to a PICU. Patients who present with concerning features should also be discussed with tertiary centres for potential transfer (table 2). Children with PIMS-TS who develop shock are challenging to manage in a DGH. They can develop profound hypotension and respond unpredictably to fluids. Early PICU advice and retrieval is strongly recommended.
Table 2Features of severe disease requiring transfer to tertiary unit
Cardiovascular instability is the most frequent factor in acute decompensation. Many children have fluid-unresponsive shock or develop signs of cardiac failure with fluid. Consider starting with 5–10 mL/kg bolus and if subsequent boluses are needed, and there are concerns of reduced cardiac function, give 5 mL/kg aliquots to allow more frequent assessments of the response. Inotropes/vasopressors are often needed, and the local team should be prepared to start these before the arrival of the retrieval team. The choice should be guided by clinical condition and local pathways. In some cases mechanical ventilation is required, mostly for cardiovascular support rather than respiratory failure.6
PIMS-TS also has several effects on the heart caused by pancarditis. The wide range of manifestations include pericardial effusion, mild valvar regurgitations, coronary artery dilatation and myocarditis with left ventricular dysfunction. Regular echocardiograms are needed to assess severity; this might be challenging to obtain in a DGH.11 Therefore, children with cardiac involvement should be managed in a tertiary centre.
Differential diagnosisThis novel condition manifests as a hyperinflammatory response with multiorgan involvement, with overlapping features of Kawasaki disease (KD), staphylococcal and streptococcal toxic shock syndrome (TSS) ( figure 3 ) and macrophage activation syndrome/haemophagocytic lymphohistiocytosis. Other differentials include invasive group A streptococcal disease, invasive staphylococcal disease, other bacterial sepsis and viral infections (measles, EBV, adenovirus, parvovirus and enterovirus) and acute abdomen such as appendicitis.12
 Figure 3
Figure 3 Differential diagnosis of PIMS-TS. PIMS-TS, paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2.
How is PIMS-TS different from other conditions?PIMS-TS patients are different from KD and TSS patients, as summarised in figure 4.
 Figure 4
Figure 4 Unique characteristics of PIMS-TS. GI, gastrointestinal; CRP, C reactive protein; CVS, cardiovascular; KDSS, Kawasaki Disease shock syndrome; PIMS-TS, paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2.
However, three distinctive classes of patients can be identified based on the clinical phenotype8: PIMS-TS only, PIMS-TS/KD and PIMS-TS/TSS.
Children with PIMS-TS solely have the least severe presentation, with median age of 7.8 years.
Within the group with PIMS-TS/KD, children are younger (median age 4.5 years) and they have the highest proportion of skin involvement,5 but criteria for KD (complete or incomplete) are not met in about 60% of the cases.13 The incidence of coronary aneurysms seems to be much higher in KD than in PIMS-TS.
Children with PIMS-TS/TSS are older (median age of 11.2 years) and seem to have a more severe presentation with multiorgan involvement.5
Furthermore, evidence supporting a causal link with this new disease and SARS-CoV-2 include a strong temporal association with COVID-19 activity, and the majority of patients are either positive for SARS-CoV-2 on RT-PCR, antibody testing or have history of a close contact with COVID-19.13
However, overlapping features between these syndromes suggest that they may share similar pathophysiology and likely explains why these patients respond to similar therapies.14
ManagementInitial stabilisationOn initial assessment of a child who presents to the hospital with persistent fever, inflammation and evidence of single or multiorgan dysfunction and/or Kawasaki-like features, appropriate personal protective equipment (PPE) should be worn and resuscitation and supportive management started15 ( figure 5 ).
 Figure 5
Figure 5 Management of PIMS-TS in a DGH. CRT, capillary refill time; CXR, chest X-ray; GCS, Glasgow coma scale; IVIG, intravenous immunoglobulin; LDH, district general hospital; PIMS-TS, paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2; PPI, proton-pump inhibitors.
ImmunomodulationIn stable patients with suspected PIMS-TS, if consent is not obtained for the RECOVERY trial, intravenous immunoglobulin (IVIG) should be given unless advised otherwise by the tertiary hospital. Second-line modulation is intravenous methylprednisolone, to be considered in patients remaining unwell 24 hours after IVIG, particularly with ongoing fever. According to the Best Available Treatment Study, no difference in outcomes was found between treatment with glucocorticoids or IVIG as single agents or between the single-agent and dual-agent primary treatments.16
If the child’s condition deteriorates or they do not respond to IVIG or methylprednisolone, then biologicals should be considered (tocilizumab, infliximab and anakinra) and the child should be transferred to a tertiary centre.15
We recommend the use of methylprednisolone as first line in haemodynamically unstable patients for two reasons: first, it contributes to maintaining blood pressure and second, there is a risk of volume overload with IVIG therapy, which could lead to acute decompensation.
Additional supportPlay therapists should be involved in management to reduce anxiety/fear associated with prolonged hospital stays, painful procedures and staff wearing PPE.
Discharge criteria and follow-upChildren admitted to the DGH with PIMS-TS can be considered for discharge once they remain afebrile for over 24 hours, have stable cardiac function and decreasing inflammatory markers. Follow-up should be arranged for 1–2 weeks after discharge and at 6 weeks. An echocardiogram should be performed as part of follow-up, since coronary artery aneurysms may develop even after mild cases.8
Future directionsA growing understanding of PIMS-TS and its management means that more patients can be managed effectively in the DGH. This reduces the need for transfer and pressure on tertiary centres and allows families to stay closer to home. Virtual MDT meetings and well-developed protocols have fostered a safe, collaborative relationship between the DGH and tertiary units, resulting in better patient care. We hope that the lessons learnt through this process can be applied to other conditions in the future.
Test your knowledgeWhich of the following are true regarding epidemiology of paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS)? You may select more than one answer.
The median age at presentation is 12 years.
There is a slight female predominance.
Most children have an underlying comorbidity.
Black, Asian and minority ethnic (BAME) groups are more commonly affected.
Cases have been identified in children as young as 3 months of age.
Which of the following is true regarding investigations for suspected PIMS-TS?
Abdominal ultrasound should be performed in all patients with suspected PIMS-TS.
Stable children may be suitable for day transfer to a tertiary unit for echocardiogram if this is not available in the district general hospital (DGH).
First-line investigation should include ferritin, D-dimer and troponin.
Negative SARS-CoV-2 antibody testing excludes a diagnosis of PIMS-TS.
Second-line investigations should only be performed if initial investigations show significant neutrophilia, lymphopaenia, thrombocytopaenia and/or CRP rise.
Which of the following findings are much more commonly seen in Kawasaki disease than PIMS-TS? You may select more than one answer.
Abdominal pain.
Coronary artery aneurysm.
Mucosal changes.
Raised C reactive protein (CRP).
Signs of cardiovascular shock.
A 10-year-old boy with no significant comorbidities presents to the emergency department in a DGH with a 4-day history of fever, lethargy, rash, sore throat and abdominal pain. There is no clear focus for infection, but he is slightly tachycardic with his fever. He is otherwise haemodynamically stable. Intravenous access is obtained and initial investigations show raised CRP, low lymphocytes and raised neutrophils. Which of the following are true regarding his management?
He should be discussed with a tertiary centre before commencing any further treatment.
Intravenous fluid should be given in 20 mL/kg aliquots in view of his tachycardia.
If he remains haemodynamically stable, ceftriaxone alone should be commenced, along with human intravenous immunoglobulin, unless consent is obtained for the RECOVERY trial.
He should receive low dose aspirin and proton pump inhibitor.
If his chest X-ray, ECG and troponin are normal, there is no indication for echocardiogram.
Which of the following are required when considering children for discharge after treatment for suspected PIMS-TS?
Afebrile >24 hours.
Falling inflammatory markers.
Stable cardiac function.
Plans for outpatient follow-up including echocardiogram.
All of the above.
Answers to the quiz are at the end of the references.
Answers to the multiple-choice questionsD and E.
B.
B and C.
C and D.
E.
Ethics statementsPatient consent for publication
留言 (0)