
記住我





A total of 428 patients with HBV-associated HCC were treated with curative hepatectomy at our institution between March 2013 and December 2017, 296 patients with serum HBV-DNA levels < 2000 IU/mL were included in the study, 157 (53.0%) of whom received antiviral therapy (entecavir 115, tenofovir 37, lamivudine 5), another 139 (47.0%) patients did not receive any form of antiviral therapy. Table 1 shows the baseline characteristics of the entire cohort, with a mean age of 56.5 years, mostly male patients (n = 242, 81.8%), and a Child–Pugh score of A in 291 (98.3%) except for 5 (1.7%) patients with B. The mean BCLC stage was 0 or A in 126 (42.6%) patients. The mean tumor size was 5.5 cm, and the presence of cirrhosis was confirmed by pathological histology in 196 (66.2%) patients, with higher AFP levels (p < 0.001), higher PLT levels (p = 0.026) and more patients with BCLC stage 0 or A (p = 0.005) in the antiviral treatment group compared with the non-antiviral group.
To reduce the impact of potential confounders between the two groups on OS and RFS comparisons, we performed propensity score matching, and among the 99 matched pairs of patients, the baseline characteristics of the antiviral and non-antiviral groups did not show significant differences and were considered to have achieved covariate balance (Table 2).
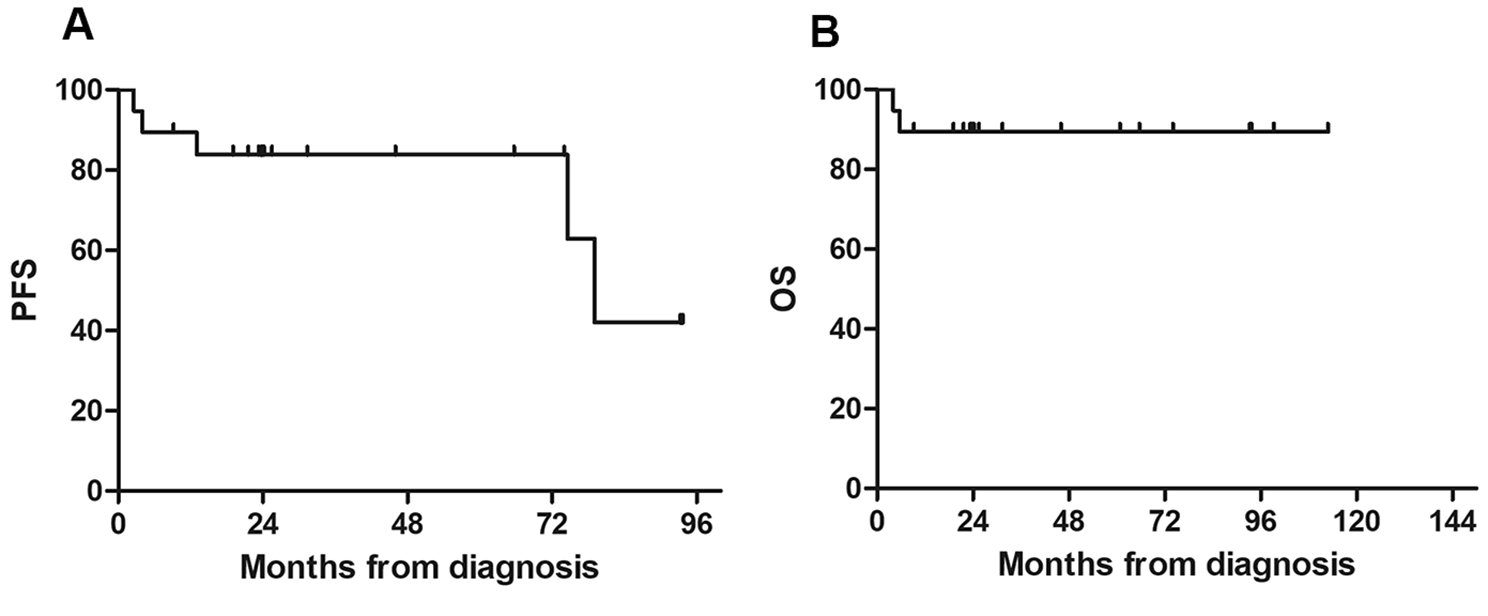
1 Baseline characteristics and clinical data Table 2 Baseline characteristics of the study patients after the 1:1 propensity score analysis Predictors of OS and RFSThe median follow-up time of patients was 54 months,174 (58.8%) patients developed tumor recurrence during the follow-up period, of which 95 (54.6%) had early recurrence, 79 (45.4%) had late recurrence, and 135 (45.6%) patients died.In the whole cohort, OS and RFS were significantly prolonged in the antiviral group compared to the non-antiviral group. The 1-, 3-, and 5-year OS was 94.9%, 80.3%, 63.7% and 86.3%, 62.6%, 48.2% in the antiviral and non-antiviral groups, respectively, p = 0.001, and the corresponding 1-, 3-, and 5-year RFS was 80.9%, 63.1%, 49.7% and 67.6%, 42.8%, 35.7% in the two groups, respectively, p = 0.001. In 198 patients (99 in the antiviral group and 99 in the non-antiviral group) after PSM, 67 (33.8%) experienced relapse (23 in the antiviral group and 44 in the non-antiviral group) and 88 (44.4%) experienced death (35 in the antiviral group and 53 in the non-antiviral group). There were significant differences in OS and RFS between the two groups, with the 1-, 3-, and 5-year OS was 94.9%, 80.8%, 66.5% and 90.9%, 64.6%, 49.4%, respectively, p = 0.009, and the corresponding 1-, 3-, and 5-year RFS was 81.8%, 76.8%, 76.8% and 67.7%, 55.6%, 55.6%, respectively, p = 0.001 for the two groups (Fig. 1A).
Fig. 1
Comparison of overall survival (A) and recurrence-free survivals (B) between the two groups in the entire cohort and in the propensity score-matched cohort the overall survival (C) and recurrence-free survivals (D) between the two groups
To identify factors associated with the impact on OS and RFS in patients after hepatectomy for HBV-related HCC, we performed univariate and multivariate COX regression analyses on the entire cohort and included parameters that had a significant impact on outcome in the univariate analysis in the multivariate analysis. Methemoglobin levels ≥ 20 ng/ml (HR, 2.227; 95% CI 1.513–3.278; p < 0.001), low to moderate tumor differentiation (HR, 1.625; 95% CI 1.150–2.297; p = 0.006), tumor size > 5 cm (HR, 2.237; 95% CI 1.130–4.429; p = 0.021), and tumor multiplicity (HR, 2.021; 95% CI 1.265–3.228; p = 0.003) were independent risk factors associated with OS. Independent risk factors affecting RFS included methemoglobin level ≥ 20 ng/ml (HR, 2.124; 95% CI 1.506–2.995; p < 0.001), alkaline phosphatase level > 130 IU/L (HR, 1.820; 95% CI 1.302–2.545; p < 0.001), tumor hypomedifferentiation (HR 1.462; 95% CI 1.067–2.002; p = 0.018), and tumor multiplicity (HR, 1.815; 95% CI 1.170–2.815; p = 0.008). Antiviral therapy was an independent prognostic factor not only for improving overall survival (HR, 0.500; 95% CI 0.343–0.728; p < 0.001) but also for RFS (HR, 0.529; 95% CI 0.377–0.741; p < 0.001) (Tables 3, 4).
Table 3 Univariate and multivariate analysis of overal survival Table 4 Univariate and multivariate analysis of recurrence-free survival Early and late recurrence of HCCOf the 296 patients included in the study, 95 patients (37 in the antiviral group and 58 in the non-antiviral group) developed early tumor recurrence within 2 years after undergoing curative hepatectomy, with prothrombin time ≥ 13 s (HR, 1.954; 95% CI 1.193–3.200; p = 0.008), methemoglobin level ≥ 20 ng /ml (HR, 2.498; 95% CI 1.538–4.057; p < 0.001), platelet count ≥ 100 × 109/L (HR, 1.756; 95% CI 1.087–2.838; p = 0.021), tumor size > 5 cm (HR, 3.035; 95% CI 1.310–7.034; p = 0.010), and tumor multiplicity (HR, 1.903; 95% CI 1.095–3.307; p = 0.023) were risk factors significantly associated with early hepatocellular carcinoma recurrence, while antiviral therapy was an independent protective factor for early recurrence (HR, 0.431; 95% CI 0.274–0.679; p < 0.001). Factors associated with late relapse were analyzed in 201 patients who did not develop relapse within 2 years, of whom 79 (45 in the antiviral group and 34 in the non-antiviral group) developed late relapse, and in a multifactorial analysis, AST levels > 40 IU/ml, ALP levels > 130 IU/L, and the presence of satellite nodules were independent risk factors associated with late relapse, while antiviral therapy was associated with late relapse was not associated with low risk of relapse (HR, 0.822; 95% CI 0.526–1.284; p = 0.389) (Tables 5, 6).
Table 5 Univariate and multivariate analyses for early recurrence of hepatocellular carcinoma in patients who underwent hepatic resection Table 6 Univariate and multivariate analyses for late recurrence of hepatocellular carcinoma in patients who underwent hepatic resection Cirrhosis and HBeAg subgroup analysisPatients in both groups who received antiviral therapy or not were stratified according to cirrhosis and HBeAg levels, and the results showed that the 1-, 3-, and 5-year RFS were significantly better in the antiviral group than in the non-antiviral group, with or without cirrhosis (p = 0.024, p = 0.024), and in the HBeAg-positive group, the 1-, 3-, and 5-year RFS in the antiviral group were not significantly different from those in the non-antiviral group (p = 0.352), while in the HBeAg-negative group, the 1-, 3-, and 5-year RFS was significantly longer in the antiviral group than in the non-antiviral group (p = 0.002) (Fig. 2).
Fig. 2
Kaplan-Meier plots of recurrence-free survival for antiviral versus non-antiviral. Patients with absence of cirrhosis (A) and presence of cirrhosis (B). Patients with absence of HBeAg (C) and presence of HBeAg (D)
留言 (0)