
記住我


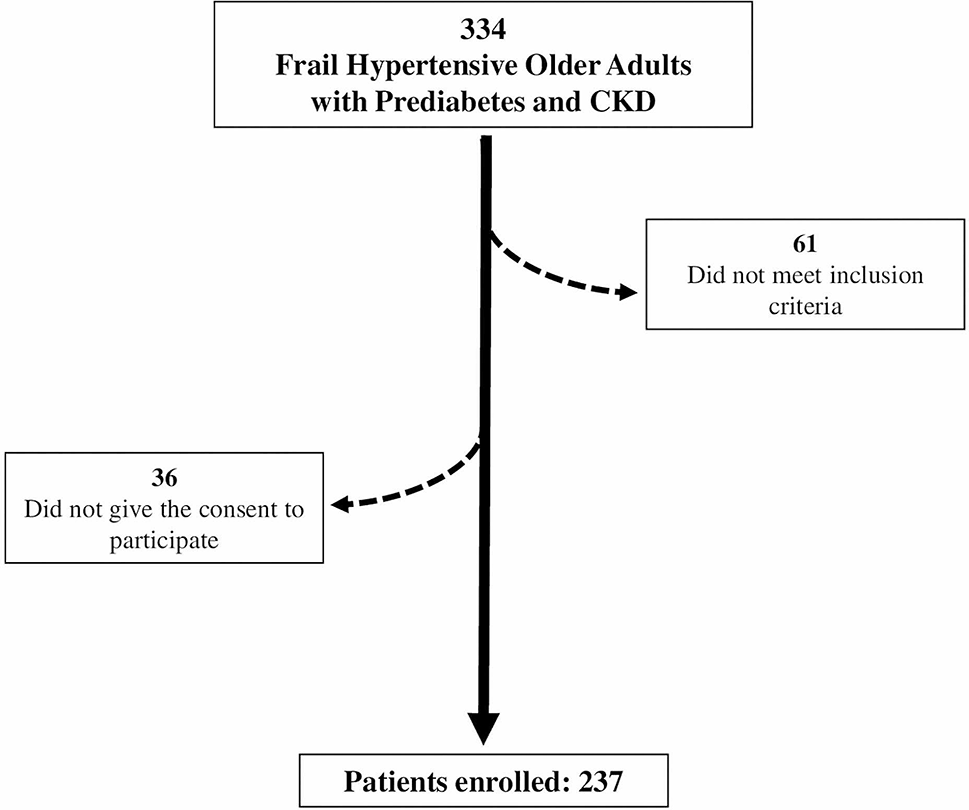
This retrospective and the observational study included 6691 consecutive patients who underwent CABG using BITA in a single large tertiary center from January 2001 to December 2017. Patients younger than 18 years (n = 14), with missing angiographical data (n = 40), who underwent CABG other than BITA grafts (n = 1916), on-pump CABG (n = 781), concomitant heart surgery (n = 456), and had previous CABG history (n = 89) were excluded (Fig. 1). Patients were divided into two groups, the non-DM and DM groups. Patients in the DM group were divided into two subgroups, namely, the well-controlled (preoperative HbA1c of < 7%) and poorly controlled DM groups (HbA1c of ≥ 7%) [12].
Fig. 1
Study flow diagram. A total of 3395 patients who underwent OPCAB with a bilateral internal thoracic artery in a single tertiary center were enrolled. Patients were divided into non-DM and DM groups. Patients in the DM group were divided into well-controlled (HbA1c < 7%) and poorly controlled DM groups (HbA1c ≥ 7%). OPCAB indicates off-pump coronary artery bypass graft; DM: diabetes mellitus; HbA1c: hemoglobin A1c
The Institutional Review Board of Samsung Medical Center approved this study (SMC 2021-11-157, date of approval: December 1, 2021), which waived informed consent from individual patients because this retrospective study poses minimal risk for patients.
Data collection and clinical follow-upThe baseline demographic, echocardiographic, laboratory, and follow-up clinical outcomes were retrospectively collected through medical record review. Extracted data were revalidated by our research coordinators and physicians for clarity.
The primary endpoint was cardiac death at 10 years postoperative and the secondary endpoints included MI, revascularization, graft failure, stroke, postoperative wound infection, and major adverse cardiovascular events (MACE; a composite endpoint of cardiac death, MI, and revascularization). The mean clinical outcome follow-up duration was 4.01 years. The mortality data for patients who were lost to follow-up were confirmed using the National Death Records. MI was defined as elevated cardiac troponin or myocardial band fraction of creatine kinase that is greater than the upper reference limit with concomitant ischemic symptoms or electrocardiography findings indicative of ischemia. Left ventricular dysfunction was classified as follow: normal (left ventricular ejection fraction more than 50%); mild dysfunction (left ventricular ejection fraction 40% to 49%); ≥ moderate dysfunction (left ventricular ejection fraction less than 40%). Graft patency was assessed using coronary computed tomography angiography or invasive coronary angiography, according to operator discretion (Additional file 1: Table S1). Grafts were evaluated following the FitzGibbon A, B, and O classification and interpreted by an independent cardiology expert who was blinded to treatment strategy. Postoperative early clinical outcomes included clinical outcomes within 30 days of the surgery. Outcome variables were defined according to the definition of the Society of Thoracic Surgeons Adult Cardiac Surgery Database version 4.20 [13].
Surgical procedure and perioperative managementThe surgical technique for OPCAB was performed following relevant standard guidelines [1, 14]. and described in our earlier report in detail [15]. BITA was prepared using the skeletonization technique. After opening the pericardium, the right ITA was anastomosed to the left side of the left ITA as a Y-composite graft. Achieving complete revascularization of all vessels with a 1-mm or larger diameter and 50% or more angiographic diameter stenosis was intended in all patients. The left ITA was first anastomosed to the left anterior descending artery and its branches, and the right ITA was sequentially anastomosed to branches of the circumflex artery. The right coronary territory was revascularized last. The quality of the anastomosis was assessed by transit-time flow measurement with a Transsonic Flowmeter (Transonic Systems, Ithaca, NY).
Strict glycemic control before, during, and after the surgery has been implemented under standard institutional protocols. Target blood glucose control in patients with DM was set to < 180 mg/dL [12, 16] by intermittent regular insulin injection (Humulin; Eli Lilly and Company, Indianapolis, Ind) intraoperatively and continuous regular insulin infusion postoperatively in the intensive care unit (ICU). Blood glucose level was measured every 1 h in the operative room and every 4 h in the ICU. If the ideal glycemic control was not made, glucose concentration was checked at an interval of 2 h until the target level was achieved in the ICU.
Guideline-directed medical therapy including a combination of antiplatelet agents, beta-blockers, statins, and angiotensin-converting enzyme (ACE) inhibitors and/or angiotensin receptor blockers (ARBs) was applied to all patients undergoing CABG, unless contraindicated [1, 17].
Statistical analysisDescriptive statistics for categorical variables were reported as frequency and percentage, whereas continuous variables were reported as mean ± standard deviation or median (range). Categorical variables were compared between the groups using the χ2 test or Fisher’s exact test, whereas continuous variables were compared using the two-sample t-tests or the Wilcoxon rank-sum test. Continuous data were checked for distribution normality using the Shapiro–Wilk test and graphical methods. The cumulative incidence of clinical events is estimated using a Fine–Gray model to account for the competing risk of death from non-cardiovascular causes.
Multiple sensitivity analyses, including multivariable Cox proportional hazard regression and propensity-score matched analyses, were performed to reduce biased effects. The Cox proportional hazard regression model considered variables that were significant in the univariable analysis or clinically relevant in the multivariable analysis. Variables included age, sex, body mass index, DM, HbA1c, an initial diagnosis of ischemic heart disease, hypertension, dyslipidemia, smoking history, end-stage renal disease requiring dialysis, previous cerebrovascular accident, abdominal aortic aneurysm, peripheral arterial disease, chronic obstructive pulmonary disease, peak troponin I, peak creatine kinase-MB, glomerular filtration rate, ejection fraction, left ventricular dysfunction, 3 vessel disease, left main involvement, and urgent surgery. The backward elimination method was used for model selection in the multivariable analysis. The results were reported as hazard ratio (HR) and 95% confidence interval (CI).
Propensity-score analyses were used to adjust covariate differences between the two groups. The variables included in the propensity-score model were as follows: age, sex, body mass index, angina, hypertension, dyslipidemia, previous stroke history, chronic kidney disease, chronic obstructive pulmonary disease, smoking history, left ventricular dysfunction, preoperative significant mitral valve regurgitation, urgent surgery, the number of anastomoses, and the number of diseased coronary arteries. A total of 1393 patients in the non-DM group and 1393 patients in the DM group were matched in a 1:1 manner using nearest-neighbor matching. Additionally, for subgroup analysis, a total of 452 patients in the well-controlled DM group and 452 patients in the poorly controlled DM group were matched in a 1:1 manner using nearest-neighbor matching. The balance between the two groups after propensity-score matching was assessed by calculating the standardized mean difference (SMD) between selected variables, with an SMD of < 0.20 suggesting an appropriate balance (Additional file 2: Fig. S1, Additional file 1: Tables S2 and S3).
All statistical tests were two-sided, with an alpha level of 0.05. Statistical analysis was performed using Statistical Package for the Social Sciences software (version 25.0, SPSS, Chicago, IL, USA) and R statistical software (version 4.0.2; R Foundation of Statistical Computing, Vienna, Austria).
留言 (0)