
記住我




A 21-year-old woman underwent bilateral SmartSurf ACE for correction of myopia and astigmatism. She had no history of clinical herpetic infection, active eye disease, or systemic disease. Preoperative refraction was -6.25/-0.75 × 30 in the right eye and -6.00/-1.25 × 158 in the left eye. Uncorrected visual acuity (UCVA) was 20/500, and best spectacle-corrected visual acuity (BSCVA) was 20/20 in both eyes. Slit-lamp examination was normal. Pachymetry readings were 572 mm in the both eyes. Corneal topography (Pentacam, Oculus) showed regular maps with simulated keratometry (SimK) readings of 41.16/42.19 @ 7 in the right eye and 41.22/42.43 @ 175 in the left eye.
The surgery was assisted by the Amaris 500 excimer laser. The epithelial thickness was set to 55 μm in the center and 65 μm in the periphery in the 6.5 mm diameter range. After laser ablation, a bandage contact lens was applied. The patient was treated with Levofloxacin eye drops, prednisolone acetate ophthalmic suspension, pranoprofen eye drops and 0.3% sodium hyaluronate drops.
One week after SmartSurf ACE, the patient reported no discomfort. UCVA was 20/25 in both eyes. After the corneal epithelium became normal, we removed the bandage contact lens, and prescribed fluorometholone eye drops 4 times per day and 0.3% sodium hyaluronate drops every 2 h.
On the tenth postoperative day, the patient had symptoms of stinging pain and foreign body sensation. Although UCVA was still 20/25, mild superficial punctate keratitis occurred in both eyes. Deproteinized calf blood extract eye drops and eye gel were used to reconstruct corneal surface.
After three days of treatment, vision was reduced in both eyes. UCVA was decreased to 20/40. Cornea epithelial defect and superficial spotted hazes were observed in both eyes. The patient was initially treated for 1 week with fluorometholone eye drops, 0.3% sodium hyaluronate drops, deproteinized calf blood extract eye drops, deproteinized calf blood extract eye gel, and wore a bandage contact lens again.
On the 24th postoperative day, pain, photophobia, tearing, and reduced vision appeared in her eyes, which lasted 1 day. Three nummular sub-epithelial infiltrates were presented on the cornea in the right eye. A dendritic corneal ulcer appeared in the left eye (Fig. 1). Fluorescein staining was both positive. A retrospective detailed history revealed that the patient was accustomed to staying up late, lived with poor sanitation, and suffered from mental stress due to school pressures, which led to decreased immunity and catching a cold two weeks after surgery. Further, postoperative topical corticosteroid was used in both eyes. HSK was considered, and we decided on hospitalization for the patient. With removal of the contact lens and cessation of flumirone eye drops, the patient was treated with oral valaciclovir 300 mg tablets 2 times per day, ganciclovir eye drops, and 0.3% sodium hyaluronate drops every 2 h, ganciclovir eye gel 2 times per day, tacrolimus eye drops 4 times per day, and deproteinized calf blood extract eye gel once before bedtime.
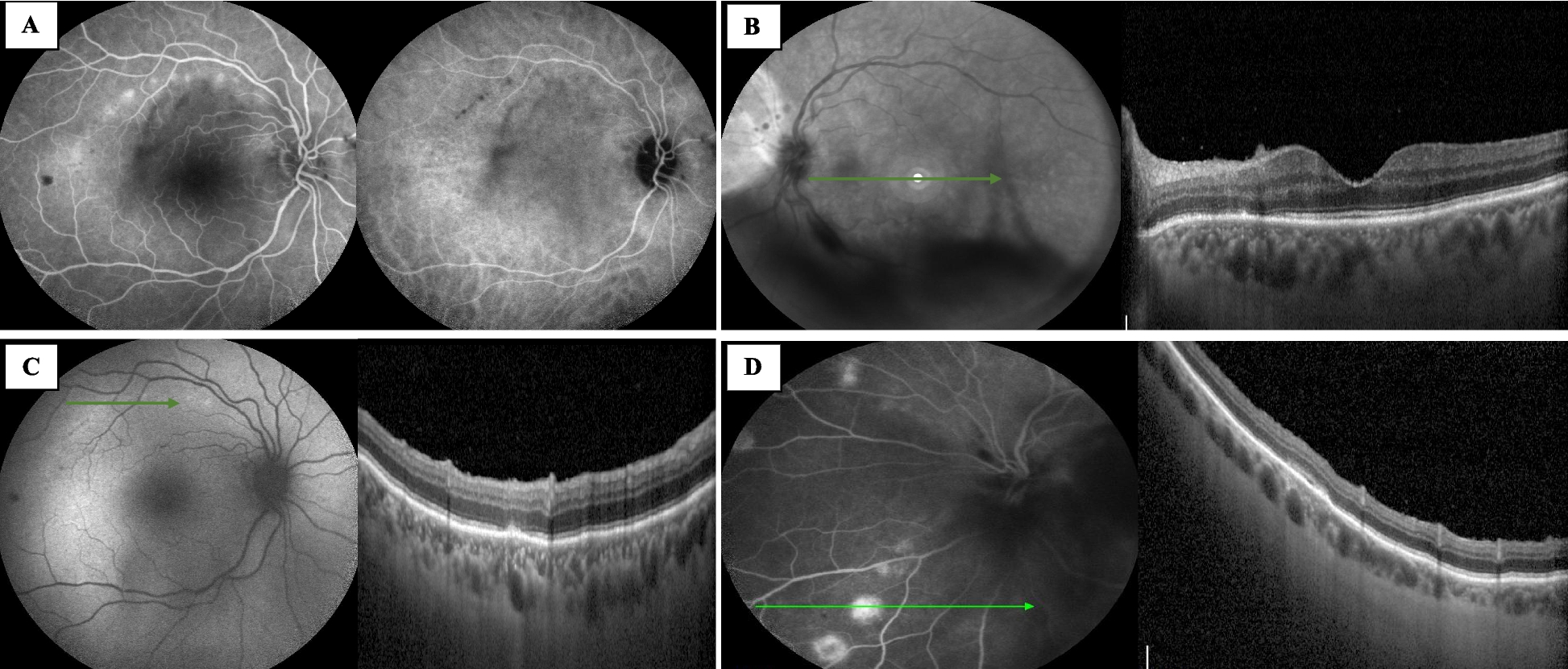
Fig. 1
Slit-lamp examination and in vivo confocal microscopy of two eyes performed on the 24th postoperative day. A Three nummular sub-epithelial infiltrates were presented on the cornea in the right eye. B A dendritic corneal ulcer appeared in the left eye. C-D In vivo confocal microscopy showed corneal epithelial edema and anterior stromal edema in the right eyes. E–F Decreased sub basal corneal nerve density, infiltration of inflammatory cells in corneal stroma were observed in the left eye
In vivo confocal microscopy revealed corneal epithelial edema and anterior stromal edema in both eyes. Decreased sub basal corneal nerve density, infiltration of inflammatory cells, and Langerhans cells in the corneal stroma were observed in the left eye. No abnormal changes were observed in the corneal endothelium or amoeba infection in either eye (Fig. 1).
After two days of hospitalization, the patient complained of reduced irritation. The corneal epithelial defect had decreased in size. Because slow improvement was observed, HSK was not suspected. One week later, the dendritic corneal ulcer had become mild and the staining range of fluorescein staining was reduced.
On the ninth day of hospitalization, the patient reported no discomfort. UCVA had improved to 20/20 and 20/25. Corneal fluorescein staining was negative with complete resolution of the corneal edema. The lesion healed with only mild corneal macula remaining in the right eye. The dendritic corneal ulcer healed and replaced by a fibrotic stromal scarring the left eye. As the disease activity completely subsided, the patient was discharged from hospital and maintained on valaciclovir 300 mg tablets 2 times per day for 2 weeks; flumirone eye drops every 2 h, tapering gradually, ganciclovir eye drops and 0.3% sodium hyaluronate drops 4 times per day, and ganciclovir eye gel once before bedtime.
At the 9-month follow-up, HSK had not recurred, and only a minimal haze at the corneal interface was seen. UCVA was 20/22 and 20/33, while BSCVA was 20/20 in both eyes. The patient was advised to continue with regular review.
留言 (0)