Up to date, the mechanisms influencing the vault can be divided to those associated to the anatomic features of the eye [2, 6, 8, 9, 19,20,21,22], the landing position of the ICL [10] and those related to ICL physical parameters [9, 23, 24]. This later group comprises the ICL dioptric power [9, 23] and the ICL size [9, 24]. Another factor, with potential influence on the vault is the optical geometry of the ICL, i.e. whether the ICL is spherical or toric [12,13,14,15]. In the present study, sICL and tICL showed no difference in vault, and the associations of the vault with anatomical and ICL-related parameters were similar for both ICL types. Also, the refractive outcomes showed good predictability and effectiveness of ICL in correcting a wide range of myopia and moderate levels of astigmatism.
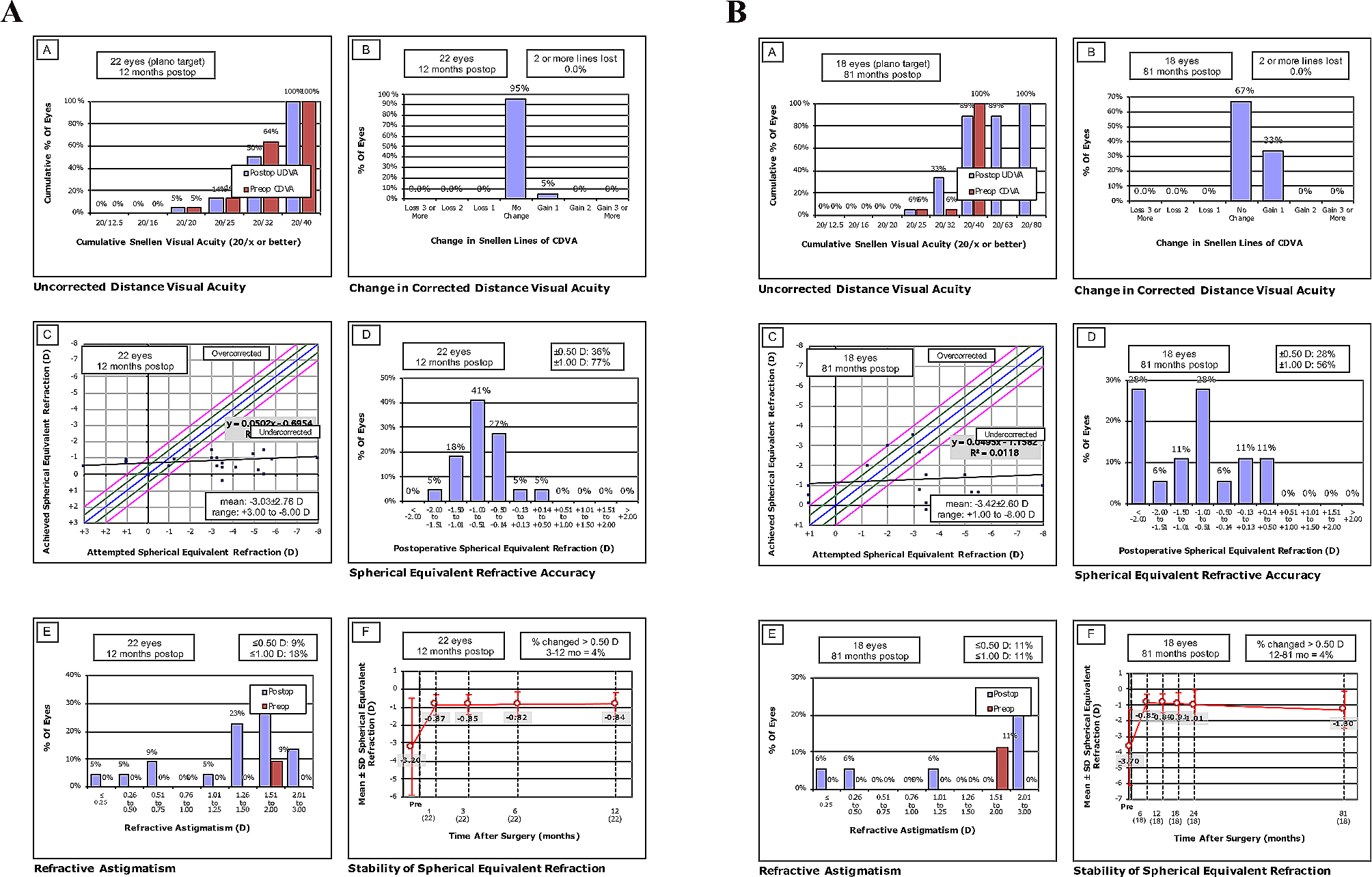
The results point towards a good predictability of sICL and tICL surgery, respectively with 66% and 83% of the eyes presenting a postoperative SE within ± 0.50 D; 93% and 95% showed a postoperative SE within ± 1.00 D. Additionally, the tICL group showed a higher percentage of eyes with lower levels (≤ 0.50 D) of postoperative astigmatism 63.4% compared to 48.8% in the sICL group. This contributed to an improvement of one or more VA lines in 34% and 54%, respectively in the eyes implanted with sICL and tICL resulting in a higher efficacy of the tICL. Garcia del la Rosa et al. in a group of patients implanted with sICL and tICL (ICL-V4b) reported at 12-months follow-up a SE within ± 0.50 D in 85% of the eyes, with approximately 45% of the eyes improving one or more VA lines [25]. Niu et al. reported in a group of high myopes (preoperative SE:-14.00 D) implanted with sICL and tICL, a postoperative SE within ± 0.50D in 73% of the eyes and within ± 1.00 D in 80%, however some of their eyes had myopia above the ICL correction limit which increases the postoperative SE [26]. Moshirfar et al. reported at 3-months follow-up in a group of eyes implanted with tICL a postoperative SE within ± 0.50D in 77% of the eyes and a reduction in refractive astigmatism from 2.67 D to 0.68 D, which concurs with the present study [27]. Zhao et al. in a prospective study of patients bilaterally implanted with sICL and tICL reported a postoperative SE within ± 0.50 D in 94% and 88% of the eyes implanted with sICL and tICL, respectively, representing lower levels of postoperative refractive error compared to the present findings [15]. The higher refractive predictability in Zhao’s study may be related to the cylinder power threshold used for tICL implantation (present study: 1.25 D; Zhao et al.: 0.75 D). This resulted in 40% (n = 17) of the eyes with postoperative astigmatism ≥ 0.75 D compared to none in Zhao’s et al. study. These outcomes point towards the importance of considering tICL in the correction of low refractive astigmatism, since it influences the visual performance [28] and the subjective quality of vision [29].
Regarding the vault differences between the two ICL types, there was no clinically significant inter-eye difference (sICL-tICL: -1.5 ± 143.4 µm). Also, both ICLs geometries showed similar relationships between vault magnitude and anatomical or ICL-related parameters. The present results do not show evidence of tICL parameters such as the cylinder magnitude or vectorial components on the vault, as observed by correlation analysis in Fig. 3 M–O. This evidence is corroborated when the association of all the independent parameters studied with the vault is investigated by merging the sICL and tICL groups though the GEE. This finding contrasts with a recent study using a similar inter-eye analysis [15]. Zhao et al. reported an average tICL vault 110 µm higher than the produced by sICL, with the cylinder power being the contributing factor for the difference in the vault between the two ICL geometries. Their estimated ICL cylinder contribution corresponded to an increase of 78 µm in vault per dioptre of cylinder. Previous studies using the ICL-V4b model reported smaller differences between sICL and tICL, 90 µm [12] and 45 µm [13] when the two types of ICL were implanted in different groups of patients. Alfonso et al. stated that the difference in vault was associated to the toricity in the posterior surface of the ICL, thus the lower radius of curvature necessary to produce the cylinder component increased the sagittal depth in the optic zone [13]. Alternatively, Lege et al. suggested that differences in the intraocular behaviour between sICL and tICL during accommodation were related to the higher rigidity of the tICL [14]. The ICL model used in this study (ICL-V4c) has the toric tailored on the anterior surface (STAAR Spain personal communication), presumably as a convex surface (positive cylinder). Thus, the hypothetical influence of tICL geometry on the vault may be attributed to differences in the ICL thickness across the meridians, produced by the presence of meridional curvature variations in the ICL anterior surface, which in turn changes the mechanical properties of the ICL. However, the present results do not show significant influence of tICL geometry on the vault, suggesting that ICL geometry plays a minor role in vault magnitude.
As far as the main vault predictors are concerned, ICL size minus the ATA represents the most influential predictor, characterizing the level compression of the ICL due to its oversize. Using the ATA as a descriptor of the anterior chamber width, the GEE model predicted a variation of 387 µm in vault per millimetre of compression, with this prediction applicable to the two ICL geometries. The present finding concurs with Igarashi et al. results in the sense that the ICL size minus the ATA could be used as a single predictor of the vault, with a variation of 661 µm in vault per millimetre of compression [21]. Similar findings were reported by Sánchez-Trancón et al., with the vault variation comprised between 318 µm to 528 µm per millimetres of compression depending on the ICL size [9]. On the other hand, we did not find a significant association between vault and the compression calculated using the ICL size minus WTW. This result agrees with previous studies that found a weaker association between the vault and the compression calculated using the WTW compared to compression calculated using the ATA [9, 21] or using the sulcus-to-sulcus (STS) distance [5]. Accounting for this, is the fact that the ICL haptics rest on the ciliary-sulcus complex, thus the STS represents the most realistic measurement to calculate the ICL compression. The anterior chamber width (e.g. ATA) has been shown to have a stronger association with the STS compared to the WTW [30, 31]. These findings support the argument that the anterior chamber width can be used as an anatomical parameter for improving the ICL manufacturer’s sizing nomogram.
A second relevant vault predictor was the ICL spherical power. The GEE estimated an increment of about 20 µm in vault for every negative unit of spherical dioptre, which is in agreement with the SE association reported by Sánchez-Trancón et al. in a larger sample [9] and similar to the 27 µm reported by Hernandez-Matamoros [23]. This reflects the increase in the innate sagittal depth of an ICL, related to a more pronounced concave ICL posterior surface radius as the spherical power becomes more myopic. Lee et al. reported an innate vault variation of about 45 µm per dioptre for ICLs (model: ICM-V4) ranging from -3.0 to -23.0 D [5]. Thus, when estimating the vault of an ICL the spherical power should be considered since more myopic ICLs tend to originate higher vaults whereas, less myopic ICL produce lower vaults. For the tICL the sphere component (with the cylinder in positive form) should be considered since the intrinsic vault of the ICL depends on the spherical power of the most negative meridian.
A third vault predictor was the ICL thickness, with the GEE predicting an increase of about 2.8 µm in the vault per one µm of increase in the ICL central thickness. Considering the full range of thicknesses measured (~ 100 µm) the maximum vault difference estimated would be 280 µm. A possible explanation for the thickness influence on the vault is that thicker ICLs are stiffer and be less likely to be influenced by the iris compression forces. Regarding the two ICL geometries, the central thickness in the sICL and tIC were proximal and both had similar relationships with the vault. The fact that the central ICL thickness could not be associated to any other ICL-related parameter, for instance ICL sphere (sICL: R = 0.08 p = 0.631; tICL: R = -0.18, p = 0.270, data not shown) limits the use of ICL central thickness as a predictor of the vault. Considering the peripheral ICL thickness may result in a better vault predictor, as the ICL peripheral thickness increases with spherical power while the central thickness tends to remain constant [32]. Future studies are required for detailing the variation of the ICL thickness in the central and peripheral parts of the ICL and study its influence on the vault. Meanwhile, the theoretical assumptions that more myopic ICLs have thicker peripheral parts and tICL with higher cylinders have thicker central parts, may guide in understanding the effect of ICL thickness on the vault.
Other parameters representative of additional mechanism regulating the vault such as the CLR [7,8,9, 22, 24, 33], age [9, 19], ICL size [9, 24] and pupil size [32, 34,35,36] failed to show statistical significance in the GEE model. In the bivariate analysis, patient age showed some degree of association (negative) with the vault, which can be attributed to two age-related factors, the increase in crystalline lens anterior protrusion (CLR) [22] and the decrease in pupil diameter [37]. The former reduces the vault created by the ICL compression and its intrinsic vault, and the later increases the anterior–posterior pressure produced by the iris placing the ICL closer to the crystalline. The vault showed a negative association with the CLR for both ICL modalities, indicating that crystalline lens morphology plays a role in vault magnitude [8, 33] however the correlations did not reach statistical significance. Gonzalez-Lopez et al. reported that eyes with high vault (> 750 µm) had an average CLR of + 73 µm whereas eyes presenting low vault (< 100 µm) had an average CLR of + 350 µm [22]. Cerpa et al. further suggested that eyes with CLR > + 150 µm were at risk of presenting low vault (< 250 µm) [24]. Larger ICLs, especially the 13.7 mm size had been associated with higher vaults [24], potentially due to a higher effect of the compression forces on the ICL [9]. In the present study, the limited number of eyes implanted with 12.6 and 13.7 mm ICLs may have restricted the ability for detecting the influence of ICL size on the vault. Nonetheless, the inter-eye comparisons showed no statistical and no clinical difference (repeatability for vault measurement ∼60 µm [38]) between sICL and tICL, with the inter-eye differences similar to those observed in fellow eyes implanted with the same ICL geometry [16]. The current results allow us advancing that the vault prediction for an ICL size is independent of the ICL optical geometry.
Postoperative pupil size and vault showed tenuous positive relationships similar for both ICL geometries, i.e. eyes with larger pupils tended to present higher vaults. A recent study by Gonzalez-Lopez et al. using well controlled lightning conditions showed that the postoperative pupil size remained barely unchanged (slightly larger postoperatively ∼0.11 mm) compared to the preoperative pupil size [39]. Therefore, considering a clinically stable pupil size pre- and post-surgery, the association between vault and postoperative pupil size may be explained by the effect anterior–posterior pressure induced by the iris on the ICL.
This study has some limitations. One of them is its retrospective nature, since a previous protocoled study minimises the occurrence of errors and bias. To counteract the occurrence of errors, all AS-OCT were reassessed by redoing the measurements by a proficient operator, unaware of the ICL implanted. Second, there was lack of a planned randomization process as the first operated eye was always the right eye. In our sample 22 eyes were first implanted with sICL and 19 with tICL, representing a good balance between type of ICL initially implanted. A third limitation regards to the sample size as the GEE sees its performance limited for samples lower than 50 individuals [40]. Additionaly, the number of analysed eyes may have limited the detection of factors known to play a role on the vault magnitude; however the study aimed and was designed to detect the influence of ICL optical geometry on the vault using a matched-pairs design. The associations observed between vault and the independent factors were very consistent in the two ICL groups and unlikely to change significantly for larger sample.







留言 (0)