
記住我

Despite advances in surgical technique and postoperative care, pneumonectomy is still associated with high mortality and morbidity. Therefore, patients who are candidates for pneumonectomy should be evaluated in detail for their suitability for bronchovascular sleeve resection and the lung parenchyma should be spared as much as possible. In our series, the rate of pneumonectomy in all anatomic lung resections was %16.1. This rate is between %4.5 and %33 in various publications [8,9,10].
Bronchopleural fistula is one of the most severe complications seen after lung resections and is reported to be in the range of 4.5–20% after pneumonectomy. It is associated with increased mortality and morbidity, prolonged hospitalization, and higher costs. Various risk factors have been described for the development of BPF like; right-sided pneumonectomy, excessive dissection of the peribronchial structures, long bronchial stump, preoperative radiotherapy, positive sputum culture, low serum albumin level, and male gender [1,2,3]. In our study, in accordance with the literature, the rate of BPF was found to be higher in patients who underwent right pneumonectomy compared to the left.
Interestingly, the presence of reoperation was found to be associated with an increased postoperative BPF rate in univariate analyzes in our study (p = 0.043). A total of 10 patients underwent reoperation due to postoperative hemorrhage, and 3 of these patients developed BPF. We do not have enough data to reveal the relationship between reoperation and the risk of postoperative BPF. However, excessive blood transfusion, hypovolemia, prolonged intubation, and physiological stress caused by reoperation can be considered possible risk factors.
The difficult and time-consuming nature of BPF treatment has increased the importance of methods to prevent this complication. For this purpose, various methods of bronchial reinforcement have been described in the literature. Omentum, azygos vein, pericardium, a pedicled pericardial fat pad, intercostal muscle, pleura, and diaphragm have been used to increase the vascularity of the bronchial stump. Despite the variety of tissues that can be used, the issue of which method is the best is controversial [6, 11].
The use of a pedicled intercostal muscle flap is reported to have the potential risk of the development of heterotopic ossification leading to necrosis of the flap. Coverage of the bronchial stump with the pedicled pericardial flap requires to make a pericardiotomy and reconstruction of the pericardium. The omental flap is one of the most effective techniques for the prevention of bronchial fistula, but it requires an additional incision into the abdomen and diaphragm [12, 13].
The pericardial fat pad is another useful tissue for bronchial stump coverage. It was also shown that various angiogenic and growth factors are produced from the pericardial fat pad and help the healing of the bronchial stump [10, 14, 15]. However, in some patients, the volume and vascularization of this tissue flap are insufficient. Thus, we preferred to use the TPFF as a well-vascularized, voluminous tissue flap to cover the bronchial stump. The usage of the pedicled thymus flap for protection of the bronchial stump or bypass graft was described before and considered as a safe and effective alternative to the other tissue flaps. Ohtsuka et al. [16] have applied a thymopericardial fat flap (also called a pedicled prepericardial fat flap) to reinforce the vascular graft in 245 cases who underwent coronary artery bypass graft surgery. In another study, Wurts et al. [17] used TPFF in 5 patients with tracheal reconstruction and they called this flap the “thoracic omentum”, referring to the efficacy and usefulness of the omental flap.
In this study, we applied TPFF in 53 patients with pneumonectomy, and no postoperative BPF was detected. In univariate analyses, the BPF rate was significantly lower in patients who underwent bronchial coverage with TPFF (p = 0.044).
However, in multivariate analysis, none of the variables included in the modeling reached statistical significance (Table 3).
For thoracic surgeons with thymectomy experience, dissecting the ipsilateral thymus lobe and including it in the pericardial fatty tissue flap is not a challenging procedure. Moreover, TPFF coverage could be easily performed also via the VATS technique. Video thoracoscopy facilitates the detection and control of minor hemorrhages by providing better exposure in the anterior mediastinum. We performed VATS pneumonectomy in 20 patients and TPFF coverage was applied in 12 of them.
Although the mean operative time was found to be slightly increased in patients who underwent TPFF coverage, this difference was not statistically significant (p = 0.101). After a certain adaptation period, the preparation of the thymopericardial flap and its suturing to the bronchial stump can be performed in as little as 15 min.
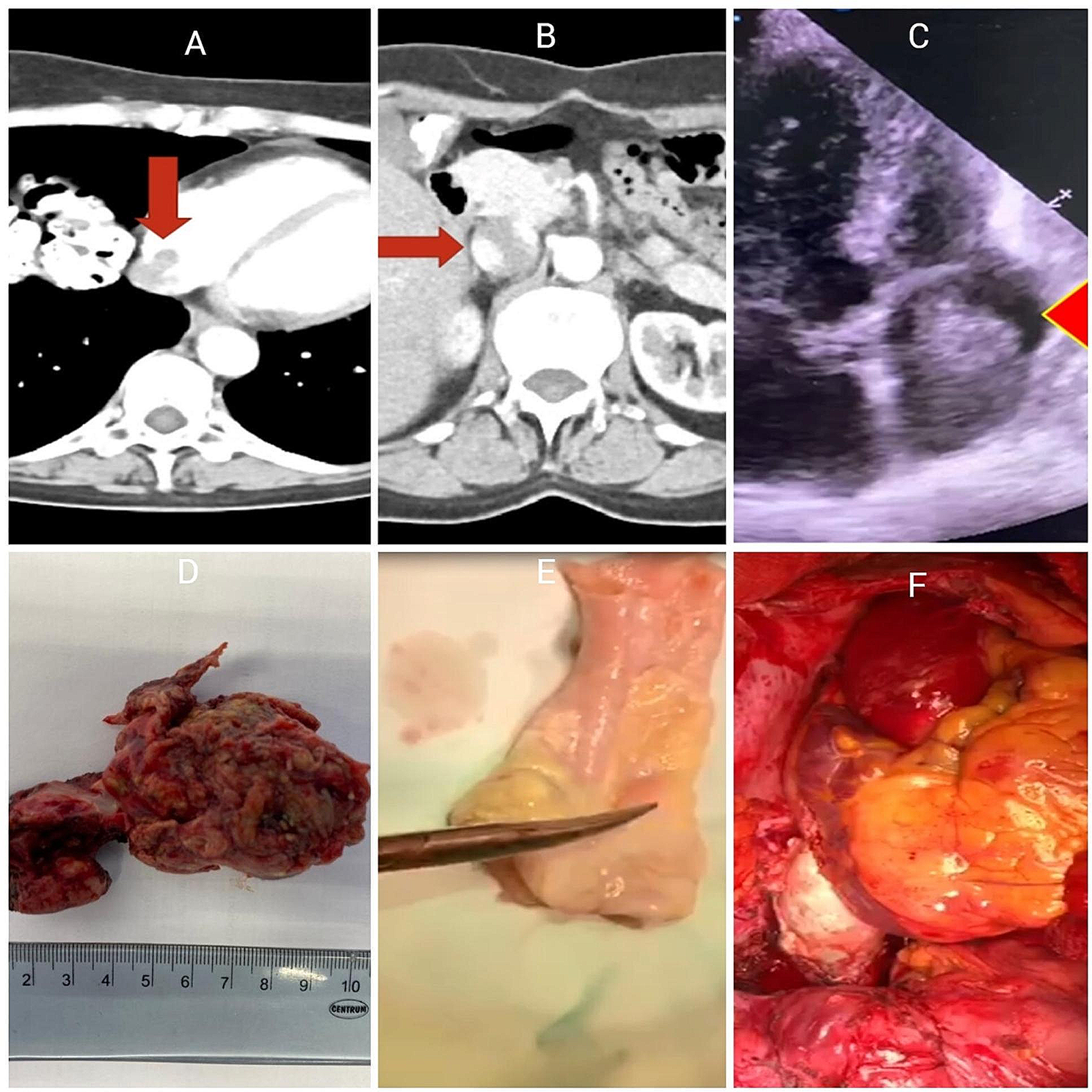
Interestingly, we detected the pedicled tissue flap around the bronchial stump could be in thorax CT even after 6–12 months in patients who underwent TPFF coverage (Fig. 3). Nagashima et al. [18] examined the postoperative change of free pericardial fat pad affixed to the bronchial stump and found a significant reduction in the volume of adipose tissue at the end of 6 months. Considering that bronchopleural fistula may occur in some patients in the very late period, we think that it would be more appropriate to use pedicle flaps instead of free harvested tissue.
Fig. 3
TPFF could be seen in thorax CT even after 6–12 months after operation (asterisks)
This study had some limitations. Because of its retrospective nature, bias regarding patient selection existed. Although there was a tendency to apply TPFF in those with a high risk of BPF the criteria for usage of a TPFF were not defined clearly. One of the reasons for this is that while the TPFF application was initially decided on a patient-specific basis, it later became a routine procedure. Furthermore, to demonstrate the efficacy and superiority of the TPFF, it is necessary to compare it with other coverage methods, especially via large-scale prospective studies.
留言 (0)