
記住我

Cervical dystonia, also known as spasmodic torticollis, is characterized by sustained involuntary contractions of cervical muscles that cause abnormal postures of the head and neck. Idiopathic cervical dystonia (ICD) develops without underlying neuromuscular disease and is predominantly of adult-onset. The prevalence of ICD is 1.18 to 30.4 cases per 100,000 population.1,2 The pathogenesis of ICD is unknown despite hypotheses such as genetic susceptibility and brain stem problems. The symptoms progress gradually and include involuntary head rotation, pulling sense, stiffness, or pain of the neck.3 Idiopathic cervical dystonia affects daily life activities and emotional moods, resulting in a poor quality of life.4
Although oral medications, manual therapy, stretching/exercise, physiotherapy, and deep brain stimulation surgery can be used for treatment of ICD, botulinum toxin (BTX) injection is the treatment of choice.3 Botulinum toxin, which is produced by Clostridium botulinum bacterium, blocks the secretion of acetylcholine to the neuromuscular junction. Muscles cannot receive nerve signals and no longer contract, becoming chemically paralyzed.5 Since onabotulinumtoxin A was approved by the US Food and Drug Administration in 1989, it has been used for several myotonic disorders.6 Botulinum toxin therapy improves symptoms and psychosocial function in ICD, increasing the quality of life and work productivity.7
A possible reason for the failure of BTX therapy in patients without other underlying diseases is the presence of neutralizing antibodies.8 The incidence of this event is fortunately low and can be prevented by using the minimum effective dose and having a sufficient injection interval. Another reason is insufficient dose or inadequate muscle targeting/selection.9 Correct injection requires a detailed understanding of muscle anatomy and modalities to accurately detect dystonic muscles. Electromyography (EMG) and contracted muscle palpation are usually used for muscle selection for BTX injection.10 However, there are opinions that routine needle EMG guidance for BTX injection has some disadvantages such as pain, equipment requirement, time-consuming process, and target misleading.11
With the increasing need for an alternative modality for muscle selection, 18F-FDG PET/CT began to be used for evaluation of ICD. Increased FDG uptake is noted in dystonic cervical muscles on PET/CT, and BTX injection can be performed in these identified muscles.12,13 It can be hypothesized that EMG is useful for muscles that are difficult to identify by physical examination and PET/CT is useful for muscles that are difficult to identify by EMG.14,15 However, it was unclear whether FDG PET/CT could predict the therapeutic outcomes and improve the BTX therapy response in patients with ICD.
Therefore, we investigated the therapeutic efficacy of FDG PET/CT-assisted BTX injection therapy and predictive PET findings related to a good response in patients with ICD.
PATIENTS AND METHODS SubjectsThis study was conducted with ICD patients who received onabotulinumtoxin A (Botox, Allergan, Dublin, Ireland) injection therapy. Idiopathic cervical dystonia was diagnosed on clinical examination by an experienced rehabilitation physician, with typical signs and symptoms in the absence of other neurologic disorders. A list of 222 patients who underwent FDG PET/CT with spasmodic torticollis from November 2007 to July 2018 was obtained and the following inclusion criteria were applied: (1) patients who underwent baseline FDG PET/CT before BTX injection; and (2) patients with both baseline Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) score and TWSTRS score at 4 weeks after BTX injection. The following patients were excluded: (1) patients with pure anterocollis or retrocollis; and (2) patients with BTX injection history within 16 weeks before PET/CT. A total of 78 final subjects was enrolled. This retrospective study was approved by the Institutional Review Board of Samsung Medical Center on February 15, 2022 (IRB file no. SMC 2022-01-188-001), and the need for informed consent was waived.
FDG PET/CTAll subjects underwent PET/CT examination with a dedicated PET/CT scanner (Discovery LS; GE Healthcare, Milwaukee, WI). Patients were instructed to fast for at least 6 hours and were injected with 5 MBq/kg of FDG. Blood sugar levels of all patients were below 200 mg/dL. Patients waited in a seated position and allowed their necks to turn spontaneously during the uptake time to improve sensitivity.14 After 60 minutes, a CT scan was performed (8-slice, 140 keV, 40–120 mA), and a PET scan from the skull base to the thigh was subsequently obtained (4 mm/frame, 2D mode). Image reconstruction was performed using an ordered subset expectation maximization algorithm (2 iterations, 28 subset, matrix size 128 × 128, voxel size 4.3 × 4.3 × 3.9 mm). The SUV was calculated after adjusting for injected radioactivity and body weight.
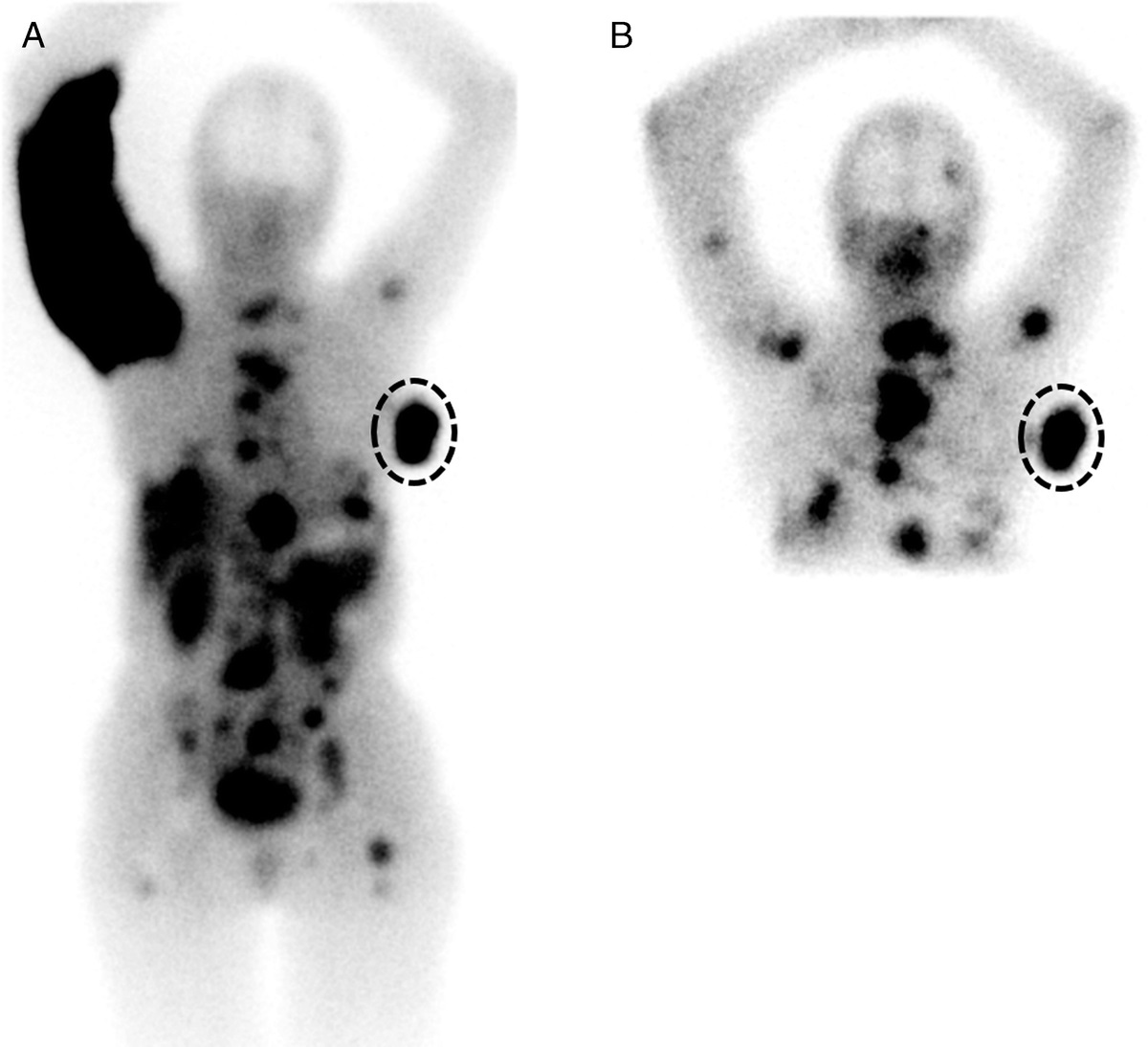
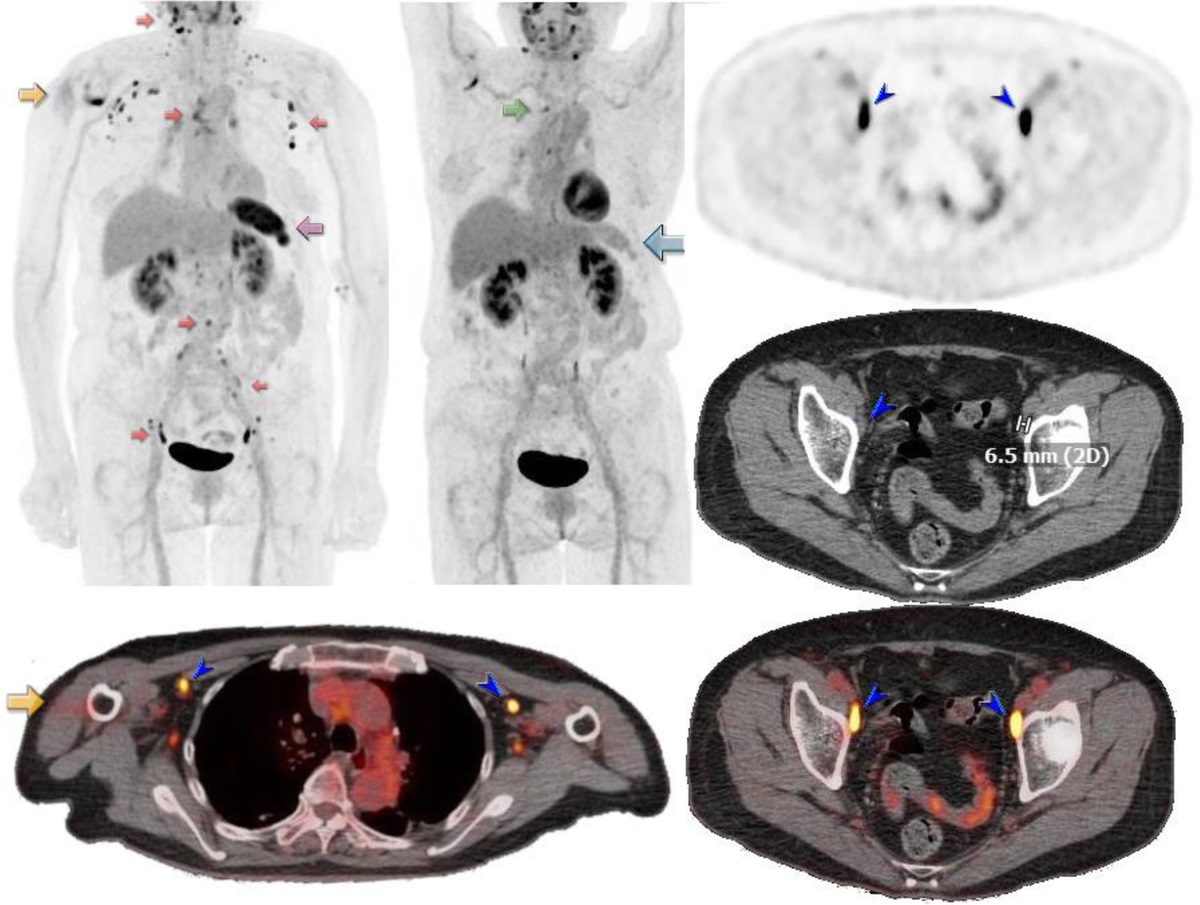
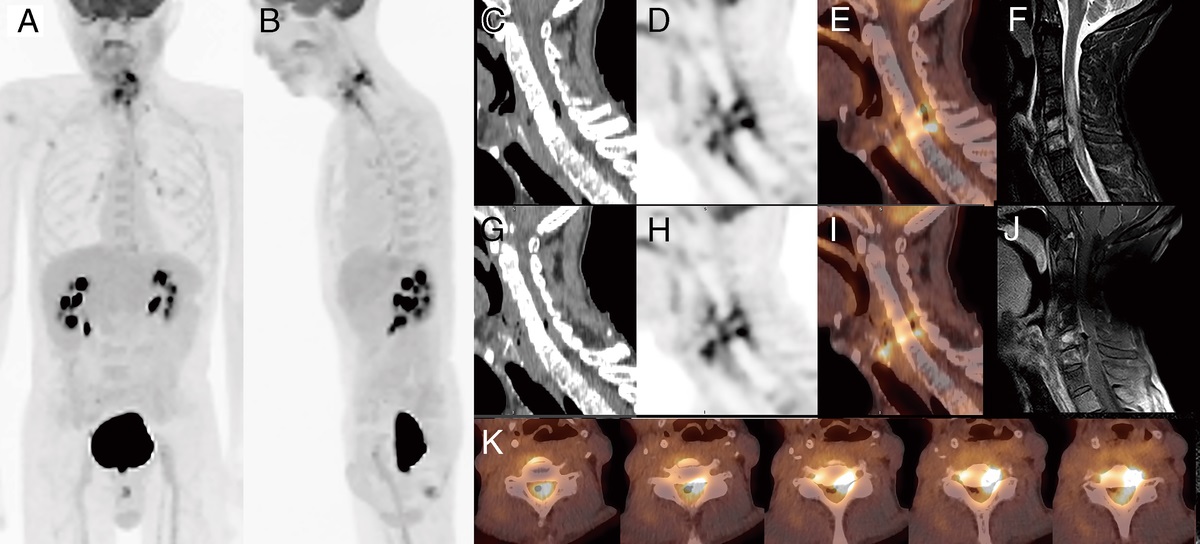
Clinical Variables and PET ParametersAge, sex, disease duration, and BTX history more than 16 weeks ago were included as clinical variables through electronic medical record review. The names and the number of EMG mapping-performed muscles, the names and the number of BTX-injected muscles, and the total amount of injected BTX volume were also obtained through injection therapy records. The names and number of hypermetabolic muscles and the SUVmax of each hypermetabolic muscle were evaluated in PET/CT images. Abnormal hypermetabolic muscles were defined as muscles with increased FDG uptake to greater than the upper mediastinal blood pool activity (Fig. 1). The highest SUVmax among all hypermetabolic muscles and the sum of SUVmax of all hypermetabolic muscles (total SUVmax) were representative PET parameters in each patient along with the number of hypermetabolic muscles. In patients without hypermetabolic muscles, the highest SUVmax and total SUVmax were considered 1.0, which means an even distribution of FDG throughout the body. The image interpretation at the time of treatment was performed by an experienced nuclear medicine physician.
 FIGURE 1:
FIGURE 1: Representative images of FDG uptake in the cervical muscles of ICD. A, Multiple hypermetabolic muscles in the MIP image (left) of a 47-year-old male patient. FDG uptake is increased in a diffuse pattern in the cervical muscles. In the fusion axial image (right), FDG uptake is observed in deep muscles such as the left longus capitis muscle, left obliquus capitis inferior muscle, and left rectus capitis posterior muscle (arrows). B, Low metabolic muscles in the MIP image (left) of a 47-year-old female patient. Faint FDG uptake is observed in the right obliquus capitis inferior muscle (arrow) in the fusion axial image (right).
Procedure for BTX Therapy and Evaluation of ResponseTarget muscle selection for BTX therapy was mainly conducted by EMG mapping and 18F-FDG PET/CT findings.12 Abnormal dystonic activities in up to 16 muscles were evaluated by the rehabilitation medicine physician, using EMG with a Teflon-coated (Dupont, Wilmington, DE) monopolar needle electrode cannular. Botulinum toxin was injected into accessible muscles among the dystonic muscles identified by EMG and PET/CT. This procedure was performed under EMG guidance. All patients were injected with a total of 100–300 units of BTX, and each muscle was injected with an amount of 10–100 units. Patients left the hospital after assessment for immediate complications.
The TWSTRS scores were assessed by the rehabilitation medicine physician at the first visit and at week 4 after BTX injection. The TWSTRS score consisted of a severity subscale (0–35), a disability subscale (0–32), and a pain subscale (0–20), and the total score was calculated as the sum of the 3 subscales.16,17 A good response was defined as a reduction rate of at least 30% of the TWSTRS total score and a simultaneous decrease of at least 15 points of the TWSTRS total score.18 In our data, most patients with a reduction rate of at least 30% already had a total score decrease of at least 10, so the point decrease was adjusted to at least 15 for further stratification.
Statistical AnalysisIn the comparison of good and poor responders, Student t test was used for continuous variables and χ2 test was used for categorical (dichotomous) variables. Multivariable analysis for predicting good response by logistic regression model with forward selection method was performed using the significant variables of univariable analysis. Pearson correlation analysis was performed for the relationship between the PET/CT parameters and the baseline TWSTRS scores. IBM SPSS Statistics software Version 25.0 (IBM, Armonk, NY) was used, and a P value less than 0.05 was considered statistically significant.
RESULTS Patients CharacteristicsThe baseline characteristics of subjects are presented in Table 1. The mean age at the time of treatment was 45.8 years. The proportion of male was 44.9%, and the mean disease duration was 2.1 years. The mean baseline TWSTRS total score was 40.0, and BTX was injected into an average of 6.4 muscles. The average number of hypermetabolic muscles was 6.2, of which 3.3 muscles were injected with BTX. The highest SUVmax of hypermetabolic muscles was an average of 9.2, and total SUVmax of hypermetabolic muscles was an average of 39.2. Three patients had no hypermetabolic cervical muscles on PET/CT, and two of them showed poor responses.
TABLE 1 - Baseline Characteristics of Patients (n = 78) Characteristic Mean ± SD Range Age, y 45.8 ± 11.4 19–72 Sex (male), n (%) 35 (44.9) Time since onset of cervical dystonia, y 2.1 ± 2.8 0.1–14.0 Previously treated with BTX earlier than 16 wk, n (%) 21 (26.9) Injected BTX volume, units 221 ± 51 100–300 TWSTRS total score, baseline 40.0 ± 12.7 14.3–66.0 TWSTRS severity subscale score, baseline 17.8 ± 5.2 5–31 TWSTRS disability subscale score, baseline 14.3 ± 6.0 0–26 TWSTRS pain subscale score, baseline 7.8 ± 5.4 0–18.0 No. BTX-injected muscles 6.4 ± 1.5 2–10 No. BTX-injected hypermetabolic muscles 3.3 ± 1.7 0–7 No. hypermetabolic muscles 6.2 ± 3.3 0*–18 The highest SUVmax among hypermetabolic muscles 9.2 ± 5.1 1.0*–28.1 Total SUVmax of hypermetabolic muscles 39.2 ± 31.2 1.0*–181.6*Three patients showed no hypermetabolic cervical muscles in PET/CT.
Table 2 shows the differences between good and poor responders. Half of the subjects showed a good response. The proportion of male was significantly higher, and the disease duration was significantly longer in poor responders (P = 0.003, P = 0.048, respectively). Good responders had significantly higher baseline TWSTRS total and 3 subscale scores than poor responders (total score, P < 0.001; severity score, P < 0.001; disability score, P < 0.001; pain score, P = 0.026). The number of BTX-injected muscles was higher in good responders (P = 0.044). For PET parameters, good responders had more hypermetabolic muscles and BTX-injected hypermetabolic muscles than poor responders (P < 0.001, both). Good responders showed higher total SUVmax of hypermetabolic muscles with marginal significance (P = 0.050). The highest SUVmax of hypermetabolic muscles was also likely to be higher in good responders but not statistically significant (P = 0.187).
TABLE 2 - Comparison of Characteristics Between Good and Poor Responders Characteristic Good Responder* (n = 39) Poor Responder* (n = 39) P Age, y 45.9 ± 10.4 45.8 ± 12.5 0.969 Sex (male), n (%) 11 (28.2) 24 (61.5) 0.003† Time since onset of cervical dystonia, y 1.5 ± 2.0 2.8 ± 3.4 0.048† Previously treated with BTX earlier than 16 wk, n (%) 10 (25.6) 11 (28.2) 0.799 Injected BTX volume, units 225.6 ± 39.5 215.9 ± 60.4 0.402 TWSTRS total score, baseline 46.9 ± 9.5 33.0 ± 11.8 <0.001† TWSTRS severity subscale score, baseline 20.0 ± 4.6 15.6 ± 5.0 <0.001† TWSTRS disability subscale score, baseline 17.7 ± 4.4 10.9 ± 5.4 <0.001† TWSTRS pain subscale score, baseline 9.2 ± 5.5 6.5 ± 5.1 0.026† No. BTX-injected muscles 6.7 ± 1.2 6.0 ± 1.7 0.044† No. BTX-injected hypermetabolic muscles 4.0 ± 1.8 2.5 ± 1.4 <0.001† Proportion of BTX-injected muscles among hypermetabolic muscles 0.5 ± 0.2 0.5 ± 0.2 0.981 No. hypermetabolic muscles 7.5 ± 3.3 4.8 ± 2.7 <0.001† The highest SUVmax among hypermetabolic muscles 10.0 ± 4.8 8.5 ± 5.2 0.187 Total SUVmax of hypermetabolic muscles 46.1 ± 28.6 32.4 ± 32.5 0.050*Good responders showed a reduction rate ≥30% and a point decrease ≥15 of the TWSTRS total score at 4 weeks after injection; poor responders showed a reduction rate <30% or a point decrease <15 of the TWSTRS total score at 4 weeks after injection.
†Statistically significant.
The multivariable analysis for good response was performed using the significant clinical and PET/CT variables mentioned previously (Table 3). Sex, baseline TWSTRS disability subscale score, and the number of BTX-injected hypermetabolic muscles were significant predictors. Male patients were less likely to have a good response (hazards ratio, 0.190; P = 0.010). Patients with a higher baseline TWSTRS disability score were more likely to have a good response (hazards ratio, 1.259; P = 0.001). Patients with a large number of BTX-injected hypermetabolic muscles had a higher probability of good response (hazards ratio, 1.574; P = 0.028).
TABLE 3 - Multivariable Analysis for Good Response by Logistic Regression Model With Forward Selection Characteristic HR 95% CI P Sex, female vs male 0.190 0.053–0.677 0.010* Time since onset of cervical dystonia 0.584 TWSTRS total score, baseline 0.266 TWSTRS severity subscale score, baseline 0.117 TWSTRS disability subscale score, baseline 1.259 1.106–1.434 0.001* TWSTRS pain subscale score, baseline 0.687 No. BTX-injected muscles 0.967 No. BTX-injected hypermetabolic muscles 1.574 1.051–2.356 0.028* No. hypermetabolic muscles 0.832 Total SUVmax of hypermetabolic muscles 0.623*Statistically significant.
HR, hazards ratio; CI, confidence interval.
The relationship between PET/CT parameters and baseline TWSTRS scores was assessed and suggested in Table 4. The number of hypermetabolic muscles showed a moderate positive correlation with the baseline TWSTRS total, severity, disability scores, and a weak positive correlation with the TWSTRS pain score (total, γ = 0.531, P < 0.001; severity, γ = 0.509, P < 0.001; disability, γ = 0.445, P < 0.001; pain, γ = 0.264, P = 0.019). There was a weak positive correlation between the highest SUVmax of hypermetabolic muscles and the baseline TWSTRS total and disability scores (total, γ = 0.234, P = 0.039; disability, γ = 0.309, P = 0.006). There was also weak positive correlation between the total SUVmax of hypermetabolic muscles and the baseline TWSTRS total, severity, and disability scores (total, γ = 0.339, P = 0.002; severity, γ = 0.289, P = 0.010; disability, γ = 0.327, P = 0.004). The higher the number of hypermetabolic muscles and the higher the SUVmax values, the higher the TWSTRS scores.
TABLE 4 - Correlation Between PET/CT Parameters and Baseline TWSTRS Scores PET/CT Parameter TWSTRS γ P No. hypermetabolic muscles Total 0.531 <0.001* Severity 0.509 <0.001* Disability 0.445 <0.001* Pain 0.264 0.019* The highest SUVmax among hypermetabolic muscles Total 0.234 0.039* Severity 0.121 0.293 Disability 0.309 0.006* Pain 0.093 0.420 Total SUVmax of hypermetabolic muscles Total 0.339 0.002* Severity 0.289 0.010* Disability 0.327 0.004* Pain 0.157 0.169The column chart of detected dystonic cervical muscles by PET/CT and EMG mapping was presented in Figure 2. When noticing only PET/CT-identified muscles, PET/CT well detected deep muscles in the prevertebral area (longus capitis muscle, longus colli muscle) and in the suboccipital area (obliquus capitis superior muscle, obliquus capitis inferior muscle, rectus capitis posterior major muscle). On the other hand, EMG showed strength in detecting superficial muscles such as the upper trapezius and levator scapulae muscles.
 FIGURE 2:
FIGURE 2: Column chart of dystonic cervical muscles reported by EMG mapping and PET/CT. SPC, splenius capitis; multi, multifidus; uTz, upper trapezius; SSC, semispinalis capitis; LS, levator scapulae; Lc, longus capitis; LC, longus colli; OCS, obliquus capitis superior; OCI, obliquus capitis inferior; LGC, longissimus capitis, RCPM, rectus capitis posterior muscle; SCM, sternocleidomastoid muscle; scal, scalene muscle; diga, digastric muscle; strap, strap muscle; platy, platysma muscle.
DISCUSSIONThis study investigated the role of 18F-FDG PET/CT in predicting and improving BTX therapy response in ICD. To the best of our knowledge, this is the first study comparing good and poor responders to PET/CT-assisted BTX therapy. Good responders had higher baseline TWSTRS scores, a greater number of hypermetabolic muscles, and shorter disease duration. There was a previous, similar study that reported patients with higher baseline TWSTRS total score had a higher probability of BTX-A response.19 Another study reported that the greater the cervical dystonia severity, the more likely patients were to respond to BTX-A.20 The treatment response was better in the acute stage with high muscle activity. On the contrary, as chronic and repetitive strains persist, the neck muscles become fixed in a contracted or shortened state. These cervical muscles can develop atrophy and interstitial fibrosis.21 Since these muscles have low exertion activity, it is assumed that the relaxation effect of BTX is relatively low. Low exertion activity is expressed with low FDG uptake in PET/CT and thus results in a small number of hypermetabolic muscles in poor responders.
In multivariable analysis for good response, the treatment response was better in patients with a large number of BTX-injected hypermetabolic muscles. This point is noteworthy because each of the number of BTX-injected muscles and the number of hypermetabolic muscles were not statistically significant. That means there should be many muscles that are metabolically active and simultaneously injected with BTX. It seems to be advantageous to inject BTX into as many identified hypermetabolic muscles as possible, particularly in patients with a large number of initial hypermetabolic muscles. In patients with a small number of pretreatment hypermetabolic muscles, the response might not be satisfactory even if BTX is injected into as many muscles as possible. Therefore, FDG PET/CT might be essential for planning and predicting response to BTX injection therapy in ICD. In addition, the disability subscale score was the only significant predictor for response among all baseline TWSTRS scores in multivariable analysis. It is necessary to pay more attention to how much the patient’s daily life is affected by ICD before treatment.
The baseline TWSTRS scores and PET parameters were positively correlated. Patients with a higher number of hypermetabolic muscles and higher SUVmax were more likely to have higher TWSTRS scores. This is consistent with the aforementioned therapy response comparison in terms of disease severity. In particular, the number of hypermetabolic muscles was related to all TWSTRS subscale scores. A previous study investigated the relationship between PET parameters and TWSTRS scores. Lee et al22 reported that the highest SUVmax was positively correlated with TWSTRS total, severity, and disability scores. The TWSTRS scores were based on symptoms, abnormal findings in neck motion, and impact on daily activities. It has been widely used as a tool to evaluate disease severity and therapy response in spasmodic torticollis.23 FDG uptake is known to be increased in exerted muscles and inflammation in PET/CT.24–26 A hypermetabolic muscle therefore refers to a strained or contracted muscle causing spasmodic torticollis. If the TWSTRS score is a clinical index for disease severity, the number of hypermetabolic muscles and the degree of FDG uptake (SUV) can be imaging indexes for muscle activity.
Although it was difficult to compare the detection rate between PET/CT and EMG since EMG mapping was not performed for all neck muscles but only for muscles with a dystonic potential related to posture, PET/CT was obviously helpful in detecting deep overactive cervical muscles. When the BTX-injected muscles in our data were assessed, there were some cases where BTX was injected into the obliquus capitis superior muscle or obliquus capitis inferior muscle because PET/CT identified them. PET/CT may improve treatment outcomes when these muscles are the cause of ICD. Revuelta et al27 reported that FDG PET/CT was useful for both superficial and deep muscles for identifying overactive dystonic muscles, which is in line with our study. For finding superficial dystonic muscles, Jang et al28 reported that FDG PET/CT was superior to EMG for specificity and accuracy, whereas EMG was superior to PET/CT for sensitivity. The detection of the 2 modalities for superficial muscles in our data was also similar.
Regarding the contribution of PET/CT on therapeutic effect, we compared the treatment outcomes of our PET/CT-assisted group and the historical control group.16 The response rate with TWSTRS total score decreasing more than 30% was 67.9% (53/78 patients) in our data, which was higher than that of 49.1% (27/55 patients) in the conventional historical EMG only group (P = 0.029). Similar to the present study, a previous study reported a lower probability of BTX reinjection and a higher TWSTRS reduction rate after 3 to 6 months in the PET/CT-assisted targeting group compared with the clinically targeting group.13 It is thought that the selection of functioning muscle by PET/CT plays a key role in improving the therapeutic effect of BTX.
This study has several limitations. First, muscles that were difficult to access or were judged by the clinician to be of low importance were not injected with BTX. Despite frequent reports of longus colli and longus capitis muscle on PET/CT, it was difficult to confirm the effect of these muscles on the improvement of the treatment because of rare actually injected cases. Second, accurate comparison with the historical control group was difficult to be included in the main results because of the partially matched inclusion criteria and the different skill levels of physicians performing BTX injection. A randomized controlled study for accurate comparison in treatment outcomes between the PET/CT-assisted and conventional EMG-guided groups is warranted.
CONCLUSIONSFDG PET/CT-assisted BTX injection therapy shows good therapeutic efficacy in ICD patients. The numbers of hypermetabolic cervical muscles and BTX-injected hypermetabolic muscles may be helpful in predicting a good response along with baseline TWSTRS scores. PET/CT was helpful in finding abnormal hypermetabolic cervical muscles not reported by EMG mapping.
REFERENCES 1. LaHue SC, Albers K, Goldman S, et al. Cervical dystonia incidence and diagnostic delay in a multiethnic population. Mov Disord. 2020;35:450–456. 2. Ortiz R, Scheperjans F, Mertsalmi T, et al. The prevalence of adult-onset isolated dystonia in Finland 2007–2016. PLoS One. 2018;13:e0207729. 3. Dauer WT, Burke RE, Greene P, et al. Current concepts on the clinical features, aetiology and management of idiopathic cervical dystonia. Brain. 1998;121(Pt 4):547–560. 4. Tomic S, Petkovic I, Pucic T, et al. Cervical dystonia and quality of life. Acta Neurol Belg. 2016;116:589–592. 5. Dressler D, Adib Saberi F. Botulinum toxin: mechanisms of action. Eur Neurol. 2005;53:3–9. 6. Scott AB. Development of botulinum toxin therapy. Dermatol Clin. 2004;22:131–133, v. 7. Petitclerc M, Cloutier M, Naud P, et al. Improvement in quality of life with OnabotulinumtoxinA for cervical dystonia: POSTURe. Can J Neurol Sci. 2021;48:676–684. 8. Yablon SA, Brashear A, Gordon MF, et al. Formation of neutralizing antibodies in patients receiving botulinum toxin type a for treatment of poststroke spasticity: a pooled-data analysis of three clinical trials. Clin Ther. 2007;29:683–690. 9. Tucker H, Osei-Poku F, Ashton D, et al. Management of secondary poor response to botulinum toxin in cervical dystonia: a multicenter audit. Mov Disord Clin Pract. 2021;8:541–545. 10. Jost WH, Tatu L. Selection of muscles for botulinum toxin injections in cervical dystonia. Mov Disord Clin Pract. 2015;2:224–226. 11. Jankovic J. Needle EMG guidance for injection of botulinum toxin. Needle EMG guidance is rarely required. Muscle Nerve. 2001;24:1568–1570. 12. Lee IH, Yoon YC, Sung DH, et al. Initial experience with imaging-guided intramuscular botulinum toxin injection in patients with idiopathic cervical dystonia. AJR Am J Roentgenol. 2009;192:996–1001. 13. Lee HB, An YS, Lee HY, et al. Usefulness of (18)f-fluorodeoxyglucose positron emission tomography/computed tomography in management of cervical dystonia. Ann Rehabil Med. 2012;36:745–755. 14. Sung DH, Choi JY, Kim DH, et al. Localization of dystonic muscles with 18F-FDG PET/CT in idiopathic cervical dystonia. J Nucl Med. 2007;48:1790–1795. 15. Comella CL, Buchman AS, Tanner CM, et al. Botulinum toxin injection for spasmodic torticollis: increased magnitude of benefit with electromyographic assistance. Neurology. 1992;42:878–882. 16. Truong D, Brodsky M, Lew M, et al. Long-term efficacy and safety of botulinum toxin type a (Dysport) in cervical dystonia. Parkinsonism Relat Disord. 2010;16:316–323. 17. Boyce MJ, Canning CG, Mahant N, et al. The Toronto Western Spasmodic Torticollis Rating Scale: reliability in neurologists and physiotherapists. Parkinsonism Relat Disord. 2012;18:635–637. 18. Truong D, Duane DD, Jankovic J, et al. Efficacy and safety of botulinum type a toxin (Dysport) in cervical dystonia: results of the first US randomized, double-blind, placebo-controlled study. Mov Disord. 2005;20:783–791. 19. Jankovic J, Schwartz M, Adams A. Predictors of onabotulinumtoxina response in patients with cervical dystonia. Toxicon. 2016;123:S43–S44. 20. Felicio AC, Godeiro-Junior C, de Carvalho Aguiar P, et al. Predictable variables for short- and long-term botulinum toxin treatment response in patients with cervical dystonia. Neurol Sci. 2009;30:291–294. 21. Gonzalez-Usigli H, Espay AJ. A rare cervical dystonia mimic in adults: congenital muscular torticollis (fibromatosis colli). Front Neurol. 2013;4:6. 22. Lee HJ, An YS, Ahn YW, et al. Threshold of clinical severity of cervical dystonia for positive (18)F-FDG PET/CT. Ann Rehabil Med. 2013;37:777–784. 23. Jost WH, Hefter H, Stenner A, et al. Rating scales for cervical dystonia: a critical evaluation of tools for outcome assessment of botulinum toxin therapy. J Neural Transm (Vienna). 2013;120:487–496. 24. Soto-Heredero G, Gomez de Las Heras MM, Gabande-Rodriguez E, et al. Glycolysis—a key player in the inflammatory response. FEBS J. 2020;287:3350–3369. 25. Pereira RM, Moura LPd, Muñoz VR, et al. Molecular mechanisms of glucose uptake in skeletal muscle at rest and in response to exercise. Mot Rev Educ Fís. 2017;23. 26. Tashiro M, Fujimoto T, Itoh M, et al. 18F-FDG PET imaging of muscle activity in runners. J Nucl Med. 1999;40:70–76. 27. Revuelta GJ, Montilla J, Benatar M, et al. An 18F-FDG PET study of cervical muscle in parkinsonian anterocollis. J Neurol Sci. 2014;340:174–177. 28. Jang SJ, Choi JY, Sung DH, et al. Comparison between (18)F-FDG PET/CT and EMG mapping for identifying dystonic superficial muscles in primary cervical dystonia: preliminary results. Nucl Med Mol Imaging. 2010;44:33–38.
留言 (0)