
記住我
Many patients with diabetic neuropathy experience neuropathic pain, which can affect daily functioning, sleep, general well-being and quality of life.
Symptomatic treatment of neuropathic pain is challenging.
Topical lidocaine 700 mg medicated plaster (LMP) has demonstrated good effectiveness with a good tolerability profile in the treatment of localized peripheral neuropathic pain.
WHAT THIS STUDY ADDSThe study compared outcomes in a large cohort (n=732) of matched patients with painful diabetic peripheral neuropathy (PDPN) treated either with LMP or with oral medications (OM).
The study demonstrated better effectiveness and tolerability of LMP compared with well-established OM for the treatment of PDPN in routine clinical practice.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICYIntroductionDiabetic neuropathies are common chronic microvascular complications affecting the somatic and/or autonomic nervous system exclusively as a consequence of diabetes mellitus.1 2 The most common type is distal symmetrical polyneuropathy defined for clinical practice as ‘the presence of symptoms and/or signs of peripheral nerve dysfunction in people with diabetes after the exclusion of other causes’.1 Many patients with diabetic neuropathy experience neuropathic symptoms such as burning, shooting, or lancinating pain (with or without numbness), tingling sensations, or stimulus-evoked pain (allodynia or hyperalgesia).3 4 In Europe, the prevalence of painful diabetic peripheral neuropathy (PDPN) ranges from 6% to 34% of patients with diabetes.5 PDPN affects daily functioning and sleep, often results in anxiety and depression, and is associated with diminished quality of life; the impact on both the individual patient and society is significant.5
Symptomatic treatment of neuropathic pain is challenging. Available pharmacological treatment options for painful diabetic neuropathy have been recently reviewed.6–8 Recent guidelines for PDPN treatment mainly recommend pharmacotherapy with tricyclic antidepressants (TCAs), the antiepileptics pregabalin and gabapentin, the selective serotonin-norepinephrine reuptake inhibitors (SSNRIs) duloxetine and venlafaxine, and high concentration capsaicin 179 mg (8% w/w) patch.9 The lidocaine 700 mg medicated plaster (LMP) has been recommended for general peripheral neuropathic pain treatment in recent guidelines.10 11 The use of oral medications is limited by a number of factors including systemic side effects, drug–drug interactions, a slow onset of action, the need for titration, and the need for multiple daily dosing,12 which can lead to suboptimal adherence to treatment. A US claims database analysis estimated that up to 50% of patients discontinued their initial PDPN treatment within 3 months of initiation.13 In contrast, topical treatments provide pain relief by directly targeting the site of the pain, and the low systemic exposure reduces the risk of systemic side effects. Thus, the benefit/risk ratio of topical treatments may be more favorable than that of oral medications, and they may offer a valuable analgesic treatment option, particularly considering that patients with PDPN are often multimorbid and polymedicated.
Real-world data can provide insights into what may be effective treatment paradigms for routine clinical practice. To date, LMP is approved in 54 countries worldwide for postherpetic neuralgia; its effectiveness and good tolerability in the treatment of this condition was recently confirmed by real-world data obtained from the German Pain eRegistry (GPeR).14 Additionally, LMP has been approved in 15 of these countries for the treatment of localized peripheral neuropathic pain (including PDPN). As LMP has also been used for the treatment of localized peripheral neuropathic pain conditions other than postherpetic neuralgia in Germany, GPeR data were available for an analysis of the datasets of all patients with PDPN treated with either topical LMP or oral medications.
Research design and methodsThe datasets in this subgroup analysis of patients with PDPN were included in a previously reported non-interventional study analyzing data of patients with localized peripheral neuropathic pain obtained from the GPeR.15 Patients had been unsuccessfully treated with recommended16 oral first-line medications (OM) and had been receiving a new treatment of either LMP or an OM and were then followed up for 24 weeks.15 Based on individual patient needs and prior treatment experience, treating physicians solely decided about the selection of analgesic medication, initial dosing, dose adjustments, continuation or discontinuation based on individual response, and other treatment options. Propensity score matching in the original study15 provided 732 pairs of datasets from patients with a diagnosis of PDPN for a comparison of LMP and oral first-line medications.
Outcome measures and statistical analysisOutcome parameters have already been described in detail for the original study and two previous subgroup analyses14 15 17 and included pain intensity, pain-related impairments in daily activities (modified Pain Disability Index (mPDI)), pain-related quality of life (Quality of Life Impairment by Pain (QLIP) Inventory Questionnaire), overall quality of life (Short Form 12 V.2, summarized in a Physical Component Score (PCS) and a Mental Component Score (MCS)),18 pain phenotype (painDETECT Questionnaire 7 (PDQ7)),19 change in health status (Patient Global Impression of Change (PGIC)),20 occurrence of drug-related adverse events (DRAEs), and treatment discontinuation due to DRAEs. Patient-reported/relevant outcomes were obtained with validated instruments (recommended by the German pain physician and pain patient organizations). The primary effectiveness endpoint was the absolute change in average 24-hour Pain Intensity Index (PIX; arithmetic mean of the lowest, average, and highest 24-hour pain intensities) from baseline after 4, 12, and 24 weeks of treatment and over the entire treatment period. Further endpoints included changes from baseline at the three timepoints in other effectiveness assessments, as well as treatment response defined as ≥30% and ≥50% reduction in PIX, change in health status, DRAE occurrence, reasons for premature discontinuation, and change in concomitant medications during observation. Treatment differences were compared using mixed-model repeated measures covariance analyses with Student’s t-test, Pearson’s χ2 test, and Fisher’s exact test for between-group comparisons and paired samples t-tests for within-group comparisons (significance p<0.05 without adjustments for multiplicity). Cohen’s d was used to determine the effect size of the comparisons for the primary variable. PASW Statistics V.18 was used for statistical analysis, and the Medical Dictionary for Regulatory Activities V.22.0 was used for AE coding.
ResultsPatientsBaseline characteristics of the two matched PDPN treatment groups are shown in table 1. Over 50% of the patients were >60 years old; all were multimorbid with a median of four comorbidities per patient and received a median of six non-analgesic medications. Despite the administration of a median of seven (LMP group) or eight (OM group) previous analgesics, pain intensity at baseline was high and was accompanied by considerable impairments in daily activities and pain-related quality of life (table 1).
Table 1Baseline characteristics of the two treatment groups
Analgesic treatmentThe mean duration of treatment with LMP was 141.5±49.2 days (95% CI 137.9 to 145). Treatment of <24 weeks was documented for 29.9% of the patients with the main reasons for discontinuation provided being ‘pain treatment no longer required’ (17.1% of patients), ‘lack of efficacy’ (4.9%), ‘due to DRAEs’ (4.4%), and ‘unclear information’ (3.6%). The mean treatment duration in patients treated with OM was 97.8±66.2 days (95% CI 93 to 102.6). They received antiepileptic medications (37.8%; pregabalin 31.3%, gabapentin 6.6%), SSNRIs (33.3%; duloxetine 24.5%, venlafaxine 8.9%), or TCAs (28.8%; amitriptyline 15.6%, imipramine 4.6%, nortriptyline 4.4%, trimipramine 2.7%, clomipramine 1.5%). A total of 58.9% of patients on OM discontinued treatment earlier than 24 weeks mainly due to DRAEs (35.8%). Further reasons were ‘lack of efficacy’ (12.2%), ‘pain treatment no longer required’ (7.4%), and ‘unclear information’ (3.6%).
All patients in both treatment groups received concomitant analgesic medications at baseline (figure 1). Concomitant analgesic use was reduced in both groups but in significantly more LMP than OM patients after 24 treatment weeks (91.9% vs 68%, p<0.001). The same was observed for the use of rescue medication (43.9% vs 35.8%, p<0.001). More patients on LMP than patients on OM had discontinued concomitant analgesics and rescue medication at the end of observation (figure 1).
 Figure 1
Figure 1 Change in concomitant medication and in rescue medication over the 24-week observation period (last observation carried forward). Data for non-opioids and mild opioids are not shown. LMP, lidocaine 700 mg medicated plaster; OM, oral medication.
Pain intensityAt baseline, the mean PIX was 64.2±14.9 mm for patients on LMP and 64.1±14.9 mm for patients on OM (table 1). Reductions in pain intensity were already considerable after 4 weeks of LMP treatment with further slight improvements in the following 20 weeks. The absolute change in average 24-hour PIX from baseline (primary effectiveness endpoint) was significantly greater for patients on LMP than for patients on OM at all three timepoints (4, 12, and 24 weeks of treatment) with an effect size of 0.662 at end of observation (figure 2A). The change in absolute scores for the average 24-hour PIX was mean −30.2 mm (SE 0.38) in the LMP group and −17.0 mm (SE 0.51) in the OM group over the 24-week treatment period. A relative mean change from baseline in PIX was noted in 51.4% of patients on LMP and 27.7% of patients on OM at end of observation (p<0.001, Cohen’s d=0.888). Treatment response after 24 weeks was significantly higher in the LMP group than in the OM group (figure 2B).
 Figure 2
Figure 2 Change from baseline in different effectiveness parameters over the observation period (last observation carried forward). (A) Average 24-hour PIX (baseline observation carried forward for patients discontinuing treatment due to lack of effectiveness, adverse event or death). (B) Improvement versus baseline in PIX at the end of observation. (C) Pain-related impairment in daily life. (D) Quality of life impairment by pain. (E,F) Overall quality of life. Improvements are shown by reductions in PIX and mPDI, and by increases in quality of life parameters. mPDI, modified Pain Disability Index; NRS, Numerical Rating Scale; PIX, Pain Intensity Index; QLIP, Quality of Life Impairment by Pain; SF-12, Short Form 12; VAS, visual analogue scale.
Further outcomesPatients reported marked impairments in daily life activities at baseline (table 1), which improved under both treatments over the observation period (p<0.001 in favor of LMP, figure 2C). Similar to the observations for pain intensity changes, considerable improvements had already occurred after 4 weeks of LMP treatment with further slight improvements in the following 20 weeks.
Pain-related quality of life was also considerably impaired at baseline: 76.6% of patients on LMP and 73.6% of patients on OM were severely affected with a QLIP sum score of ≤20. Continuous improvements were observed under both treatments, however, with a significant treatment difference in favor of LMP (p<0.001, figure 2D). At week 24, the proportion of severely impaired patients had decreased to 12.7% in the LMP group and 32% in the OM group.
Overall quality of life with respect to the physical components was markedly affected at baseline. Under LMP treatment, it had already considerably improved after 4 treatment weeks with a further slight increase until the end of observation (median relative change 10.1% after 4, 11.2% after 12, and 12.1% after 24 weeks). In contrast, the median relative change under OM treatment was 0%, 0%, and 1.1%, respectively. Improvements under LMP treatment were significantly greater than under OM treatment over the observation period (p<0.001, figure 2E). The MCS of quality of life only slightly changed over the observation period but to a significantly greater extent in the LMP group (p<0.001, figure 2F). The median relative change from baseline was 2.6%, 2.9%, and 4% for LMP and 0% under OM treatment.
At baseline, mean (SD) PDQ7 scores were 26.7±3.4 in both groups. A marked reduction was already observed in the LMP group after 4 treatment weeks. At all three timepoints, reductions were significantly greater in the LMP group compared with the OM group (4 weeks: −8.5±3.3 vs -3.0±2.7, 12 weeks: −10.8±4.0 vs -4.5±3.6, 24 weeks: −11.4±4.2 vs -4.8±3.9; all p<0.001).
At end of observation, significantly more patients in the LMP group rated their health status on the PGIC as ‘much better’ or ‘very much better’ (77.3% vs 41.5% for OM, p<0.001).
TolerabilitySignificantly fewer patients on LMP than patients on OM experienced DRAEs (9.6% vs 61.6%, p<0.001; figure 3). Patients on LMP mainly reported application site reactions and other skin-related issues (table 2). In the OM group, the main DRAEs were nervous system disorders (27.5% of patients), psychiatric disorders (23.5%), and gastrointestinal disorders (17.8%), with somnolence (14.8%) and dizziness (6.7%) the most commonly documented DRAEs (table 2). A significantly smaller proportion of patients on LMP discontinued treatment due to DRAEs (4.4% vs 35.8% for patients on OM, p<0.001; figure 3).
Table 2Drug-related adverse events documented during the observation period (system organ class and preferred term)
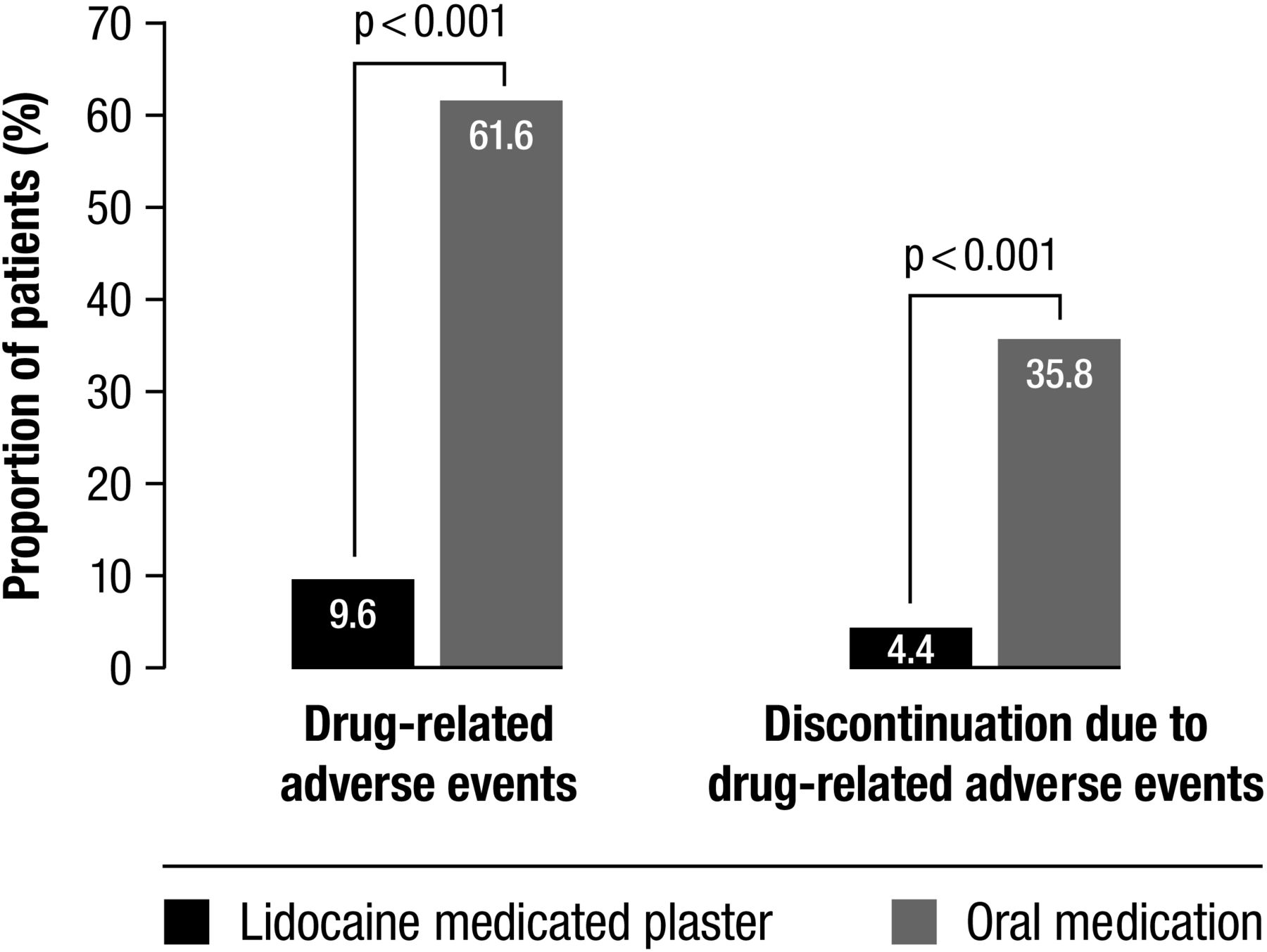 Figure 3
Figure 3 Drug-related adverse events and discontinuation due to these events over the observation period.
DiscussionThe substantial burden experienced because of decreased physical and emotional functioning associated with PDPN21 22 was also observed in our multimorbid and polymedicated study population. Over 80% of the patients had at least three comorbidities, and 90% were prescribed three or more non-analgesic concomitant medications. They consulted a median of 7 healthcare providers who prescribed a median of 7 (LMP group) or 8 (OM group) medications for their pain. Nevertheless, the pain burden at baseline was high, with considerable limitations in daily activities and diminished quality of life.
The mean age of the patients in our sample was 62.2 years. Especially for elderly populations, topical treatment options are important as treatment failure is frequent in neuropathic pain and is accompanied by central side effects with recommended oral drugs that affect the central nervous system. Such options are available and are supported by efficacy and safety data as confirmed in a review of 18 randomized controlled clinical trials supporting the efficacy of various topical treatments including LMP in the elderly.23
Restoring or preserving patients’ independence and quality of life is an important goal in pain management. In addition to pain intensity, it is thus also important to take into account the pain-related limitations in daily functioning and the pain-related distress experienced by the patient. The new International Classification of Diseases, 11th Revision, coding proposes these three dimensions as optional specifiers (‘extension codes’) for chronic pain diagnoses for the determination of pain severity.24 These dimensions can aid the selection of an appropriate pain medication. The German Diabetes Association states in their practice recommendations under pharmacotherapy for PDNP: ‘Pain therapy should not merely mitigate pain but should also improve the quality of sleep, mobility and overall quality of life’.2
The clinical practice data presented here show that topical LMP treatment considerably improved pain intensity and daily functioning and resulted in an overall better health status after 24 weeks of treatment. Marked improvements were already observed after 4 treatment weeks and were maintained over the treatment period. In particular, the effect on physical functioning in this population is remarkable, given that improvement in this domain could be very beneficial. There is increasing evidence that physical activity as well as dietary interventions are effective in reducing the severity of both somatic and autonomic neuropathies.25 There appeared to be no tolerance development to the LMP effect. The number of plasters used is determined by the skin area to be treated; the dose is therefore fixed and there is no tendency for a dose increase over time as can be observed with certain oral treatments. Effectiveness of the plaster was observed despite the lower intake of concomitant analgesic medications and rescue medications. Most patients on LMP (92%) could reduce and 43% were able to discontinue concomitant analgesics, thus easing the burden of polypharmacy. The decrease in strong opioid use (44% of the patients) is particularly noteworthy.
Only very few studies investigated the effectiveness of the lidocaine plaster exclusively for PDPN treatment.26–28 Significant improvements in a composite score of different pain qualities26 and in pain intensity and quality of life27 were observed in two short-term open-label studies with LMP as add-on to existing analgesic regimens. A randomized, open-label, non-inferiority trial with pregabalin as comparator showed a comparable treatment response and a comparable reduction in allodynia severity to pregabalin, and greater quality of life improvements under LMP treatment.28 To our knowledge, this is the only randomized trial comparing LMP to other analgesic medications in PDPN. A comparison of 29 pharmacological PDPN treatments using a network meta-analysis found the highest probability of 30% pain reduction for LMP compared with placebo.29 A second network meta-analysis suggests comparable effects in the reduction of DPN pain for the lidocaine plaster to amitriptyline, capsaicin creme, gabapentin, and pregabalin.30 The authors, did, however, state limited evidence due to small trial numbers. The real-world comparison with matched patients treated with oral medications presented here supports the clinical trial data and provides evidence for significantly greater improvements in all measured effectiveness parameters under LMP compared with OM treatment in the routine clinical practice setting.
Lidocaine is continuously released at the site of plaster application; however, only approximately 3%±2% reach systemic circulation.31 Adverse reactions based on systemic lidocaine effects are thus unlikely. As expected, no systemic side effects were reported under LMP treatment in this study. Adverse reactions were mainly associated with plaster application and other skin-related tolerability issues. The previously shown premature treatment discontinuation rate of below 5%32 was also observed with our clinical practice data. LMP tolerability was significantly better compared with oral medications. Most OM patients (62%) reported mainly nervous system, psychiatric, and gastrointestinal side effects and 36% discontinued earlier than 24 treatment weeks because of these adverse reactions. Our findings support the previously reported good short-term and long-term tolerability of the plaster32 and the generally better adverse event profile compared with oral medications.33 34 A recent benefit/risk analysis showed that LMP had a more favorable benefit/risk balance compared with pregabalin (300 and 600 mg/day) for the treatment of peripheral neuropathic pain.35
The focus of the current study was to compare LMP with oral treatments used as first-line treatments in PDPN. There are other topical treatments indicated for PDPN, such as the capsaicin 179 mg cutaneous patch. To our knowledge, no studies are available that directly compare LMP and the capsaicin patch when both are used as recommended. Recently, a meta-analysis of 12 trials compared topical treatments used for the treatment of postherpetic neuralgia and concluded that LMP was the most effective and most tolerable topical treatment.36
This subgroup analysis has all the limitations stated for the original non-interventional retrospective cohort study.15 Briefly, propensity score matching was employed to eliminate the main confounding factors and to reduce selection bias; however, other confounders might have been present. The registry data capture the prescribed regimens/dosages of the medications under evaluation but do not provide information about treatment compliance or reasons for the prescription of concomitant analgesics. Treatment outcomes could have been biased by the prescription of specific PDPN medications based on individual patient needs and the response to previous therapies. Physicians prescribing oral medications might also have paid closer attention to side effects. In addition, confirmation/verification of data to detect errors in measurement or misclassification was not possible, as only anonymized data were available due to data protection regulations.
ConclusionsThe effectiveness and good tolerability of LMP was confirmed in a large cohort of patients with PDPN in routine clinical practice. The reduction in use of concomitant and rescue analgesic medication (and especially of opioid treatments) over time offers new perspectives for a reduced burden of polypharmacy with LMP treatment. Moreover, an overall improvement in physical functioning with LMP is an encouraging feature that may help to reduce the overall burden of the disease.
Data availability statementNo data are available. Data cannot be made available. According to German Pain eRegistry standard procedures, data are only temporarily extracted from the database and are deleted after completion of the analyses specified in the research project.
Ethics statementsPatient consent for publicationEthics approvalThis study involves human participants and was conducted in accordance with the Declaration of Helsinki and relevant national and regulatory requirements. The concept and use of the German Pain eRegistry were reviewed and approved by the steering committees of the German Pain Association and the German Pain League. All patients provided written informed consent prior to participation in the registry. The study is registered with the European Network of Centers for Pharmacoepidemiology and Pharmacovigilance in the European Union Electronic Registry of Post-Authorization Studies. All analyses were carried out using only anonymised data to comply with German guidelines on protection of data privacy and with the European Union General Data Protection Regulation.
留言 (0)