
記住我

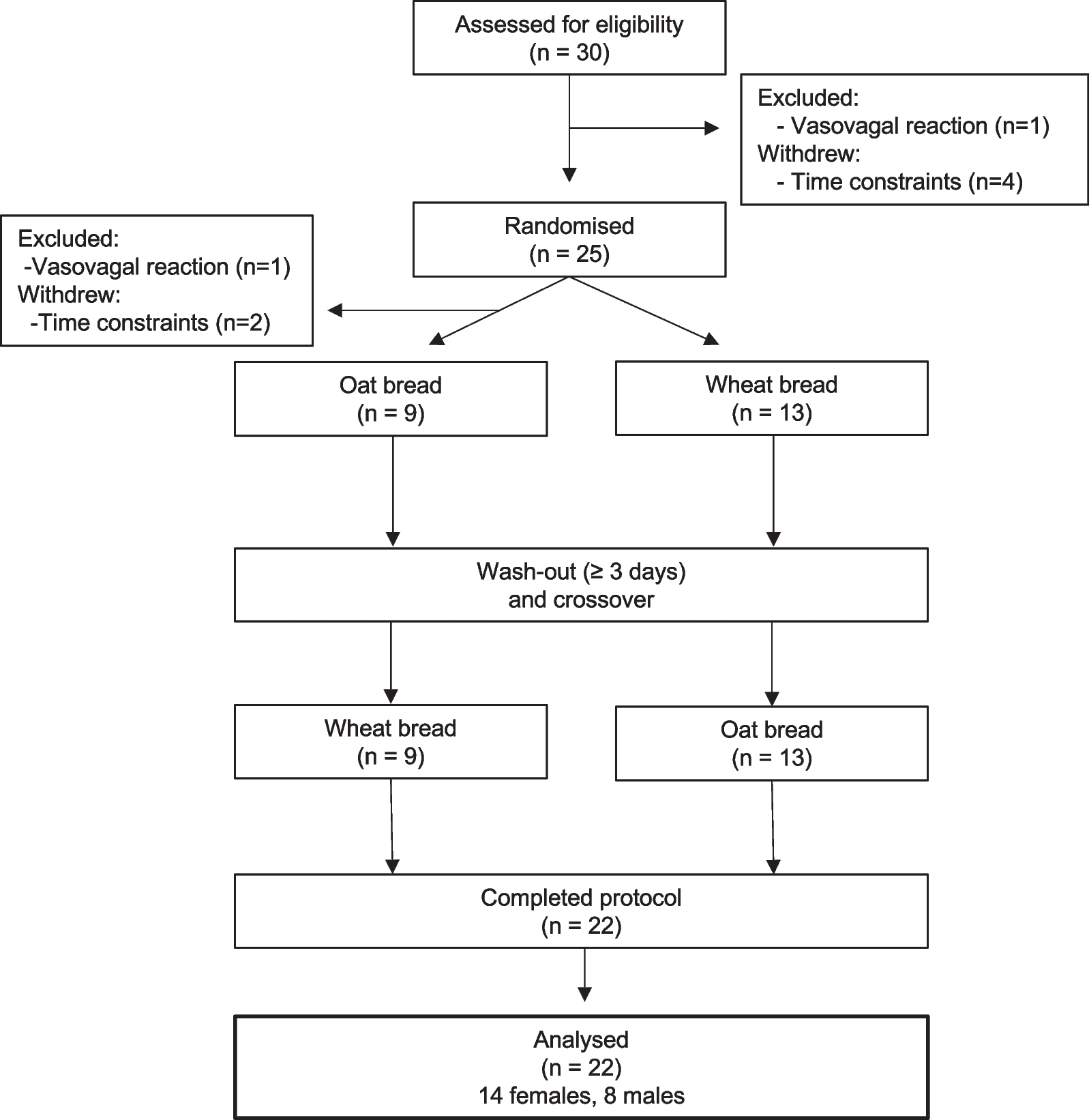

A total of 762 articles were retrieved (408 from PubMed, 86 from the Cochrane Library, 112 from the Web of Science, and 156 from Embase), of which 26 articles met the inclusion criteria. Sixteen articles were further excluded: 4 lacked a normal eating dietary strategy group [10,11,12,13]; in 2 articles, the intervention method was not TRE [14, 15]; in 8 articles, the BP value was incomplete [16,17,18,19,20,21,22,23]; and in 2 articles, the control group was a hypoenergetic diet [24, 25]. Therefore, 10 eligible studies [26,27,28,29,30,31,32,33,34,35] were included in the final meta-analysis. Of these, reference 24 included three groups, with two different TRE intervention groups. A flowchart of the study selection process is shown in Fig. 1.
Fig. 1
Flowchart of the study selection
Study characteristicsThe study characteristics are listed in Table 1, which includes data source and setting, study design, participants, study duration, TRE regimen (Fasting: Feeding), total number, age, sex, and BMI.
Table 1 Characteristics of the studies investigating the effects of Time-Restricted Eating on blood pressureMain outcomesA meta-analysis of ten studies [26,27,28,29,30,31,32,33,34,35] showed that TRE significantly reduced SBP (mean difference = −4.15, 95% CI: −6.73, −2.30; P < 0.0001), as shown in Fig. 2a. Meanwhile, TRE had no significant effect on DBP (mean difference = −2.06, 95% CI: −4.16, 0.02; P = 0.053), as shown in Fig. 2b. Although 10 studies were included, the graphs have 11 rows because reference 24 includes three groups, including two different TRE intervention groups.
Fig. 2
Forest plots of TRE vs. normal dietary eating in overall analyses, and a based on SBP changes b based on SBP changes c based on heart rate changes; d based on weight changes; and e based on blood glucose. TRE, time-restricted eating; SBP, systolic blood pressure
Secondary outcomesA meta-analysis of three studies [28, 33, 34] showed that TRE was unable to lower the heart rate (mean difference =0.36, 95% CI: −2.83, 3.54; P = 0.825), as shown in Fig. 2c.
The results of a meta-analysis of nine [27,28,29,30,31,32,33,34,35] studies showed that TRE significantly reduced weight (mean difference = −1. 63, 95% CI: −2.61, −0.64; P = 0.001), as shown in Fig. 2d.
A meta-analysis of seven studies [27,28,29, 31, 32, 34, 35] showed that TRE significantly reduced blood glucose levels (mean difference = −2.80, 95% CI: −4.64, −0.96; P = 0.003), as shown in Fig. 2e.
A meta-analysis of five studies [28, 31, 33,34,35] showed that TRE had no significant effect on total cholesterol (mean difference = 0.03, 95% CI: −10.01, 10.08; P = 0.995), as shown in Fig. 3a. A meta-analysis of eight studies [26,27,28, 31,32,33,34,35] showed that TRE insignificantly increased HDL-C (mean difference = 0.85, 95% CI: −1.80, 3.49; P = 0.531), as shown in Fig. 3b. A meta-analysis of seven studies [26,27,28, 31, 32, 34, 35] showed that TRE decreased LDL-C (mean difference = −0.86, 95% CI: −6.47, 4.76; P = 0.764), as shown in Fig. 3c. A meta-analysis of seven studies [26,27,28, 31, 32, 34, 35] showed that TRE decreased triglyceride levels (mean difference = −3.52, 95% CI: −9.49, 2.45; P = 0.248), as shown in Fig. 3d.
Fig. 3
Forest plots of TRE vs. normal eating dietary on blood lipids a based on cholesterol levels; b based on HDL-C; c based on LDL-C; and d based on triglycerides. TRE time-restricted eating; HDL-C high-density lipoprotein cholesterol; LDL-C low-density lipoprotein cholesterol
Subgroup analysisAs shown in Table 2, upon stratification by the duration of TRE intervention, we divided the studies into two groups 8 weeks (n = 3) and 12 weeks (n = 4). DBP was significantly reduced in patients with an intervention time of 12 weeks (WMD = −1.916 mmHg, 95% CI: −3.037, −0.794, P = 0.001), with low heterogeneity (I2= 0.0%).
Table 2 Subgroup Analysis. SBP, systolic blood pressure; DBP, diastolic blood pressure; WMD, weighted mean difference; 95% CI, 95% confidence intervalSensitivity analysisAs shown in Table 3, sensitivity analysis was performed on nine indicators, including SBP, DBP, heart rate, weight, glucose, total cholesterol, HDL-C, LDL-C, and triglycerides. After excluding studies individually, the combined effect size before and after did not change significantly, indicating that the results of the meta-analysis were relatively stable.
Table 3 Sensitivity Analysis. SBP, systolic blood pressure; DBP, diastolic blood pressure; HR,heart rate;95% CI, 95% confidence intervalMeta-regressionWe included nine studies that included changes in body weight and seven studies that included changes in blood glucose levels using meta-regression. The random-effect meta-regression of the primary meta-analysis on SBP revealed that body weight change (P = 0.044) predicted the size of the estimated treatment effect or explained heterogeneity between studies, while glucose (P = 0.867) did not. We further found that weight loss can predict TRE-induced SBP reduction.
Funnel plots and egger testsAs reflected by the filled funnel plots (Fig. 4), there was obvious heterogeneity in the SBP (Fig. 4b). In addition, as indicated by Egger’s tests, there was a low probability of publication bias for all indexes under study (all P > 0.05).
Fig. 4
Filled funnel plots of TRE vs. normal dietary eating a based on SBP changes; b based on SBP changes; c based on heart rate changes; d based on weight changes; e based on blood glucose levels; f based on cholesterol; g based on HDL-C; h based on the LDL-C; i based on triglycerides. TRE time-restricted eating; SBP systolic blood pressure; HDL-C high-density lipoprotein cholesterol; LDL-C low-density lipoprotein cholesterol
The quality of evidence assessmentTen studies included in our analysis were assessed for their quality. As shown in Fig. 5, we evaluated the quality assessment of the included studies using the risk of bias tool in Revman 5.4.
Fig. 5
The quality of evidence assessment
留言 (0)