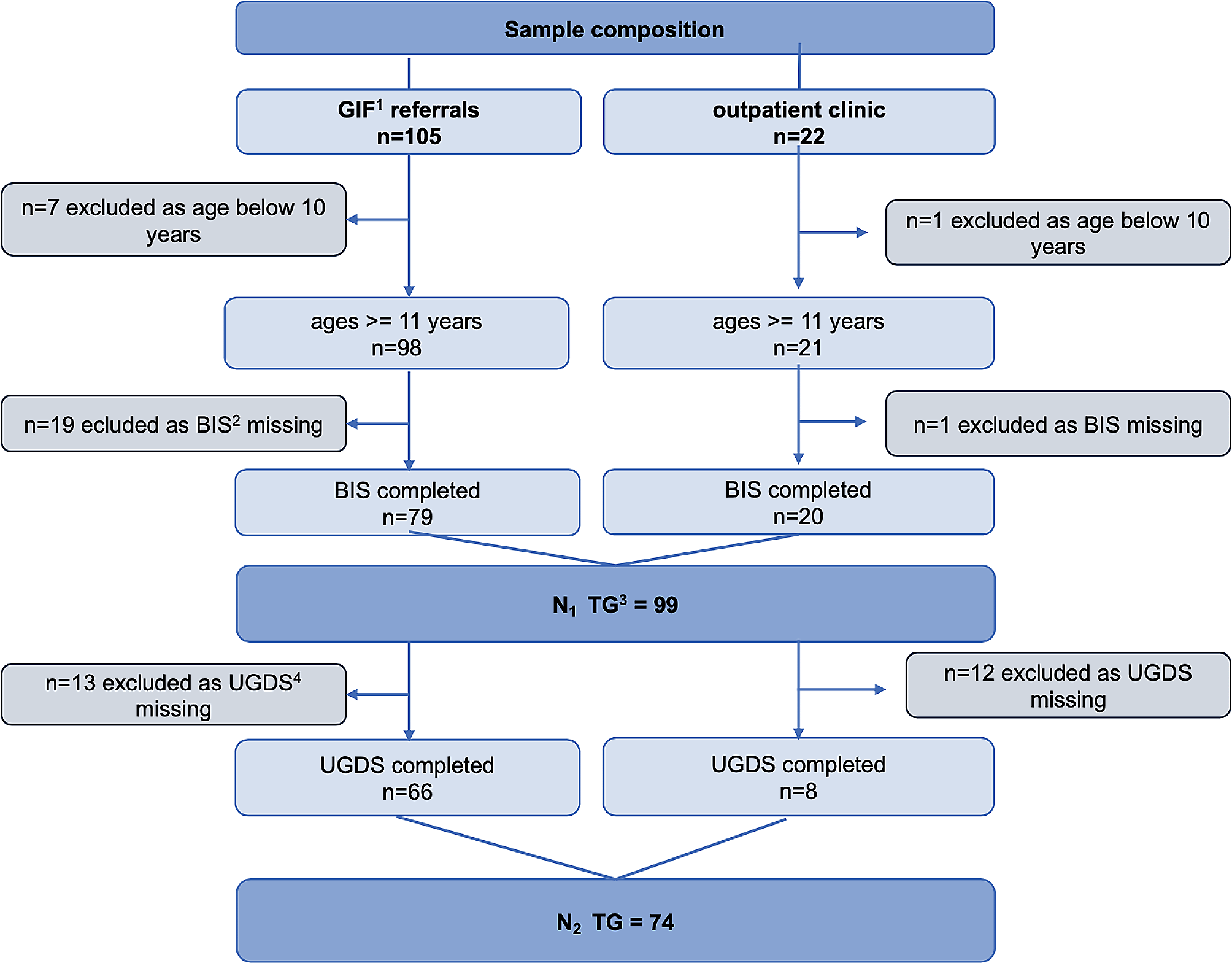
One hundred and eighteen patients participated in MUCTUM from June 2016 to April 2022. Participants were aged 11 to 17 yo and came from the following areas: Western Africa (Mali, Ivory Coast, Guinea, Senegal), Central Africa (Nigeria, Congo, Congo Kinshasa, Somalia), Northern Africa (Morocco, Algeria, Tunisia), Asia (Afghanistan, Pakistan, Bangladesh), and Europe (Albania). Most participants suffered from anxiety, depressive, or post-traumatic disorders, with a few experiencing psychotic disorders and addictive disorders. Sixteen interviews were conducted from April 2021 to April 2022, ranging from 20 min to one hour. Participants’ characteristics are described in Table 1. Analysis revealed that participants described strangeness and loneliness in relation to psychiatric symptoms, often feeling misunderstood before participating in MUCTUM. Several youth experienced triple stigmatization: of being UM, of suffering from psychotrauma, and of being mental health patients. Some reported feeling suspicious of care providers, due to negative cultural representations of mental health care or limited background knowledge of mental illness. As therapeutic alliance built up, participants felt increasingly helped by the consultations. They no longer experienced suspicion towards care providers, but rather trust. We identified three themes that reflect how UM feel supported, hoping to further improve caregivers’ interventions for UM: (1) A safe space for unaccompanied minors; (2) Helpful interventions during therapy; and (3) Narrating one’s story can “set us free'' if guided carefully by care providers. Themes and subthemes are summarized in Table 2.
Table 1 Sociodemographic characteristics of participantsTable 2 Themes and subthemesA safe space for unaccompanied minorsA secure therapeutic framework
The perception that caregivers were compassionate, engaged in care, and steadily present despite repeated missed sessions was cited by participants as a major factor in building therapeutic alliance. Participants considered their care providers “trustful,” “skilled,” “deeply caring,” “generous,” knowledgeable on their culture, and always providing “thorough explanations.”
" I can have problems in my life and I call Mrs. X on her number. It's really... I don't know about the others, but for me, it's not only a follow-up at the hospital, it's really a follow-up that was really very thorough (...) I improved a lot of things, like anger. I, I worked with that with Dr. Y... anger and everything.... It was something that I couldn't handle... It allowed me to... really deal with some of the things about myself that I didn't like…”
According to UM, care providers offered much-needed guidance, giving advice and helping to find concrete solutions to daily life problems. They were perceived as role models, and even compared to a parent by some participants, “like a mother.” Several participants reported having the personal phone numbers of care providers (which is unusual in France) in case of crisis: “I could call or send a message (…) and that's what helped me even more, that made things easier for me.” All participants stressed that feeling welcomed at the first session had been essential: “The first time I came, it was great, I felt at ease just like at home.” Laughter was a notable event during the first meeting: "The first day, I was with my caseworker. It worked out well. [Care providers] had a good laugh with me too." According to participants, consistency of care increased adherence, even despite some missed appointments. Said one participant, “Only God knows how many times I didn’t come,” with continuation of MUCTUM contrasting sharply with previous care that canceled follow-ups after only two missed sessions. Care providers became secure references during transfer of care, sharing “knowledge” about participants with new care providers who “don’t know how to handle [them] yet.” Nevertheless, some participants mentioned that the presence of four adults – two care providers, one caseworker and one interpreter – led them to feel “afraid” or “lost” at the beginning. Despite being overwhelming, the presence of several adults was overall seen as helpful to discuss a variety of opinions.
“At first, I thought it was too much. I said to myself: there are too many people. But then I realized that when there are several people, we talk more. When there are several people, we discuss more, everyone gives their opinion. That's good. That's really good. I think that... Just at the beginning… I thought it was too much, but then I saw that it's better, when there are several people, each one speaks. They also, they talked a little bit about themselves. That's good.”
The interpreter prevents misunderstandings and is a reassuring link with the native country
Participants perceived interpreters as instrumental in achieving full understanding of their identity, origins, language, and culture. Interpreters prevented possible misunderstandings (“so that I don't understand the opposite meaning”) and helped overcome language barriers.
“With them, I was not alone, we were several. In addition, there was someone who spoke..., who interpreted, who was there, who knows me well, who knows where I come from. He knows the place, he knows my culture and everything.”
Participants also valued interpreters’ ability to help them articulate difficult subjects to the care providers.
"I can explain to him what I have. I speak French but I don't really speak, there are things I don't know in French. With him, I can explain and he can understand me. I don't know how to tell you. (...) Often, when I spoke with him in my language, when I explain it to him, the explanation he gives... If it had been me, it would not be the same explanation. He knows the French language well. He explains well, in fact. He explains well compared to me and I wouldn't have explained well like him."
For many, interpreters illustrated a bond with the native country, especially for UM who had not seen “anyone from the same country” since arriving in the host country.
“I am of Somalian origin and I am in France since I was little and also when I arrived I did not see Somalian people. So when I see the interpreter every time here it was a pleasure to see a person from the same country as me (...) I felt sometimes that I spoke the same language and all that sometimes I asked questions about my country because I was little when I left my country (...) [the interpreter spoke] about the cultures of the villages, all that, all that, all the things, the food to eat”
A support to caseworker-youth relationship
Some participants identified caseworkers as a reassuring support during sessions.
"In fact, at the consultation when I go there, when they send me to the consultation, but sometimes when I arrive at the consultation, when we speak, I don't really like it, so I let my caseworker talk, as I really trust her, when we speak. After that, that's when I can talk.”
However, for some participants, the caseworker’s continuous presence was perceived as intrusive and created a disincentive to talk, especially about very “personal” migratory life events. Some participants criticized the framework as too rigid, preferring to be “asked” if they consented to the caseworker’s presence during therapy.
Helpful interventions during MUCTUM therapy
Participants identified several helpful interventions during their follow-up.
Behavioral guidance promotes feelings of safety, self-confidence, and self-care practices
Participants valued education on coping skills and appropriate behaviors, especially during conflicts.
" I am someone, I get very, very angry. Even sometimes when I speak, I get angry very, very quickly. So Mrs. Y taught me and I'm learning to breathe and not to get angry very quickly. If someone comes to get me, I will try to speak calmly to these people, so as not to be very aggressive. (...) Once she finds that the situation is very hard, she tells me that I take a breath, I drink a glass of water, that it calms me down and then I speak again. Sometimes when I'm upset or sad, even when I'm at home, I take a drink of water and my throat feels better.”
Skills that participants cited included emotional regulation, relaxation methods (e.g. breathing exercises, drinking a glass of water), planning (e.g. writing to-do lists in a notebook), and reflection (e.g. “practicing speech in front of [a] mirror”). Participants who had experienced violence and detention also explained how the care providers’ explanations about security in France increased their feeling of safety:
“It didn't really go away but I evolved a lot on it because before, it was due to everything I had been through, I had the feeling that I was going to be found, no matter what. So that's a little bit of what fueled that feeling too... But then I was made to understand that this is France and all... I was reassured a lot by Mrs X and Dr. Y too and uh I started to let go a little bit, they made me understand that I wasn't going to be attacked overnight in the street... Or kidnapped and everything... So that kind of... calmed me down a bit…”
One participant explained that she continues to apply these negative affect regulation techniques now that she is a mother, which increases her self-confidence. “I worked [on] self-confidence a lot (…) and it is going very well”.
Care providers facilitate links with the other institutions
Care providers facilitate links with the other institutions caring for UM, particularly social workers, who facilitate support for the youth at Children’s Foster Home and school. Although some participants initially expressed displeasure at the presence of caseworkers in therapeutic sessions, most participants said that inclusion of their caseworker in MUCTUM unlocked communication and improved the relationship with the caseworker.
"I was the one who was really struggling and uh it was really really um... The follow-up that allowed us to tighten up.... Strengthening the ties, no but... Allowed me to have… uh… a discussion with [my caseworker] because having a discussion with her was not possible...
Researcher: Yes.
Participant: We couldn't understand each other at all.
Researcher: Yes.
Participant: Because here I was really saying everything I wanted to say and who I really was… [care providers] had the ability to transmit that to another person, so that the person could understand me too…
Researcher: Yes.
Participant : So uh, [my caseworker] had to go through them to understand how I functioned and me too how she functioned and sometimes we had big meetings where there were people and uh... It was partly thanks to them that I was able to establish a link with my caseworker...”
For others, MUCTUM provided a place to air discontents about their caseworkers, such as daily conflicts or misunderstandings. Some UM “felt bad” at the Children’s Foster Home, and shared that MUCTUM allowed them to express this opinion. Participants identified that the care providers could help the caseworkers learn how to navigate certain situations more effectively, such as one participant experiencing social withdrawal or mutism:
“Basically, you know as I said, basically, I didn't talk to anybody. So everybody was like, how do I talk to this individual? (...) So it was complicated for them... And in the end uh... (...) So, since there are certain things that I don't want to tell them about. So I invited them to come and participate in my sessions. That way, they will hear certain things. So, when we go back [home], [if] there are certain things that they don't (...) understand or that kind of thing, they call me, we talk about it, they ask me questions. And I answer, if I feel it... I answer. And so with that, it allows them to know how (...) to talk to me, how, how to handle the situation with me.”
In another example, one participant’s need for privacy due to his traumatic history was acknowledged, and he obtained access to an individual room. In addition to collaborating with the social workers, care providers use a problem solving approach to address social, educational and legal problems. One participant reported how care providers supported her to pursue her academic studies and advocated for her with social services. Another reported that he felt supported for minority recognition administrative procedures with his lawyer, to whom he “did not say everything” previously because of fear and uncertainty.
The work on family issues
Family issues were often discussed during therapy, such as the violent loss of parents, or the family relational difficulties that had led the UM to exile.
"There were problems with the family. My mother, who was not present, left us long ago. I was with my aunt and her children. Often it was not going well. That's why I left there. There is all that, we talked about all that too, with them."
In particular, participants valued phone calls and advice from the care team to family back home. In the case of one participant who had previously been sending money home due to being a victim of prostitution, care providers called the participant’s mother to explain that her daughter, now in school with no income, could no longer send money back home:
"I told all my stories to Mrs. X. In any case, she found some words. She called my mother to explain something to her. She made it clear that I don't work here, that I'm studying, that I won't have enough money, as much as she asks, that I won't be able to finance everything. So my mother, I don't know, but she has trouble understanding, my mother. She had a hard time."
This communication induced a change in parental expectations, which “relieves more and more” for adolescents seeking reassurance that it is okay to refuse to send money to over-demanding family members. For another participant, interpreters facilitated a conversation with the participant’s mother back in Somalia in order to restore family links, relationships, and childhood memories, which had been erased because of traumatic amnesia: “All my culture (…), when I was a child, lullabies, all this.” For this participant, finding her mother was a “huge relief” and allowed this adolescent to “reconnect to reality.” Now, the ability to call her mother frequently has “changed” and “energized” the participant: “It gave [me a] smile, me who was always sad.”
Cultural focus enables traditional care implementation
Cultural etiology and treatment were acknowledged and employed as needed, as cultural etiologies had variable importance for participants across the sample. Most participants did have representations of their conditions in their native culture (e.g. kénu in Soninke language, a certain conception of worry, or undusu, a “heart discomfort” in Malenke language), or explanations for certain phenomena (e.g. djodjo, witchcraft in Nigeria) and their cures. Some had no cultural hypothesis because they had left their country too young and their only solution was to “talk to my parents, and they will take care of me.” Other participants knew traditional etiological explanations, such as possession by spirits, like djinns, but associated djinns with problems more severe than their own. Participants also described various traditional treatments, specific to their home countries, including herbal treatments, massages, reading the Bible and listening to music, reading, and alms ("I buy stuff and give to the poor, give to people, and I ask God to protect me"). Some participants reported that their families in the native country recommended these traditional treatments, which they completed in France or their native country with the support of their MUCTUM care providers, such as prayers, alms, and sacrifices.
"I had a dream about an old man (…) I had to get out the alms and I managed to call my mother to do that alms and since then it's been fine."
Help with medications
Participants mentioned the value of medications, which reportedly helped with anxiety and sleep problems, but did not elaborate further on this topic.
“Before… I was awake… every hour… I tried to sleep at night but I couldn’t sleep… I had nightmares even if the door is open. I got out at night like people who walk at night, I sleep but I got out at the beginning. As I spoke to the psychologist and the psychiatrist, it stopped, I took medicine to sleep.
Researcher: Okay
Participant: And that stopped and even if I have a bad memory, a nightmare, well I still sleep but before I didn't sleep and all that.”
Narrating one’s story can “set us free” if carefully guided by care providersUM valued a delayed, progressive, and fractionated narration
Several participants said that the narration of their story at a slow pace was important, once a relationship of trust had been established with care providers. The narration was described as progressive, fractionated, prudent and non-forced:
"It was a little bit each session. Just a bit, a bit… and then the whole thing and that's it. It wasn't like 'you have to tell us what you've been through right away.'”
Participants appreciated the care providers' attention to preventing participants from sharing “too much” at once:
“If we manage to empty ourselves of this, in fact we empty our heads. When I was able to clear my past with Mrs. X, she found solutions, words and things that could calm me down. (...) They know their work well and they know very well that when it goes too far, they also know how to stop the person when it goes too far. So I like that.”
Consequently, narrating one’s history was not perceived as obligatory, and in fact some participants recalled relief at being explicitly asked not to talk about their story during early stages of therapy, because it was too painful.
“Participant: As I said earlier, I'm not someone who likes to re-explain that part.
Researcher: Yes
Participant: But afterwards, it was really a moment when you had to talk.
Researcher: Yes.
Participant: It was really. They gave me time, they let me... I think it took a year and a half before... That we really got into it. We only talked about myself, my fears, my mother. And then we really went through the process where ... well I had to explain my story to them and that was it…”
Narration encompassed both positive and negative life events: "I talked about my memories, times that went well and times that didn't go well, too." Some UM, on the contrary, did not narrate adverse life events: "I didn't tell my story to them." Narration was at times difficult for participants whose memories remained mostly “images” rather than easily-verbalized stories.
Care providers provide active, participative and empathetic listening to narration
Although this would seem self-evident for most practitioners, participants frequently and independently volunteered these reflections on providers' attitudes during narration of traumatic events, making it a notable theme in UM's experiences. Care providers were described as empathetic and non-judgmental, which contributed to trust and openness. Participants described how narration involved rephrasing by care providers, creating active, participative, and empathetic listening by care providers: "It was really like, ‘I experience the story with you. It helps you to let it go." Care providers with knowledge of the “sea crossing” helped participants feel understood, as did using “images” when they talked.
"Participant: It was very, very, very hard. Uh to say again what I… I had experienced, uh… You had to respect… and especially that they, when you explained, they illustrated for you.
Researcher: That is to say?
Participant: In itself... they take examples from you or do as if I tell them, for example, I crossed the sea: they tell you: by boat, the sea? Basically, to make you really live the thing, but in an intense way so that you can free yourself once and for all, and I think it was not bad for me anyway…
Researcher: Yes…
Participant: Because when I said uh when I took the example of Italy with the prostitution, really it was illustrated to me... And that was really what I wanted to say. So I was led to say what I had inside me without forcing myself.For example, a person can't understand your past, he's not in your shoes, but in fact, he tries to put himself in your shoes and all that, it feels good."
Care providers helped UM stop feeling guilty and provided explanations that helped participants “talk more openly.” Said one participant, "When I would say that when I was in Italy, I was prostituting, they would say, ‘yes, we know you were forced. How did this happen to you?’”.
Sharing one’s story is “painful” but “sets us free.”
Several participants mentioned a feeling of "liberation" in relation to the therapy, particularly through the ability to "talk."
"That's the hardest part. But once you get it all out, you feel good about your body. Plus, we open up to people and they give us ideas, advice on how to be able to deal with our past."
Sharing one’s story was experienced as “painful” ("it makes me sad,” brings back "weird memories") but provided relief and allowed care providers to find solutions. "It feels good to talk about the things that are in your heart. When you've told someone, it's like everything has gone from your heart." Narrating one’s story, though painful, reduced participants’ feeling of pain and loneliness.
"It hurt and at the same time, when I was talking, that's when I was able to work on it. When I was able to talk to people where at the same time it relieves my heart and it relieves me in my head."
It was often the first time they shared what they had endured with someone. “That way, at least someone knows.”










留言 (0)