
記住我










The results of the randomised placebo-controlled SENSCIS trial showed that in patients with systemic sclerosis-associated interstitial lung disease (SSc-ILD), nintedanib reduced the rate of decline in forced vital capacity (FVC) over 52 weeks.
WHAT THIS STUDY ADDSThe results of this open-label extension study show that the safety profile of nintedanib over longer term use was consistent with that seen in the SENSCIS trial and that the change in FVC over 52 weeks of the open-label extension was similar to that seen in patients who received nintedanib in SENSCIS.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICYIntroductionSystemic sclerosis is a heterogeneous autoimmune disease characterised by multiorgan vascular and fibrotic abnormalities.1 Interstitial lung disease (ILD) is a common manifestation of SSc, which most frequently develops early in the disease course.2 Systemic sclerosis-associated ILD (SSc-ILD) has a variable course and in some patients becomes progressive, characterised by an increase in fibrotic abnormalities on high-resolution CT (HRCT), a decline in forced vital capacity (FVC) and premature death.3 4 A decline in FVC in patients with SSc-ILD is predictive of mortality.3 5 6 There is no established algorithm to inform when pharmacotherapy for SSc-ILD should be initiated or which therapy should be used. Treatment decisions should be made on a case-by-case basis, taking into account the severity of ILD, risk factors for progression, other manifestations of SSc and the patient’s preferences.7 8
Nintedanib, a tyrosine kinase inhibitor with anti-inflammatory and antifibrotic properties,9 has been licensed for the treatment of SSc-ILD as well as for the treatment of idiopathic pulmonary fibrosis (IPF) and other chronic fibrosing ILDs with a progressive phenotype. The efficacy and safety of nintedanib in patients with SSc-ILD were investigated in the SENSCIS trial, in which patients were randomised to receive nintedanib or placebo until the last patient had reached week 52 but for a maximum of 100 weeks.10 Over 52 weeks, nintedanib reduced the rate of decline in FVC (mL/year) by 44% compared with placebo, with an adverse event profile characterised predominantly by gastrointestinal events, particularly diarrhoea. Data collected over the whole SENSCIS trial (up to 100 weeks of treatment) suggested that nintedanib provided a sustained benefit on slowing the progression of SSc-ILD over 100 weeks, with adverse events that were manageable for most patients.11 An open-label extension of SENSCIS, SENSCIS-ON, is assessing the safety and tolerability of nintedanib over the longer term. Exploratory data on FVC are also being collected. Here, we present data from the first year of SENSCIS-ON.
MethodsTrial designPatients in SENSCIS-ON (NCT03313180) came from two parent trials: SENSCIS (NCT02597933) and a drug–drug interaction (DDI) study (NCT03675581). SENSCIS enrolled patients with SSc-ILD with onset of first non-Raynaud symptom in the prior ≤7 years, extent of fibrotic ILD on HRCT ≥10% and FVC≥40% predicted.10 Patients receiving prednisone ≤10 mg/day or equivalent and/or stable therapy with mycophenolate or methotrexate for ≥6 months were allowed to participate. Patients were randomised to receive nintedanib 150 mg two times per day or placebo, stratified by antitopoisomerase I antibody status, until the last patient had reached week 52 but for ≤100 weeks. Patients who completed SENSCIS on treatment and attended a follow-up visit 28 days later were eligible to participate in SENSCIS-ON. Per protocol, the off-treatment period between SENSCIS and SENSCIS-ON was ≤12 weeks.
The DDI study from which patients could enter SENSCIS-ON was an open-label study of nintedanib plus oral contraceptive (Microgynon; ethinylestradiol and levonorgestrel) in female patients with SSc-ILD.12 Patients receiving prednisone ≤10 mg/day or equivalent and/or stable therapy with methotrexate for ≥6 months were allowed to participate. Treatment with mycophenolate ≤2 weeks prior to the start of the study was not permitted. Patients received nintedanib 150 mg two times per day over a period of ≥14 days to approximately 28 days. Per protocol, the off-treatment period between this study and SENSCIS-ON was ≤7 days.
In both SENSCIS and the DDI study, dose reductions to 100 mg two times per day were permitted to manage adverse events and dose could be increased back to 150 mg two times per day once the adverse event had resolved. Treatment could be interrupted for ≤4 weeks or ≤8 weeks to manage adverse events considered to be related to study drug, or not related to study drug, respectively. Patients receiving nintedanib or placebo at a dose of 150 mg two times per day at the end of the parent study received nintedanib 150 mg two times per day in SENSCIS-ON. Patients receiving nintedanib or placebo at a dose of 100 mg two times per day at the end of the parent study could receive nintedanib 100 mg two times per day or 150 mg two times per day in SENSCIS-ON. In SENSCIS-ON, nintedanib dose reductions from 150 mg two times per day to 100 mg two times per day were permitted, and treatment could be interrupted for ≤4 weeks or ≤12 weeks to manage adverse events considered to be related to study drug, or not related to study drug, respectively. FVC was assessed at baseline and at weeks 4, 12, 24, 36 and 52, using sponsor-supplied spirometers, in accordance with American Thoracic Society/European Respiratory Society guidelines.13 FVC measurements were centrally reviewed.
SENSCIS-ON is being carried out in compliance with the protocol and in accordance with the principles of the Declaration of Helsinki, the International Council for Harmonisation Harmonised Tripartite Guideline for Good Clinical Practice, applicable regulatory requirements and standard operating procedures. Patients provided written informed consent prior to entry into the trial.
Exclusion criteriaPatients with aspartate aminotransferase or alanine aminotransferase >3 times the upper limit of normal (ULN) or bilirubin >2 times the ULN were excluded from SENSCIS-ON, as were patients at risk of bleeding and patients with major thromboembolic events following completion of the parent trial. A complete list of the exclusion criteria is provided in the supplemental material.
EndpointsAdverse events, reported irrespective of causality, with onset from the first drug intake to week 52 (or to the last drug intake plus 7 days for patients who prematurely discontinued treatment) were coded using the Medical Dictionary for Regulatory Activities V.22.1. Serious adverse events were defined as adverse events that resulted in death, were life threatening, resulted in hospitalisation or prolongation of hospitalisation, resulted in persistent or clinically significant disability or incapacity, were a congenital anomaly or birth defect or were deemed serious for any other reason. Recommendations for the management of diarrhoea and liver enzyme elevations were provided to the investigators.14 Efficacy endpoints assessed at week 52 included absolute change from baseline in FVC (mL); the proportions of patients with relative categorical increase and decline in FVC (mL); the cumulative distribution of patients by absolute change from baseline in FVC % predicted; and changes from baseline in the modified Rodnan skin score (mRSS), St. George’s Respiratory Questionnaire (SGRQ) total score and University of California Los Angeles (UCLA) Scleroderma Clinical Trial Consortium Gastrointestinal Tract (UCLA SCTC GIT) V.2.0 instrument total score. The mRSS measures skin thickness based on palpation of 17 areas, each rated on a scale of 0–3, with higher scores indicating worse skin thickening.15 The SGRQ is a measure of health-related quality of life (HRQL) in patients with respiratory diseases and comprises three domains: impact, symptoms and activity.16 Each domain score and the total score are scaled from 0 to 100, with higher scores indicating worse HRQL. The UCLA SCTC GIT instrument V.2.0 comprises seven scales measuring the severity and impact of gastrointestinal symptoms: reflux, distension or bloating, faecal soilage, diarrhoea, constipation, emotional well-being, social functioning.17 Each scale is scored from 0 to 3 except for diarrhoea (0 to 2) and constipation (0 to 2.5). The total score, derived as the mean of the scores for the scales except constipation, ranges from 0 to 2.83, with higher scores indicating worse symptoms.
AnalysesAnalyses were conducted in patients who had received nintedanib in SENSCIS and continued nintedanib in SENSCIS-ON (‘continued nintedanib’ group), and in patients who had received placebo in SENSCIS and initiated nintedanib in SENSCIS-ON or who had received nintedanib for a brief period in the DDI study (‘initiated nintedanib’ group). All analyses were descriptive and conducted in patients who received ≥1 dose of trial medication. Changes from baseline in each endpoint were based on observed data available at the respective time point. The cumulative distribution of patients by absolute change from baseline in FVC % predicted was determined post hoc based on the worst observation carried forward method. In post hoc analyses, adverse events and absolute change from baseline in FVC (mL) at week 52 were analysed in subgroups by mycophenolate use at the start of SENSCIS-ON.
ResultsPatientsOf the 473 patients who completed SENSCIS (n=456) or the DDI study (n=17) on treatment, 444 (93.9%) entered SENSCIS-ON. There were 197 patients in the continued nintedanib group and 247 patients (231 from SENSCIS, 16 from the DDI study) in the initiated nintedanib group. Baseline characteristics at entry into SENSCIS-ON were generally similar between patients who continued and initiated nintedanib (table 1). The majority of patients were women (75.5%) and white (69.4%); mean (SD) FVC at baseline was 70.6 (18.0) % predicted; 232 patients (52.3%) were taking mycophenolate. Baseline characteristics at entry into SENSCIS-ON in subgroups by mycophenolate use are shown in online supplemental table S1. In the continued nintedanib and initiated nintedanib groups, respectively, 13 (6.6%) and 51 (20.6%) patients permanently discontinued nintedanib before week 52 (figure 1).
 Figure 1
Figure 1 Disposition of patients in SENSCIS-ON.
Table 1Baseline characteristics of patients at inclusion in SENSCIS-ON
ExposureDue to the trial design, the patients rolled over from SENSCIS into SENSCIS-ON had received different exposures to trial drug in SENSCIS (52–100 weeks). The median (minimum and maximum) off-treatment period between SENSCIS and SENSCIS-ON was 44 (26 and 88) days in patients who continued nintedanib in SENSCIS-ON and 49 (24 and 140) days in patients who initiated nintedanib in SENSCIS-ON. The median (minimum and maximum) off-treatment period between the DDI study and SENSCIS-ON was 8 (6 and 37) days. Median (minimum and maximum) exposure over 52 weeks in SENSCIS-ON was 13.8 (0.2, 13.8) months in the continued nintedanib group and 13.8 (0.0 and 13.8) months in the initiated nintedanib group. Total median (minimum and maximum) exposure to nintedanib across both SENSCIS and SENSCIS-ON was 29.5 (12.8 and 37.0) months. Among those in the continued nintedanib group, 54 patients (27.4%) had >36 months’ exposure to nintedanib across both SENSCIS and SENSCIS-ON.
Adverse events and dose adjustmentsAdverse events are shown in table 2. Diarrhoea was the most frequent adverse event, reported in 134 patients (68.0%) who continued nintedanib and 170 patients (68.8%) who initiated nintedanib. In the continued nintedanib and initiated nintedanib groups, respectively, the worst diarrhoea event was mild or moderate in intensity in 99.3% and 95.3% of the patients who had diarrhoea. Among patients who experienced diarrhoea, 3 (2.2%) and 17 (10.0%) patients who continued and initiated nintedanib, respectively, permanently discontinued nintedanib due to diarrhoea. Liver test abnormalities were reported in 22 (11.2%) and 48 (19.4%) patients who continued and initiated nintedanib, respectively. Bleeding and cardiovascular adverse events are summarised in online supplemental table S2.
Table 2Adverse events (reported irrespective of causality) in SENSCIS and SENSCIS-ON
Serious adverse events were reported in 42 (21.3%) and 60 (24.3%) patients in the continued nintedanib and initiated nintedanib groups, respectively. The most frequent serious adverse event was pneumonia, reported in 8 (4.1%) and 4 (1.6%) patients who continued and initiated nintedanib, respectively (online supplemental table S3). The adverse event profile of nintedanib was generally similar in subgroups by mycophenolate use at the start of SENSCIS-ON (online supplemental table S4). Among patients who continued nintedanib, upper respiratory tract infections were more frequent (17.1% vs 9.8%) and vomiting less frequent (10.5% vs 17.4%) in the subgroup taking mycophenolate. Among patients who initiated nintedanib, nasopharyngitis was less frequent in patients taking mycophenolate (10.2% vs 16.7%). Cough was more frequent in the subgroup taking mycophenolate both among those who continued (15.2% vs 8.7%) and initiated (11.8% vs 5.0%) nintedanib. Liver test abnormalities were less frequent in patients taking mycophenolate both among those who continued (3.8% vs 19.6%) and initiated (13.4% vs 25.8%) nintedanib.
Among patients who continued and initiated nintedanib in SENSCIS-ON, respectively, 36 (18.3%) and 122 (49.4%) had≥1 dose reduction and 55 (27.9%) and 104 (42.1%) had ≥1 treatment interruption. Among those who had ≥1 dose reduction, nine patients (25.0%) in the continued nintedanib group and eight patients (6.6%) in the initiated nintedanib group had ≥1 dose increase to 150 mg two times per day. Adverse events led to permanent discontinuation of nintedanib in nine patients (4.6%) who continued nintedanib and 53 patients (21.5%) who initiated nintedanib.
Forced vital capacityIn total, 176 (89.3%) and 171 (69.2%) patients in the continued nintedanib and initiated nintedanib groups, respectively, had FVC data available at baseline and week 52. Mean (SE) changes in FVC from baseline to week 52 of SENSCIS-ON were −58.3 (15.5) mL in patients who continued nintedanib, −44.0 (16.2) mL in patients who initiated nintedanib and −51.3 (11.2) mL in all patients (figure 2). Changes in FVC over time in patients who continued and initiated nintedanib in SENSCIS-ON are shown in figure 3. Changes in FVC over time in SENSCIS and SENSCIS-ON are shown together in online supplemental figure S1. Changes in FVC over time based on pooled data from SENSCIS and SENSCIS-ON are shown in figure 4.
 Figure 2
Figure 2 Change from baseline in FVC (mL) at week 52 in SENSCIS and SENSCIS-ON. Changes were based on data from patients with available data at baseline and at week 52. FVC, forced vital capacity.
 Figure 3
Figure 3 Absolute change from baseline in FVC (mL) over time in SENSCIS-ON. Baseline was the last measurement on or before the date of first trial drug intake in SENSCIS-ON. FVC, forced vital capacity.
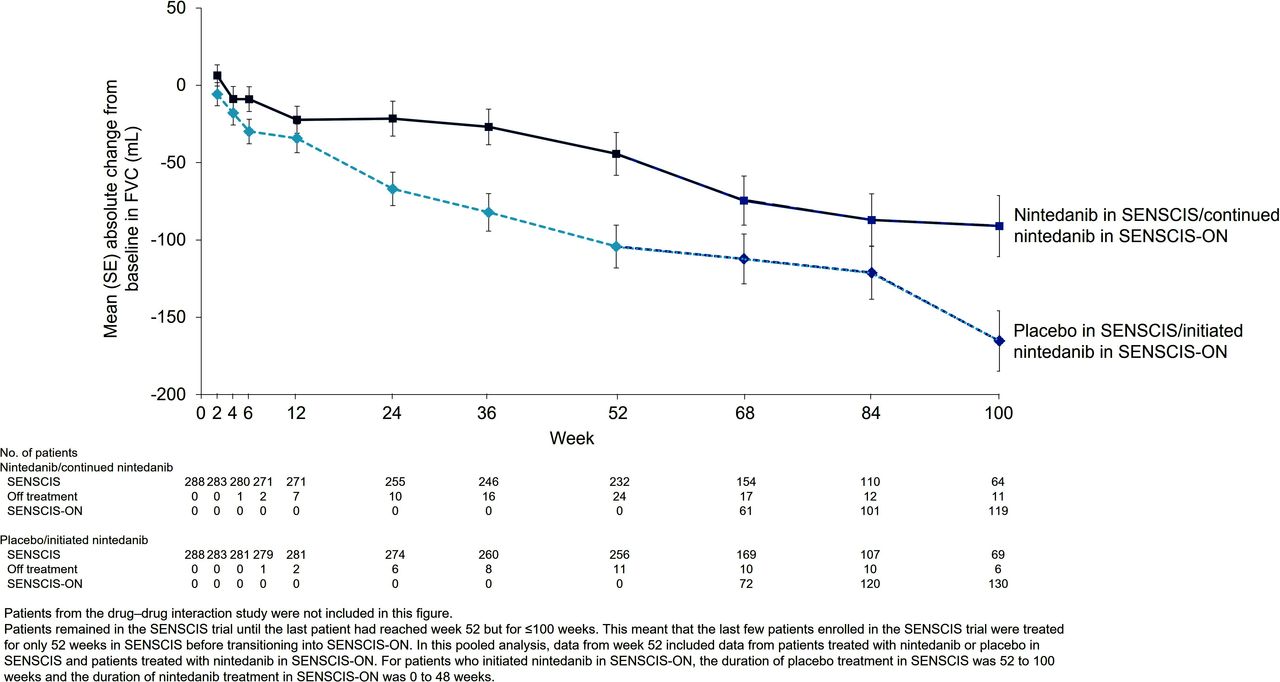
As patients remained in the SENSCIS trial until the last patient had reached week 52, the last few patients enrolled were treated for only 52 weeks in SENSCIS before transitioning into SENSCIS-ON. Thus, in the pooled analysis of changes in FVC over time, data after week 52 included data from patients treated with nintedanib or placebo in SENSCIS and patients treated with nintedanib in SENSCIS-ON. Of the patients who had FVC data available at baseline and at week 52, 13.6% of patients who continued nintedanib and 17.0% of patients who initiated nintedanib had an improvement in FVC (mL) ≥5% between baseline and week 52 of SENSCIS-ON (figure 5). A relative decline in FVC (mL) of >5% from baseline to week 52 of SENSCIS-ON was observed in 38.6% of patients who continued nintedanib and 29.2% of patients who initiated nintedanib; a relative decline in FVC (mL) of >10% occurred in 17.6% of patients who continued nintedanib and 12.9% of patients who initiated nintedanib. The cumulative distribution of patients by absolute change in FVC % predicted from baseline to week 52 of SENSCIS-ON is shown in online supplemental figure S2. Mean (SE) changes in FVC in subgroups by mycophenolate use at the start of SENSCIS-ON are shown in online supplemental figure S3.
 Figure 5
Figure 5 Proportions of patients with relative increases and declines in FVC (mL) from baseline to week 52 of SENSCIS-ON. Percentages were calculated using the number of patients with available data at baseline and at week 52 as the denominator. FVC, forced vital capacity.
mRSS, SGRQ and UCLA SCTC GIT instrumentMean (SE) change from baseline in mRSS at week 52 was −0.9 (0.2) in the continued nintedanib group (n=180) and −1.0 (0.3) in the initiated nintedanib group (n=174).
Mean (SE) change from baseline in SGRQ total score was 1.37 (0.87) in the continued nintedanib group (n=177) and −0.31 (0.91) in the initiated nintedanib group (n=183).
Mean (SE) change from baseline in UCLA SCTC GIT instrument total score was 0.28 (0.03) in the continued nintedanib group (n=168) and 0.18 (0.03) in the initiated nintedanib group (n=162).
DiscussionData from 52 weeks’ follow-up in SENSCIS-ON showed that the adverse event profile of nintedanib over longer term use was consistent with that reported over 52 weeks in SENSCIS.10 14 Among patients who initiated nintedanib in SENSCIS-ON, the proportions of patients who had a dose reduction or treatment interruption to manage adverse events over 52 weeks were similar to those observed in the nintedanib group of SENSCIS.14 These dose adjustments were less frequent among the patients who continued nintedanib in SENSCIS-ON. Permanent discontinuations of nintedanib due to adverse events were also less frequent among patients who continued nintedanib in SENSCIS-ON than among those who initiated nintedanib in SENSCIS-ON or took nintedanib in SENSCIS. It is unclear whether the lower frequency of dose adjustments and discontinuations in the patients who continued nintedanib in SENSCIS-ON simply reflects that patients who were better able to tolerate the drug were more likely to have entered and continued in the trial, or whether there is improved tolerance to nintedanib with longer-term use.
Diarrhoea has consistently been shown to be the most frequent side effect of nintedanib in patients with ILDs.10 18 Mild or moderate diarrhoea was the most frequently reported adverse event in SENSCIS-ON. Among patients who initiated nintedanib in SENSCIS-ON, 6.9% discontinued nintedanib due to diarrhoea over 52 weeks, consistent with the rate observed in patients who initiated nintedanib in SENSCIS. Discontinuation of nintedanib due to diarrhoea was less frequent among patients who continued nintedanib in SENSCIS-ON (1.5% over 52 weeks). Mean scores on the UCLA SCTC GIT instrument in both the continued nintedanib and initiated nintedanib groups suggested that most patients had no or mild gastrointestinal symptoms at the start of SENSCIS-ON.17 A small worsening in mean UCLA SCTC GIT instrument total score was observed over 52 weeks. The adverse event profile of nintedanib was generally similar in patients who used nintedanib alone and in combination with mycophenolate, although the proportion of patients who had cough was higher in patients taking than not taking mycophenolate. This is consistent with the product label for mycophenolate, which reports cough as a side effect.
The change in FVC over 52 weeks of SENSCIS-ON was similar to the change in FVC over 52 weeks in the nintedanib group of SENSCIS (−51.3 and −42.7 mL, respectively) and much smaller than the change in FVC over 52 weeks in the placebo group of SENSCIS (−104.8 mL). Similar proportions of nintedanib-treated patients in SENSCIS and SENSCIS-ON had a decline in FVC from baseline of >5% and >10% over 52 weeks. These data, which suggest a sustained benefit of nintedanib on slowing the progression of SSc-ILD, are supported by data from the open-label extension of the INPULSIS trials, which suggested that the effect of nintedanib on slowing the progression of IPF persisted beyond 4 years.19 The reduction in the rate of FVC decline provided by nintedanib in patients with SSc-ILD may be regarded as clinically meaningful given the disease trajectory and the known association between FVC decline and mortality in patients with SSc-ILD3 5 6 and other ILDs.20–22 Although the SENSCIS and SENSCIS-ON trials were not designed to investigate the effects of combination therapy, we note that the smallest decline in FVC over 52 weeks of SENSCIS-ON occurred in patients receiving both nintedanib and mycophenolate, consistent with observations in the SENSCIS trial.23 Changes in the SGRQ total score in SENSCIS-ON were small, consistent with observations from SENSCIS10 and from the INPULSIS trials in patients with IPF,24 suggesting that the changes in FVC in SENSCIS-ON were not associated with a significant deterioration in respiratory symptoms.
Strengths of our analyses include the large cohort of patients who participated in SENSCIS-ON and the standardised collection of FVC measurements. About half of the patients who entered SENSCIS-ON were taking mycophenolate, increasing the relevance of our findings to clinical practice. Limitations of our analyses include the lack of a placebo group and the gradual loss of patients over the course of the trial. There may be selection bias among the patients who opted to participate in SENSCIS-ON, that is, these patients may have had fewer adverse events or better lung function; however, over 90% of patients who completed SENSCIS on treatment opted to participate in SENSCIS-ON. Although patients who participated in SENSCIS-ON were grouped according to their prior treatment, these are not randomised groups in SENSCIS-ON, so direct comparisons between patients who continued and initiated nintedanib should be approached with caution.
In conclusion, these data suggest that continued treatment with nintedanib, up to 3 years in duration, had a manageable safety and tolerability profile in patients with SSc-ILD. The adverse event profile of nintedanib over 52 weeks in SENSCIS-ON was consistent with that reported over the 52 weeks of initial use in SENSCIS. The change in FVC in patients who received nintedanib over 52 weeks of SENSCIS-ON was similar to the change in FVC in patients who received nintedanib over 52 weeks in SENSCIS. These findings are consistent with a sustained clinically meaningful benefit of nintedanib in slowing the progression of SSc-ILD and support the prompt initiation of nintedanib in patients with SSc and pulmonary fibrosis.
Data availability statementData are available upon reasonable request (see online supplementary material).
Ethics statementsPatient consent for publicationEthics approvalThe protocol was approved by an Ethics Committee or Institutional Review Board at all the participating centres (listed in the supplemental material). Participants gave informed consent to participate in the study before taking part.
AcknowledgmentsThe authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE). The authors did not receive payment for development of this manuscript. Julie Fleming and Wendy Morris of FleishmanHillard, London, UK, provided medical writing assistance, which was contracted and funded by BI. BI was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
留言 (0)