
記住我
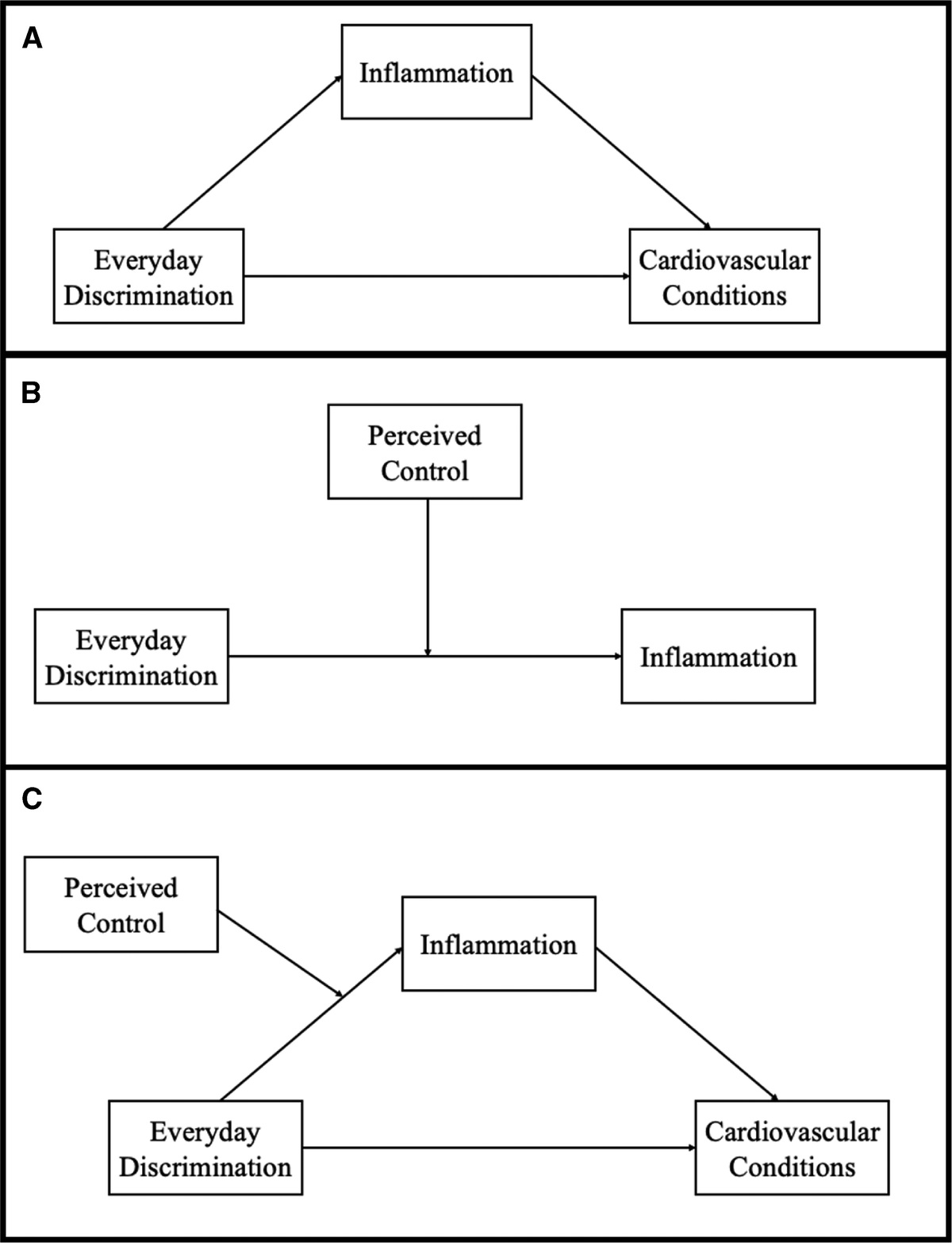
Effective antiretroviral therapy (ART) has changed the face of the human immunodeficiency virus (HIV) epidemic from a disease with increased mortality to a manageable chronic condition. According to the Centers for Disease Control and Prevention, by 2015, more than 50% of people with HIV (PWH) in the United States were 50 years or older, and in 2020, that number was expected to have increased to 70% (1,2). Consequently, the “graying of the HIV epidemic” has led to new challenges including elevated incidence of comorbidities traditionally associated with chronic stress exposure such as cardiovascular disease, type 2 diabetes, cancer, and neuropsychiatric complications (3,4). PWH are exposed to a higher-than-average stressor burden, and the degree of stress-related comorbidities exceeds similar comorbidities observed in other chronic illnesses (5–8). Perceived stigma has been linked to decreased quality of life among PWH (9), and women living with HIV report higher psychological distress (10). Furthermore, stress-related disorders increase threefold to fourfold after HIV diagnosis among women (11). In addition to the impact of psychosocial stressors, HIV may directly impact the stress response systems. Cytokines from viral infections stimulate the hypothalamic-pituitary-adrenal (HPA) axis and alter function of cortisol (12). Finally, evidence suggests that PWH have impaired coordination between the immune system and the HPA axis, particularly in women (13). Together, data suggest that HIV uniquely impacts stress physiology.
The glucocorticoid (GC) receptor (GCR) is a prime candidate as a mediator of stress-related diseases and disorders and may be modified by HIV. GCRs are present on nearly every cell in the body and are stimulated by GCs, primarily cortisol in humans. Cortisol is released as the culminating step of activation of the HPA axis, which is engaged daily as part of the circadian rhythm, and robustly activated during responses to physical or psychological stressors. The GCR is both a receptor and a transcription factor. Therefore, stimulation of the GCR produces a robust cascade of changes that are primarily centered on the mobilization of resources to cope with the energetic demands created by the stress response. In addition to functions in the regulation of metabolic processes, the GCR also has potent anti-inflammatory effects through primary changes in gene expression and transrepression of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), a prominent proinflammatory transcription factor. Interactions between the GCR and immune mediators, such as NF-κB, position the GCR as both a potential mechanism of HIV-associated chronic inflammation and a potential biomarker of progression toward inflammation-related comorbidities such as cognitive impairment (14) and related impairments in everyday functioning (15–18). Furthermore, previous studies in animal models demonstrate that HIV-related proteins can independently alter function of the HPA axis and precipitate changes in affective-like behaviors and cognition (19,20).
Previous efforts to examine the role of stress and alterations in stress biology in HIV-associated comorbidities have primarily focused on cortisol and have yielded disparate and equivocal results (21–24). Viruses are known to increase activation of the HPA axis (12,25), which may further limit the interpretation of the overall impact of HIV by the singular metric of circulating cortisol. Although cortisol measurements are an accurate assessment of circulating steroid concentrations, they provide limited information on GCR function. As is the case with many steroids and their associated receptors, the function of cortisol is heavily regulated by binding globulins, chaperones, and co-chaperones. Because of these additional levels of regulation, concentration alone does not necessarily reflect function.
GCR co-chaperones, in particular, FKBP5, are essential for GCR function and can directly alter GCR sensitivity and action (26). FKBP5 harbors the GCR in the cytosol of the cell, effectively acting as a negative regulator of GC function. Alterations in FKBP5 are associated with cognitive impairment and altered stress responsivity. For example, in psychiatric disorders, FKBP5 gene expression is related to memory and function of the hippocampus and prefrontal cortex (27,28). In rodents, increased FKBP5 is related to reduced GCR translocation and reduced GCR-DNA binding that in turn is associated with memory impairments (29). Translating that basic science evidence to humans, impaired GCR function could predispose women with HIV (WWH) to cognitive impairment linked to GC resistance defined as reduced efficacy of GCR stimulation. FKBP5 is altered in postmortem brains of PWH (30,31), but neither the impact of HIV on FKBP5 in peripheral cells nor the potential predictive value of subthreshold changes in FKBP5 and GCR function has been considered as an underlying mechanism of cognitive function.
HIV seems to interact with/or accelerate age-related inflammation (32) and possibly exacerbate neuroinflammation within the brain (33). Given substantial sex differences in the immune response (34) and the dearth of neuroHIV studies focused on WWH (35–37), studies in this subgroup require particular attention. Identification of the mechanisms of HIV-associated chronic inflammation will provide the critical framework needed to design therapeutic strategies for the chronic inflammation that affects WWH and consequently may reduce comorbidities such as cognitive impairment that are associated with chronic inflammation (38).
Given that HIV infection and age may independently and synergistically perturb the function of the GCR, we examined the role of chronological aging and HIV serostatus on GCR function in peripheral blood mononuclear cells (PBMCs). We assessed ex vivo GCR function in three ways: a) assessment of co-chaperone expression as an indicator of potential GCR resistance, b) examination of expression of genes responsive to GCR stimulation as a metric of GCR response to ligand presentation, and c) assessment of the anti-inflammatory potential of the GCR. We first examined FKBP5 in PBMCs and hypothesized that aging and HIV would interact to associate with increased expression of FKBP5 beyond the independent effects of either HIV or aging. We then examined the stimulatory effects of dexamethasone (DEX) on GCR-mediated gene transcription. Given that FKBP5 inhibits translocation of the GCR to negatively regulate GCR transcriptional activity, we hypothesized that age and HIV would interact to attenuate the ability of DEX stimulation to engage GCR-mediated gene transcription. We tested this hypothesis by examining GCR-mediated gene transcription by measuring common genes controlled by the transcriptional activity of GCR: FKBP5, DUSP1, TSC22D3 (encodes for protein: GC-induced leucine zipper [GILZ]), and PER1. In addition, the anti-inflammatory capacity of GCR stimulation was examined by assessing the ability of DEX stimulation to block inflammatory signaling induced by the inflammatory stimulus lipopolysaccharide (LPS). The prefrontal cortex and hippocampus are particularly prominent sites of GCRs (39–43) and are critical components of neural circuitry underlying verbal and working memory (44,45). We therefore hypothesized that expression of FKBP5 would be more strongly associated with verbal and working memory difficulties in older WWH compared with younger WWH or HIV-uninfected (HIV−) younger or older women. Given the established role of the GC in the modulation of inflammation and in brain function, an understanding of the associations among HIV, age, and GCR function will provide insight regarding the degree to which GCR dysfunction could contribute to elevated inflammation and poorer cognitive function in WWH.
METHODS ParticipantsParticipants were enrolled in the Women’s Interagency HIV Study (WIHS), an ongoing longitudinal multisite cohort study of the natural and treated history of WWH and HIV− women. For this cross-sectional, nested case/control study, we used participants enrolled in the first three waves of the study who also completed baseline neuropsychological testing between 2009 and 2011. The waves of study enrollment occurred between October 1994 and November 1995, October 2001 and September 2002, and January 2011 and January 2013, from six sites (Brooklyn, Bronx, Chicago, DC, Los Angeles, and San Francisco). Detailed information regarding recruitment procedures, the core study protocol, and eligibility criteria have been previously published (46–48). All participants provided informed consent, and the WIHS Executive Committee approved the concept for this study.
To determine which cases were selected for analyses, our initial sampling frame was women with one neuropsychological assessment completed between 2009 and 2011 and stored biospecimens (PBMCs) collected and available for analysis concurrent with the neuropsychological assessment (n = 1595). Women (n = 382) were excluded from case selection for factors that can impact GCR function and/or cognition including: a) use of hormone-mediated contraceptives, pregnant, and/or breastfeeding within the past 6 months (49), d) self-reported use of antipsychotic or Alzheimer’s medication within the past 6 months (50), and/or c) current CD4 cell count <400 (51,52). From the remaining 1213 cases, 160 women were selected for the present study to yield four groups of women: a) older WWH (age >50 years), b) younger WWH (age <40 years), c) older HIV− women (age >50 years), and d) younger HIV− women (age <40 years). To balance the four groups on key variables, we first selected 40 older WWH then matched the other three groups as close as possible on key variables including age, race, and education. Because of cell viability, final sample sizes were n = 40 younger WWH, n = 38 older WWH, n = 39 younger HIV− women, and n = 38 older HIV− women.
GCR Function Cell CultureBlood was collected as part of a routine WIHS core visit. PBMCs were isolated and cryopreserved in the WIHS repository (Precision Bioservices, Rockville, Maryland). After concept approval by WIHS and sample selection (see the Participants section), PBMCs were shipped to Emory University, where they were maintained in liquid nitrogen until plated. Cells were thawed in an RPMI medium supplemented with 5% fetal bovine serum, 2 mM l-glutamine, and 10/10 pen/strep. Cell viability was confirmed with Trypan blue, and cells were counted and plated at a density of 1 × 106 cells/ml in 12-well cell culture plates (Corning Inc., Corning, New York; 2 × 106 cells/well total). Cell viability from this PBMC thawing protocol has a ~92% viability rate as measured by Trypan blue exclusion. After overnight incubation in a humidified atmosphere at 37°C in 5% CO2, the cells were stimulated with vehicle (baseline), DEX (Sigma Aldrich, product D-4902), LPS (Sigma Aldrich, product L2880), or concurrent LPS and DEX (LPS + DEX). DEX (concentration of 10−8 M) and/or LPS (concentration of 30 ng/ml) was added at 0 hours. Cells were harvested at 6 hours, centrifuged at 1000 rcf for 5 minutes at 4°C, and after a wash with ice-cold phosphate-buffered saline, the cell pellets were lysed for RNA extraction. Cell lysates and cell culture supernatant were stored at −80°C until they were used for RNA extraction and enzyme-linked immunosorbent assay (ELISA). Cell pellets from baseline and DEX conditions were used for quantitative polymerase chain reaction experiments, whereas cell culture supernatant from baseline, LPS, and LPS + DEX conditions were used for ELISA assessments.
Quantitative Polymerase Chain ReactionRNA was extracted from cell pellets using the RNeasy Mini Kit (Qiagen, Valencia, California) according to the manufacturer’s instructions. RNA integrity was assessed by a NanoDrop One spectrophotometer (ThermoScientific, Wilmington, Delaware), and RNA samples were reverse transcribed using the High Capacity RNA to cDNA Kit (Applied Biosystems, Foster City, California). To ensure uniform amounts of total cDNA across groups, cDNA was quantified via the PicoGreen Assay (Invitrogen, Carlsbad, California) and standardized throughout all samples. The human gene RPL13A was determined to be the optimal endogenous control based on an intergroup variance of less than 10% across groups. FKBP5 was selected for assessment given its established role in GCR resistance, cognition, and stress pathophysiology (19,26,28,49). DUSP1 (53,54), TSC22D3 (55,56), and PER1 (57,58) were selected because they are reliable indicators of GCR engagement. Primers for FKBP5 (forward: CTTGCTGCCTTTCTGAACCT, reverse: CCCTTGGCTGACTCAAACTC; protein: FKBP5), DUSP1 (forward: GATACGAAGCGTTTTCGGCT, reverse: GGGCCACCCTGATCGTAGA; protein: dual specificity phosphatase 1), TSC22D3 (forward: TGGTGGCCATAGACAACAAG, reverse: CTTCAGGGCTCAGACAGGAC; protein: GC-induced leucine zipper, GILZ), PER1 (forward: GGCAAGGACTCAGAAGGAAC, reverse: CTCCAGCTCCTCCAGGGTAT; protein: period circadian regulator 1), and RPL13A (forward: ATGCTGCCTCACAAGACCA, reverse: TAGGCTTCAGACGCACGAC; protein: ribosomal protein L13a) were designed and purchased from Applied Biosystems. The real-time polymerase chain reaction cycling conditions used on the QuantStudio Flex 6 (Applied Biosystems) were as follows: 50°C (2 minutes) and 95°C (2 minutes), followed by 40 cycles of 95°C (15 seconds) and 60°C (1 minute). Samples were run in triplicate and averaged, and the coefficient of variation (CV) within the triplicates was no more than 4%. Baseline gene expression data were calculated and presented as cycle of threshold (Ct) values normalized with regard to the endogenous control gene (RPL13A; formula: normalized Ct = [Ct of target gene] − [Ct of endogenous control]), with larger values indicating less gene expression because more cycles were necessary to amplify the gene to the threshold level. Post-DEX Ct values were calculated as [DEX normalized Ct] − [Baseline normalized Ct]. As the value reported approaches zero, this indicates less effective DEX stimulation of GC-related gene expression, with zero being indicative of no effect of DEX on GC function, as measured by GC-related gene expression.
Enzyme-Linked Immunosorbent AssayCytokine expression was assessed via ELISA in cell culture supernatant at baseline, after LPS (stimulated), and after LPS + DEX (suppression of LPS-stimulated cytokines by DEX) as additional indices of GC function. Human tumor necrosis factor α (TNF-α) ELISA kits were purchased from R&D Systems (Minneapolis, Minnesota), and assays were performed according to the manufacturer’s instructions. The sensitivity of the assay was 0.5 to 5.5 pg/ml, and the average intra-assay CV was 7.56% and the interassay CV was 12.01%. Samples were run in duplicates and averaged, and the CV among the duplicates was less than accepted cutoff of 15%. DEX suppression was calculated for each subject using the following equation:
[((TNFαfromLPScondition)−(TNFαfromLPS+DEXcondition))/(TNFαfromLPScondition)]×100
Neuropsychological FunctionAll women completed a comprehensive neuropsychological test battery between 2009 and 2011 and had available biospecimens for GCR function analysis. Neuropsychological domain assessments and outcome measures were as follows: verbal learning and memory, Hopkins Verbal Learning Test—Revised (outcomes = total words recalled across trials 1–3, delay free recall); attention/working memory, Letter-Number Sequencing (LNS; outcomes = total correct for experimental and control conditions); executive function, Trail Making Test Part B (outcome = time to completion) and Stroop Test Trial 3 (outcome = time to completion); psychomotor speed, Symbol Digit Modalities Test (outcome = total correct) and Stroop Trial 2 (outcome = time to completion); fluency, Letter (outcome = total correct words generated on F, A, S) and semantic (outcome = total correct animals generated); and motor skills, Grooved Pegboard (outcome = average time to complete dominant and nondominant hand). A log transformation was used on all timed outcomes to normalize distributions and then reverse scored so that higher scores equated to better performance across all domains.
Demographically adjusted T scores were derived for each outcome adjusting for age, years of education, Wide Range Achievement Test 3 (WRAT-3) reading subtest, race (African American versus not), ethnicity (Hispanic versus not), and number of times the test had been administered following methods used by other large-scale HIV cohorts including the WIHS (59,60). For each domain, a composite T score was derived by averaging the T scores for domains with at least two outcomes. If only one test in a domain was completed, the T score for that test was used. The primary outcome measures of interest were verbal memory and attention/working memory.
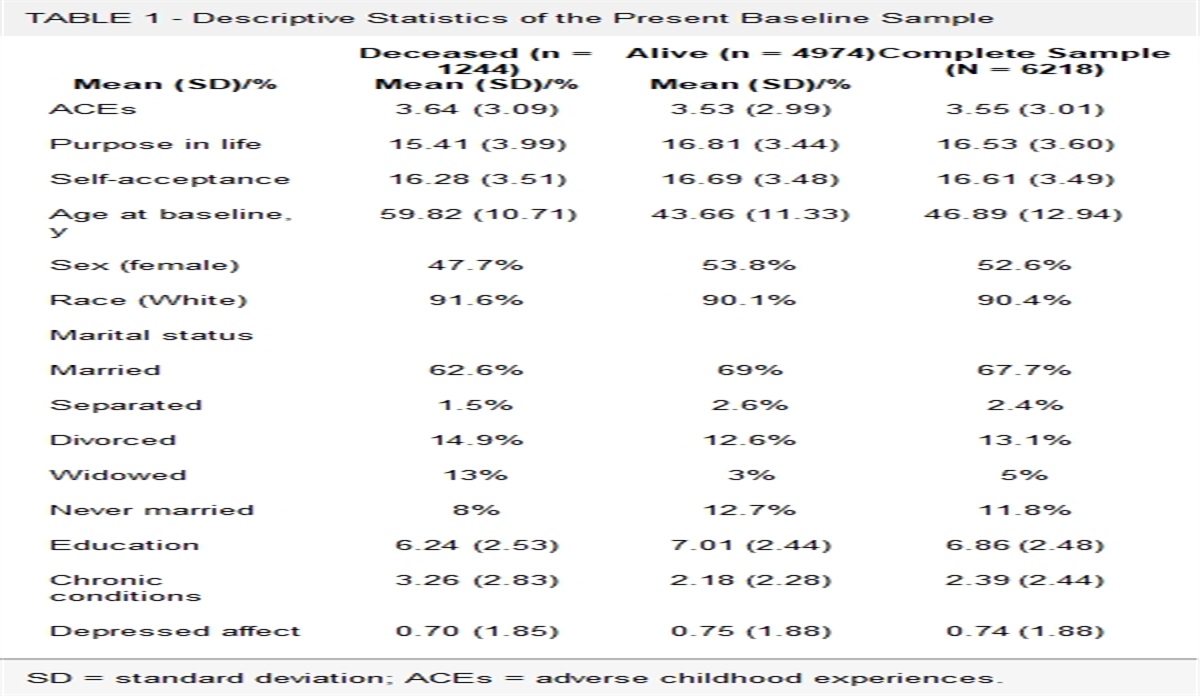
CovariatesCandidate covariates were based on our previous WIHS publications (selected a priori) (59,60) and are listed in Table 1. These variables (sociodemographic factors, clinical, and behavioral variables) have warranted consideration as covariates in analyses where we have examined cognition as a primary end point in the WIHS. Covariates included in all analyses were selected because they were associated with the independent (HIV, age) and dependent variables (cognitive outcomes) in univariate analyses at p < .20. All other variables did not shift our regression coefficients of interest and were not included as covariates in the model. The WRAT-3 reading subtest scores were not included as a covariate because this variable is accounted for in the cognitive domain–specific T scores. These variables included the following: depressive symptoms (Center for Epidemiological Studies Depression scale, ≥16 cutoff (61,62)); smoking status (current, former, never); heavy alcohol use (>7 drinks per week or >4 drinks in one sitting); crack, cocaine, and/or heroin use (ever, never); and recent antidepressant medication use. For analyses conducted in WWH only, the following HIV-related clinical characteristics were selected from a larger subset of factors (Table 1) and included the following: CD4 count, prior AIDS diagnosis, years on combination ART, and proportion of total WIHS visits that HIV RNA was undetectable.
TABLE 1 - Demographics and Other Descriptive Information About Study Participants as a Function of HIV Serostatus (WWH, HIV−) and Age (Younger, 50 Years) at Baseline Younger Older HIV− (n = 40) WWH (n = 39) p HIV− (n = 38) WWH (n = 38) p Age, M (SD), y 33 (4) 35 (3) .16 53 (3) 56 (5) <.001 Years of education, M (SD) 13 (2) 12 (3) .65 12 (3) 13 (2) .07 WRAT-3 reading subtest, M (SD) 97 (16) 93 (17) .30 86 (17) 95 (17) .04 Race/ethnicity, n (%) .48 .24 Black, non-Hispanic 22 (55) 27 (69) 25 (66) 19 (50) White, non-Hispanic 6 (15) 3 (8) 3 (8) 9 (24) Hispanic 6 (15) 6 (15) 9 (24) 8 (21) Other 6 (15) 3 (8) 1 (3) 2 (5) Annual household income ≤12,000/y, n (%) 15 (37) 10 (26) .26 18 (47) 14 (37) .35 Elevated depressive symptoms, n (%) 8 (20) 12 (31) .27 16 (42) 8 (21) .04 Antidepressant medication use 1 (2) 3 (8) .29 6 (16) 12 (31) .11 Hepatitis C RNA positive, n (%) 0 (0) 1 (2) .31 1 (3) 3 (8) .31 Smoking status, n (%) .11 .04 Current 15 (38) 9 (23) 15 (39) 11 (29) Former 17 (42) 14 (36) 19 (50) 14 (37) Never 8 (20) 16 (41) 4 (11) 13 (34) Recent heavy alcohol use, n (%) 14 (35) 9 (23) .25 12 (31) 3 (7) .01 Marijuana use, n (%) .007 .76 Recent 16 (40) 8 (20) 6 (16) 7 (18) Former 19 (47) 14 (36) 26 (68) 23 (60) Never 5 (13) 17 (44) 6 (16) 8 (21) Crack, cocaine, and/or heroin use, n (%) .02 .20 Recent 4 (10) 0 (0) 3 (8) 2 (5) Former 24 (60) 17 (44) 28 (74) 22 (58) Never 12 (30) 22 (56) 7 (18) 14 (37) HAART medication a — 28 (71) — 34 (89) Nadir CD4 count in WIHS, median (IQR) — 282 (201) — 223 (192) Current CD4 count, median (IQR) — 733 (336) — 820 (312) HIV RNA, Median (IQR) — 48 (2422) — 48 (27) Proportion of WIHS visits, M (SD) HIV RNA <500 copies/ml — 58 (31) — 54 (22) On HAART — 59 (33) — 60 (27) Adherence (≥95%) to ART, n (%) — 24 (80) — 30 (88) HAART duration, M (SD), y — 9 (4) — 10 (5) Previous AIDS diagnosis, n (%) — 7 (18) — 18 (47)HIV = human immunodeficiency virus; WWH = women with HIV; HIV− = HIV uninfected; M (SD) = mean (standard deviation); WRAT-3 = Wide Range Achievement Test standard score; HAART = highly active antiretroviral therapy; IQR = interquartile range; WIHS = Women’s Interagency HIV Study; ART = antiretroviral therapy.
Variables reported as n (%) were analyzed with χ2 tests. Variables reported as M (SD) were analyzed with analyses of variance. Variables reported as median (IQR) were analyzed with Wilcoxon-Mann-Whitney test. Column percents may not total to 100% because of rounding.
a Quantified over the three study visits; current refers to within the past week; recent, refers to within 6 months of the most recent WIHS visit; heavy alcohol use reflects >7 drinks a week or >4 drinks in one sitting.
For the first aim addressing the role of age and HIV serostatus on GCR function, we conducted a series of multivariable linear regression analyses. Predictor variables initially included in the model were as follows: age (younger, older), HIV serostatus (WWH, HIV−), and the two-way interaction. The two-way interaction was removed from the model if it was not significant (p > .05). Outcome variables included baseline FKBP5 expression levels, reporter gene expression after DEX (DUSP1, PER1, TSC22D3), and TNF-α after combined DEX + LPS. See the Covariates section for the covariates included in the models. For the second aim examining whether GCR function-cognition associations are moderated by HIV serostatus and age, we conducted a series of multivariable linear regressions (simple bivariate associations are included in Table S1, Supplemental Digital Content, https://links.lww.com/PSYMED/A864). Predictor variables included age, HIV serostatus, GCR function (baseline FKBP5 expression levels, reporter gene expression after DEX, or TNF-α after combined DEX + LPS), and the two- and three-way interactions. Unstandardized β (B) coefficients, standard errors (SEs), and p values were extracted from the models for interpretation of higher-order interactions. If higher-order interactions were not significant (p > .05), they were removed from the models. Outcome measures included the cognitive domain T scores. Primary outcomes included verbal memory and attention/working memory. All other cognitive domains were considered secondary outcomes. Covariates are listed in the Covariates section. Analyses were conducted in SAS version 9.4, and significance was set at p < .05 for all primary outcomes. A false discovery rate correction (Benjamini-Hochberg procedure) was applied for secondary outcome measures to adjust for multiple comparisons.
RESULTSTable 1 shows the participant characteristics as a function on HIV serostatus and age (younger, older). Among younger women, WWH and HIV-uninfected women were only found to differ on marijuana and crack, cocaine, and/or heroin use; HIV− women were more likely to use these illicit substances in the past 6 months compared with WWH. Among older women, WWH were slightly older (56 versus 53 years), had higher scores on the WRAT-3 reading subtest, had lower depressive symptoms, and were less likely to report heavy alcohol use or smoke.
Does HIV Infection or Age Independently or Synergistically Perturb Function of the GCR (Baseline Levels and Post-DEX Stimulation)? Baseline LevelsThe interaction between HIV serostatus and age on baseline FKBP5 expression levels was not significant (p = .94). After removing the two-way interaction from the model, HIV serostatus and age were also not independently associated with baseline FKBP5 expression levels (p values > .30; Figure 1A). The interaction between HIV serostatus and age was not significant on baseline TNF-α levels (p = .20; Table S2, Supplemental Digital Content, https://links.lww.com/PSYMED/A864). After removing the two-way interaction from the model, HIV serostatus (p = .07) and age (p = .98) were not associated with baseline TNF-α levels.
 FIGURE 1:
FIGURE 1: Baseline FKBP5 Ct value (A), TSC22D3 (GILZ) expression levels post-DEX (B). PER1 expression levels post-DEX (C). DUSP1 expression levels post-DEX (D), TNF-α baseline levels ((E), and TNF-α levels after LPS + DEX (F) as a function of HIV serostatus and age category (<40 and >50 years). Baseline gene expression data are presented as normalized cycle of threshold (C t) values, with larger values indicating less gene expression (A, B). Post-DEX C t values were calculated as [DEX normalized C t] − [Baseline normalized C t]. As the value reported on the y axis approaches zero, this indicates less effective DEX stimulation of GC-related gene expression, with zero being indicative of no effect of DEX on GC function, as measured by GC-related gene expression (C, D). DEX = dexamethasone; GC = glucocorticoid; HIV = human immunodeficiency virus; LPS = lipopolysaccharide; TNF-α = tumor necrosis factor α.
Post-DEX StimulationThere were no significant HIV serostatus by age interactions on DEX-stimulated expression of the genes regulated by the GCR or LPS-stimulated TNF-α levels (with or without DEX stimulation; p values > .13). After removing the two-way interaction from the models, HIV serostatus was associated with PER1 (p = .006) and DUSP1 (p = .02), but not TSC22D3 (p = .32) after DEX stimulation (Figures 1B–D). Specifically, PER1 and DUSP1 reporter gene inductions were lower in WWH compared with HIV-uninfected women irrespective of age. In addition, there was an age difference on TSC22D3 after DEX stimulation, with older women (mean = −2.87, SE = 0.1) having lower gene expression compared with younger women (mean = −3.0, SE = 0.1; p = .03), which remained significant after adjusting for depressive symptoms and other factors that differed between the older women. Age was not associated with DUSP1 (p = .06) or PER1 (p = .13).
Is the Association Between GCR Function and Cognition Modified by HIV Serostatus and Age? Baseline LevelsThe test of the primary hypothesis—the three-way HIV serostatus by age by baseline FKBP5 expression levels—was significant in the domain of attention/working memory (p = .009) but not in verbal memory after adjusting for confounding factors (p = .84; Table 2). This indicated that the magnitude of the association between baseline FKBP5 expression levels and attention/working memory varied as a function of HIV serostatus and age. Specifically, HIV serostatus significantly moderated the relationship between baseline FKBP5 expression and attention/working memory among older (p = .002) but not younger women (p = .53). Further interpretation of this interaction based on the B coefficients, SE, and p values from this single model revealed that, among older women, higher expression of baseline FKBP5 expression levels was associated with lower attention/working memory performance among WWH (B = 6.4, SE = 1.7, p = .0003) but not HIV-uninfected women (B = −1.7, SE = 1.9, p = .37; Figure 2). To ensure that the finding among older WWH was not driven by HIV-related clinical characteristics, we conducted a subanalysis among this group only. The association remained significant among older WWH after further adjusting for HIV-related clinical characteristics including current CD4 count, the proportion of virally suppressed visits in WIHS, and the number of years on combination ART (B = 7.1, SE = 1.9, p = .001). Exploratory analyses examining the pattern of performance for each outcome measure contributing to the attention/working memory domain indicated the same three-way interaction on the number correct for the working memory condition on LNS (p = .004) and missed statistical significance on the attention condition on LNS (p = .09). On verbal memory, there were no significant two-way interactions (HIV serostatus by baseline FKBP5 expression levels; age by baseline FKBP5 expression levels) or general associations between baseline FKBP5 expression levels and performance. On the secondary outcome measures (using the false discovery rate correction), there were no significant two- or three-way interactions or a significant association of baseline FKBP5 expression levels with performance.
TABLE 2 - Adjusted Association Between Baseline FKBP5 Expression and Cognition as a Function of HIV Serostatus (WWH, HIV−) and Age (Younger, 50 Years) Outcomes Younger Older HIV−, B (SE) WWH, B (SE) WWH Versus HIV−,
留言 (0)