
記住我










A 41-year-old gravidity 5/parity 3 (G5P3) woman presented with a 6 month history of intermittent vaginal spotting. Two months before consultation, she began having lower abdominal and pelvic pain and two episodes of postcoital bleeding. Although she had an abnormal pap smear 5 years previously, her most recent pap smear obtained 2 years prior to symptom onset was normal. After the second episode of postcoital bleeding, the patient consulted her gynecologist who performed a pap smear that was negative for intraepithelial lesion or malignancy but positive for human papillomavirus (HPV) 18. Pelvic examination revealed normal vaginal mucosa and an enlarged cervix with a 5 cm exophytic and necrotic nodular lesion along the cervical os. There was no vaginal or parametrial extension. Cervical biopsies and endocervical curettage were obtained.
Dr RamalingamEndocervical curettage showed a high grade neuroendocrine carcinoma, small cell type ( Figure 1A ). The tumor was composed of cells with a high nuclear to cytoplasmic ratio, molding and crush artifact with scattered mitotic figures, and apoptotic bodies ( Figure 1B ). Immunohistochemical stains showed that the tumor cells were positive for p16 (diffuse block-like staining) ( Figure 2A ), chromogranin ( Figure 2B ), synaptophysin ( Figure 2C ), and CD56, but negative for p40 and p63. In situ hybridization for high risk HPV was positive ( Figure 2D ). The morphology and immunophenotype were diagnostic of high grade neuroendocrine carcinoma, small cell type.
 Figure 1
Figure 1 (A) Small cell neuroendocrine carcinoma showing diffuse proliferation of small round blue cells. (B) High power images show tumor cells with a high nuclear to cytoplasmic ratio, molding and crush artifact with scattered mitotic figures, and apoptotic bodies.
 Figure 2
Figure 2 (A) Tumor cells were positive for p16 (diffuse block-like staining), (B) chromogranin, and (C) synaptophysin. (D) In situ hybridization for high risk human papillomavirus shows numerous positive signals.
Positron emission tomography–computed tomography (PET-CT) was performed to evaluate distant metastatic disease.
Dr BhosaleA subcentimeter left hilar node was seen, with a maximum standardized uptake value (SUV) of 5.4. There were multiple scattered pulmonary nodules, compatible with metastases. These were not metabolically avid. There was a 1×1 cm left upper lobe nodule with a maximum SUV of 6.9, a subcentimeter perivascular nodule posterior to the right hilum with a maximum SUV of 5.0, and another one with a maximum SUV of 4.8. The cervix was enlarged and intensely metabolically avid with a maximum SUV of 22.2, compatible with the known primary malignancy. There was a subcentimeter right obturator node, metabolically avid with a maximum SUV of 5.8, and a right common iliac node measuring approximately 1 cm with a maximum SUV of 11. There was no evidence of retroperitoneal adenopathy. ( Figure 3A,B)
 Figure 3
Figure 3 (A) Maximum intensity projection image shows a mass in the cervix (squiggly arrow) and pulmonary metastases and mediastinal lymphadenopathy (arrows). (B) Fused positron emission tomography–computed tomography image shows a mass in the cervix (*).
With the diagnosis of a small cell, International Federation of Gynecology and Obstetrics (FIGO) stage IVB cervical tumor, the recommendation was for chemotherapy with cisplatin (60 mg/m2 on day 1 every 3 weeks) and etoposide (100 mg/m2 on days 1–3) with re-evaluation after 3–4 cycles and a goal of six cycles if the patient could tolerate.
Dr Frumovitz: What is the Chemotherapy Regimen of Choice for this Patient? Is There Any Role for Immunotherapy in the Upfront Treatment Setting?Multiple guidelines, including those published by the National Comprehensive Cancer Network, Society of Gynecologic Oncology, and Gynecologic Cancer InterGroup, recommend platinum and etoposide for patients with metastatic (stage IVB) neuroendocrine cervical cancer. 1–3 We favor cisplatin and etoposide due to the well known sensitivity of cervical cancers to cisplatin. 3 Other providers prefer carboplatin and etoposide, which is likely reasonable. Currently, we do not recommend the addition of immunotherapy to platinum and etoposide regimens even though it is commonly used in patients with small cell lung cancer. In several studies, although the addition of immunotherapy improved overall survival, the clinical significance is debatable. For example, the IMPOWER-133 study, which compared platinum and etoposide with platinum, etoposide, and atezolizumab, showed statistically significant improvement in survival of 12.3 months in the atezolizumab group compared with 10.3 months in the control group. 4 The CASPIAN study compared platinum and etoposide with platinum, etoposide, and durvalumab and again showed a statistically significant improvement in survival from 10.3 to 13.0 months. 5 A third study, KEYNOTE-604, compared platinum and etoposide with platinum, etoposide, and pembrolizumab and reported a statistically significant improvement in survival from 9.7 to 10.8 months. 6 These very modest (<3 month) improvements in survival as well as the lack of data showing activity in neuroendocrine cervical cancer call into question the cost and toxicities of adding immunotherapy to upfront platinum and etoposide.
The patient tolerated four cycles of chemotherapy with the addition of pegfilgrastim from cycle 2 onward. A PET-CT scan and pelvic magnetic resonance imaging (MRI) were performed to evaluate response to rule out disease progression and to guide subsequent treatment strategy.
Dr BhosaleMultiplanar multisequence MRI of the pelvis was performed with and without intravenous administration of contrast. The previously seen 5.0 cm cervical mass had decreased in size. Although comparison with prior PET/CT was difficult, the endophytic cervical mass now measured 1.4×1.5×1.6 cm. No retroperitoneal or pelvic adenopathy was seen. There was normal appearance of the adrenal glands, and the kidneys were without hydronephrosis ( Figure 4A–C ). PET-CT showed complete response of all previous hilar and pulmonary nodes.
 Figure 4
Figure 4 (A) Post contrast T1 weighted sequence shows a mass in the endocervical region extending into the stroma (arrow). (B) Diffusion sequence shows a mass in the endocervix (*). (C) Sagittal T2 weighted sequence shows a mass in the cervix (arrow).
Images were discussed with the radiation oncologist and pelvic radiation (curative intent) with concurrent cisplatin and etoposide was recommended.
Dr Frumovitz: Can you Comment on the Role of Radiation Therapy With Curative Intent in Patients With Stage IVB Neuroendocrine Cervical Carcinoma?For patients with stage IVB metastatic disease, we typically start with systemic chemotherapy (cisplatin and etoposide). Surprisingly, 15–20% of patients with stage IVB disease will have resolution of their extra pelvic disease after 4–6 cycles. 7 For these patients, the addition of definitive chemoradiation improves progression free survival and overall survival. For patients who have received six cycles of platinum and etoposide at this point, we typically proceed with cisplatin as a radiosensitizer. For those, like this patient, who have only received four cycles of platinum and etoposide, we would continue both drugs with radiation to complete six cycles. In a retrospective study, women with stage IVB disease who had resolution of extrapelvic disease with chemotherapy and then underwent definitive chemoradiation had an overall survival of 20.3 months compared with 13.6 months for those women who did not receive chemoradiation (p=0.001). In addition, 25% of the cohort that received chemoradiation had an overall survival of >5 years and 20% had not recurred with a minimum follow-up of 8 years.7
A PET scan and pelvic MRI performed after completion of the primary treatment (chemotherapy and pelvic radiation) showed no evidence of local or distant disease.
Dr Frumovitz: On Completion of Therapy, is There Any Role for Maintenance Therapy? What is the Best Image Study for Patient Surveillance, PET-CT or CT-scan?Currently, we are not recommending maintenance therapy in patients who have a complete response. In patients with metastatic small cell lung cancer who did not progress with primary chemotherapy, the CHECKMATE-451 study evaluated immunotherapy maintenance. Maintenance with immunotherapies showed a statistically significant but clinically very modest improvement in progression free survival. Maintenance with the combination of ipilimumab and nivolumab resulted in a progression free survival of 1.7 months compared with 1.9 months for nivolumab maintenance alone and a progression free survival of 1.4 months for placebo. 8 However, there was no improvement in overall survival (9.2 months vs 10.4 months vs 9.6 months) or survival at 1 year (41% vs 44% vs 40%).
Our standard for surveillance in patients who have had a complete response is physical examination and PET/CT scan every 3 months in the first year, every 4 months in the second year, and every 6 months in years 3–5. After 5 years some patients are hesitant to forego examinations and imaging, and for those patients we will often continue. We prefer the combination PET/CT scans over CT scans as we consider additional valuable information is garnered from the PET portion; however, at this time, we do not have objective data to support this notion.
Unfortunately, a CT scan of the chest abdomen and pelvis at 6 months after completion of primary treatment showed recurrent disease.
Dr BhosaleThere was interval development of multiple small low attenuation lesions in both lobes of the liver suspected of metastatic disease. A representative lesion in the left liver measured 1.2 cm. A lesion in the right liver measured 1 cm. Other lesions in the liver were noted but these were subcentimeter in size. The chest, spleen, pancreas, adrenal glands, and kidneys were unremarkable. No locally recurrent masses were identified in the pelvis.
The patient underwent a liver biopsy confirming recurrent metastatic small cell carcinoma.
Dr Frumovitz: What Should be the Standard Evaluation at the Time of Recurrence for a Patient With Neuroendocrine Tumor?For patients who recur, we perform a history and physical, including a pelvic examination. Assessment of performance status is important for treatment planning, especially if a clinical trial is being considered. For patients with liver and/or lung disease at recurrence, we will often obtain imaging of the brain as there may be occult disease. We will also do imaging of the brain if the patient is having any neurologic symptoms. Finally, we typically order programed cell death ligand 1 (PD-L1), microsatellite instability, and molecular testing to assess for tumor mutations in an effort to expand treatment options with targeted therapies, most frequently with clinical trials, but occasionally with off-label prescription of drugs approved by the US Food and Drug Administration.9 10
A CT scan of the brain showed no evidence of metastatic disease. Solid tumor genomic test was performed using biopsy tissue with no detected mutations noted. DNA microsatellite instability analyses (polymerase chain reaction based method evaluating a panel of seven microsatellite markers: BAT25, BAT26, BAT40, D2S123, D5S346, D17S250, and TGFBR2) showed a microsatellite stable tumor. PD-L1 immunohistochemistry showed a combined positive score of <1. The patient was started on topotecan (0.75 mg/m2 on days 1–3), paclitaxel (175 mg/m2 on day 1), and bevacizumab (15 mg/kg on day 1) every 21 days. A CT scam was ordered every three cycles showing almost complete resolution of disease after cycle 9.
Dr BhosaleCT of the chest, abdomen, and pelvis with intravenous contrast after three cycles showed a partial response with a previously identified lesion in the left liver measuring 0.8 cm compared with 1.2 cm. A lesion in the right liver measured 0.7 cm (compared with 1 cm previously. Other subcentimeter lesions were barely perceptible. No recurrent masses were seen in the pelvis. Post radiation changes were identified (Figure 5A ).
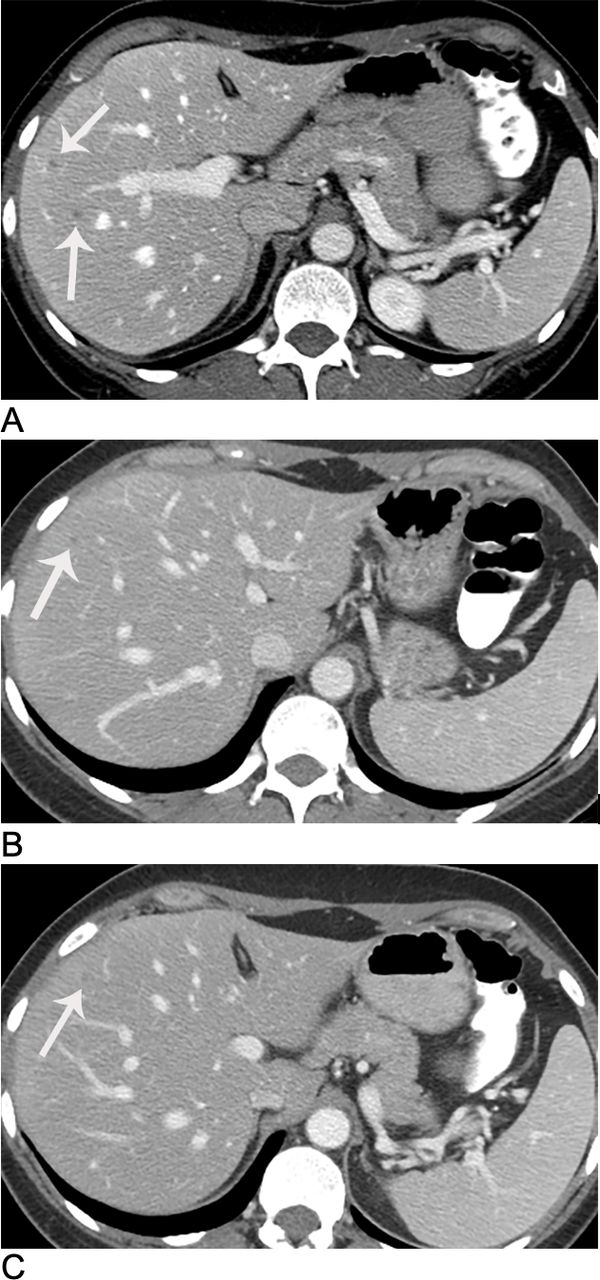 Figure 5
Figure 5 Liver metastases (arrows) after three (A), six (B), and nine (C) cycles of chemotherapy.
A CT scan after cycle 6 showed no evidence of metastatic disease in the chest. Previously identified hepatic metastatic lesions were stable ( Figure 5B). After cycle 9, the CT scan showed stable small low density lesions in the liver consistent with stable or treated metastases with no new or enlarging liver lesions. No enlarging nodules or masses were present to suggest pelvic recurrence ( Figure 5C)
Dr Frumovitz: What is the Evidence in the Literature as to the Best Systemic Therapy for Recurrent Cervical Neuroendocrine Carcinoma?The National Comprehensive Cancer Network guidelines have no specific recommendations for patients with recurrent neuroendocrine carcinoma of the cervix, but for small cell lung cancer patients who recur >6 months from completing upfront therapy with platinum and etoposide, they recommend rechallenging with that regimen. We have adopted this approach into our treatment decision making. For those who recur <6 months from completing or progress on platinum and etoposide, we typically move to the three drug regimen of topotecan, paclitaxel, and bevacizumab. The rationale and evaluation of this regimen for women with neuroendocrine cervical cancer has been published elsewhere. This regimen has been shown to improve progression free survival and the percentage of patients alive at 12, 24, and 36 months. Overall survival is also improved but it does not reach statistical significance.11
After 12 cycles of topotecan, paclitaxel, and bevacizumab, a PET-CT scan showed evidence of progressive disease.
Dr BhosaleThere was interval development of bilateral hilar adenopathy and a nodule in the right lower lobe adjacent to the hilum, measuring at least 1.6 cm. A left hilar nodal mass measured 1.9×1.8 cm. Confluent right hilar nodal mass measured 1.9×1.4 cm. Post radiation changes were identified in the pelvis. No enlarged lymph nodes were seen in the abdomen or pelvis.
Dr RamalingamCytology image guided fine needle aspiration showed tumor cells with high nuclear cytoplasmic ratio and stippled chromatin, consistent with metastatic high grade neuroendocrine carcinoma, small cell type.
Dr Frumovitz: What are the Treatment Options or Recommendation for Second Recurrence and Beyond?There are very few options for patients who progress on topotecan, paclitaxel, and bevacizumab. Molecular testing may open some options for clinical trials or off-label prescribing of targeted therapies. Studies have shown that neuroendocrine cervical cancer tumors may harbor mutations in PIK3CA, KRAS, PTEN, and p53, among others. 10 12 There are case reports showing good response to targeted therapies based on molecular testing.13
In addition, there are also case reports showing responses to immunotherapy. One case report showed a complete response to single agent nivolumab 14 However, our phase II basket trial of single agent pembrolizumab in rare tumors showed no responses in six patients with cervical neuroendocrine tumors. 15 Another case report detailed a complete response to the combination of nivolumab and ipilimumab. 16 In addition, a phase II basket trial of the same combination in patients with high grade extrapancreatic neuroendocrine tumors showed an overall response rate of 44%. 17 This study included three patients with high grade neuroendocrine carcinoma, one of whom had a partial response. These data support additional evaluation of dual cytotoxic T lymphocyte associated protein 4 (CTLA-4) and programmed cell death 1 (PD-1) inhibition as a potential therapeutic option for women with high grade neuroendocrine cervical cancer.
The patient was enrolled on a phase II trial of single agent AK104 (Cadonilimab), a human immunoglobulin G1 monoclonal antibody, that simultaneously binds to human PD-1 and CTLA-4 (NCT05063916). Both are cell surface receptors expressed primarily on activated T cells, and block PD-1/PD-L1, PD-1/PD-L2, CTLA-4/B7-1, and CTLA-4/B7-2 interactions.
Dr FrumovitzUpfront treatment for patients with stage IVB cervical neuroendocrine carcinoma should be chemotherapy. Pelvic radiation is typically indicated for symptom control as bleeding or pain. A recent study showed improved progression free and overall survival when radiation with curative intent is added to platinum and etoposide when there is resolution of extrapelvic disease. For recurrent neuroendocrine cancer, options are scarce. A regimen including topotecan, paclitaxel, and bevacizumab has been shown to improve progression free survival. The role of immunotherapy is still undetermined.
留言 (0)